Classic Human Anatomy in Motion: The Artist's Guide to the Dynamics of Figure Drawing (2015)
Chapter 8
Body Types, Surface Landmarks, and Soft-Tissue Characteristics
This chapter begins by briefly examining three basic body types, then goes on to explore other surface form characteristics to increase your understanding of the dynamics of the human figure. Surface form landmarks include the various bony landmarks mentioned in Chapter 1, as well as soft-tissue forms that influence the surface shape, including muscles, fatty tissue, tendons, cartilages, and ligaments that collectively produce a variety of eminences, depressions, furrows, creases, and folds in the skin throughout the body.
During certain actions, some soft-tissue landmarks may be quite noticeable, becoming harder to detect when the body or body part changes position. When drawing the figure, it is not necessary to include every surface characteristic you see in each pose. You may choose to emphasize, downplay, or edit surface landmarks depending on your interpretation and on the movement or feeling you want your drawing to convey.
Basic Body Types
The endless variation of human bodies makes the study of the figure challenging as well as captivating. People come in a wide assortment of shapes and sizes—petite, portly, slender, muscular—and all these different body shapes are influenced not only by skeletal and muscle characteristics but also by the subcutaneous layer, which contains adipose (fatty) tissue. Among other factors contributing to differences in body shapes are genetic makeup, the aging process, and glandular influences. Alterations to the shape of the body can also result from illness, bone deterioration, and malnourishment. Some factors’ influence is inevitable, as with aging. However, the amount and distribution of fatty tissue and the tone of muscles can be changed intentionally through bodybuilding, dieting, cosmetic surgery, or disciplined training in sports, martial arts, or dance.
One system of identifying different body types that has been used for decades states that there are three basic body types—mesomorph, ectomorph, and endomorph—each with its own particular characteristics. These types are, of course, generalizations. Most people’s bodies have attributes of all three types, with one type predominating. While this system is not totally reliable and might possibly lead to stereotyping, it is useful for learning purposes.
The Mesomorph Body Type
The mesomorph has a naturally athletic build, with large bones and well-defined muscular forms. The chest tends to be wide, the neck thick, and the face angular in appearance. Basic traits of the mesomorph—male and female—are shown in the drawing on this page.
MESOMORPH BODY TYPE
Male figure
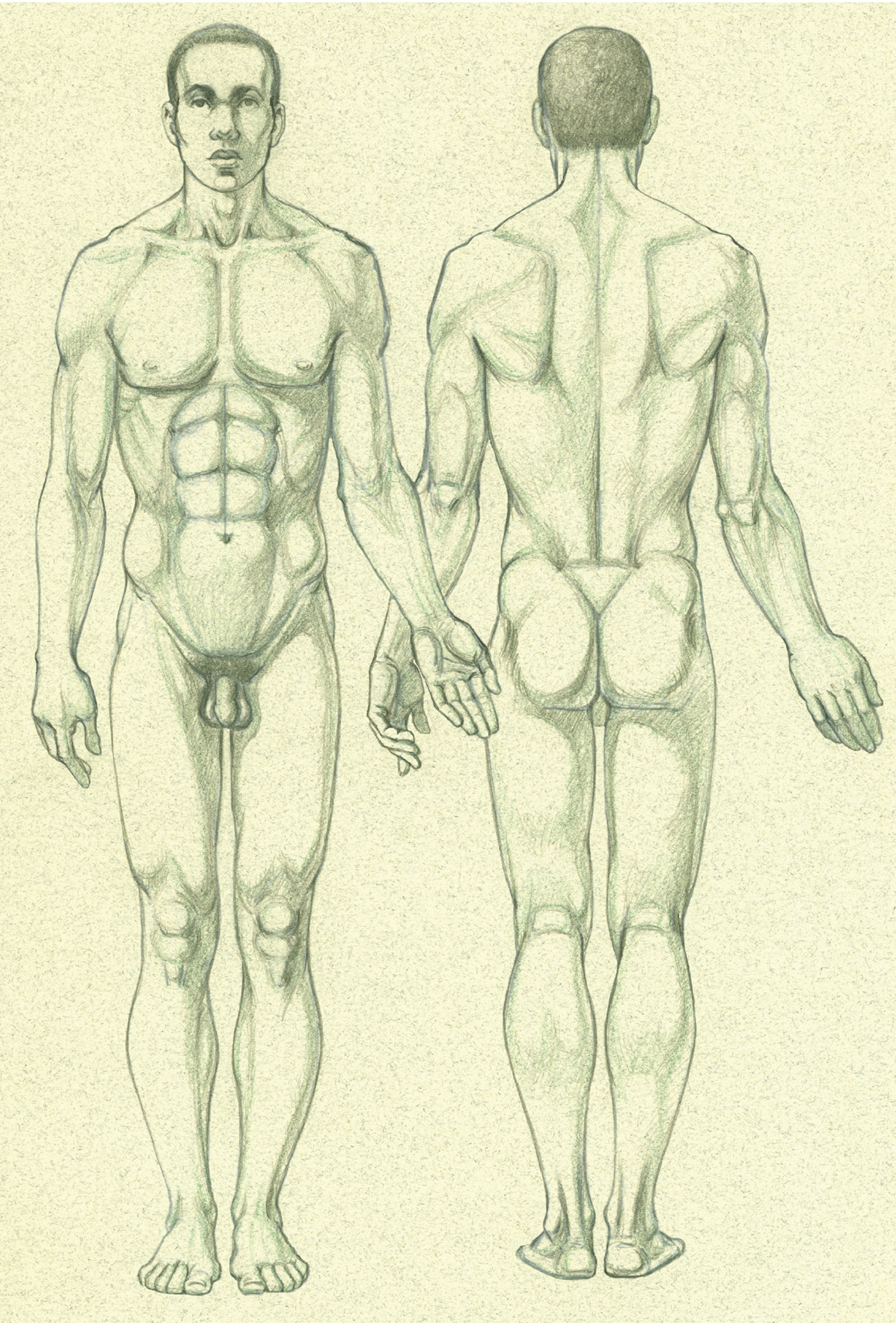
Anterior and posterior views
MESOMORPH BODY TYPE (CONTINUED)
Female figure
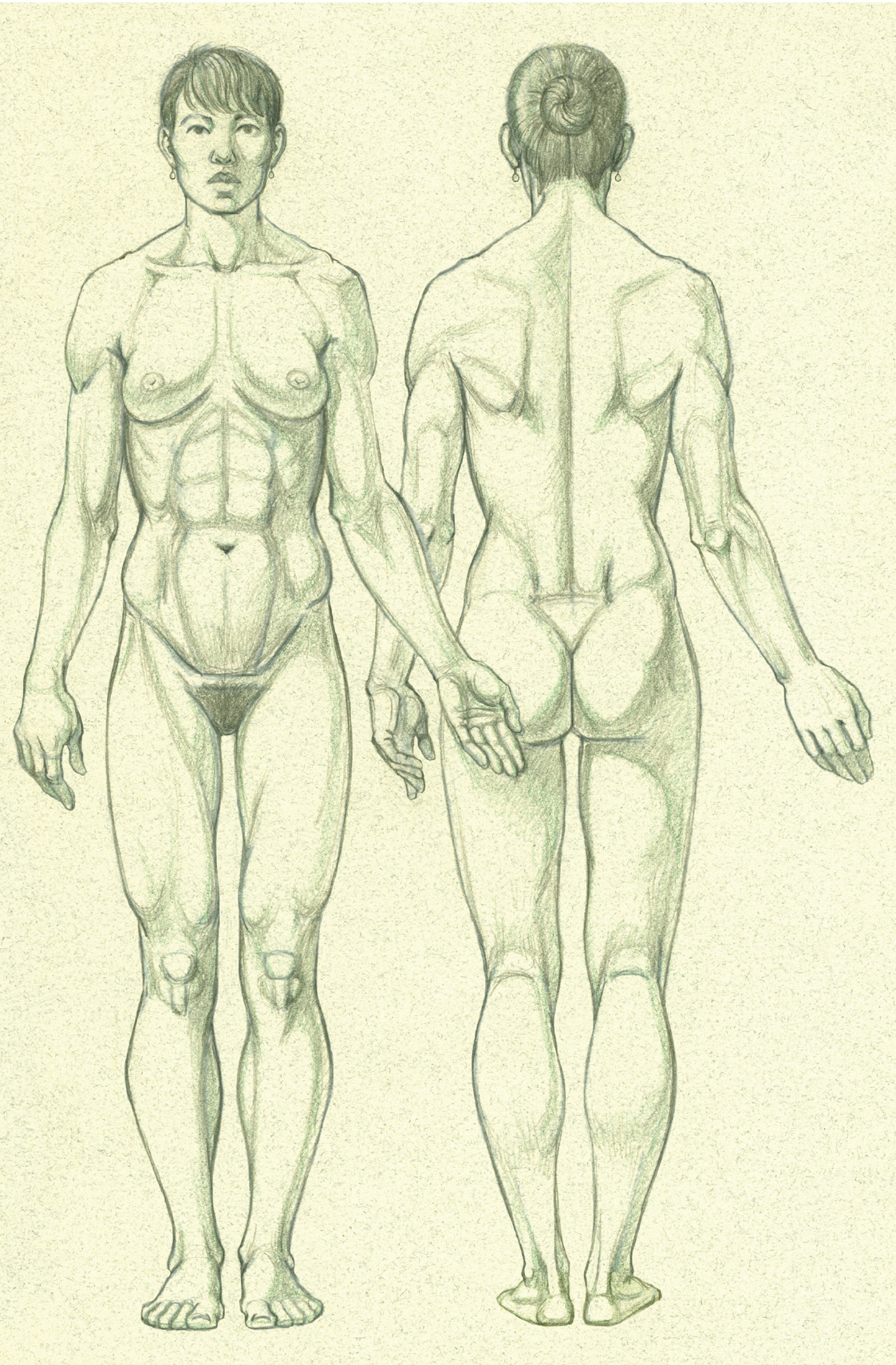
Anterior and posterior views
Among bodybuilders you see many variations on the mesomorph body type. A person who is tall and lean but has distinct muscle definition can be classified as a cross between the mesomorph and ectomorph body types (“ecto-mesomorph”). This type of physique can be described as “Apollonian,” after the typical depiction of the god Apollo in Greco-Roman art. A physique combining mesomorph and endomorph traits (“endo-mesomorph”), with exaggerated muscular definition, might be called “Herculean,” after depictions of the mythic hero Hercules.
The Ectomorph Body Type
The ectomorph is slender and delicate in appearance. An ectomorph’s bones are fairly noticeable on the surface form because of the relative lack of fatty tissue. Some ectomorphs have lean but apparent muscles, while others, who are not muscular, have a somewhat flaccid look. The upper body tends to be short, with a narrow rib cage, pelvis, and shoulders, while the limbs, hands, face, and neck are usually long and thin. There is always some amount of adipose tissue in the subcutaneous layer, even on exceedingly thin people, but if this layer becomes extremely diminished, the ectomorph’s body may look malnourished or anorexic. Basic traits of the ectomorph—male and female—are shown in the following drawings.
ECTOMORPH BODY TYPE
Male figure
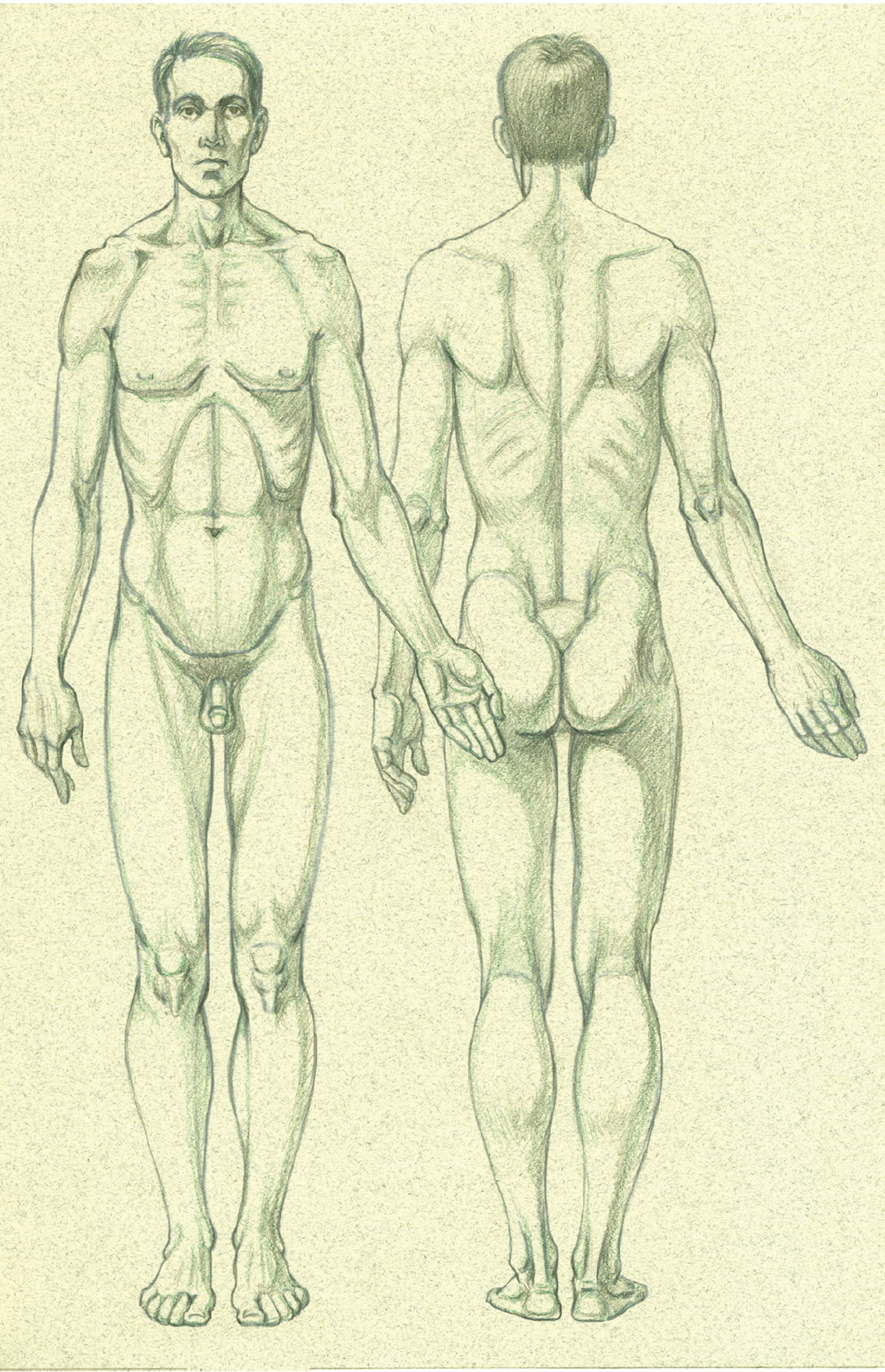
Anterior and posterior views
ECTOMORPH BODY TYPE (CONTINUED)
Female figure
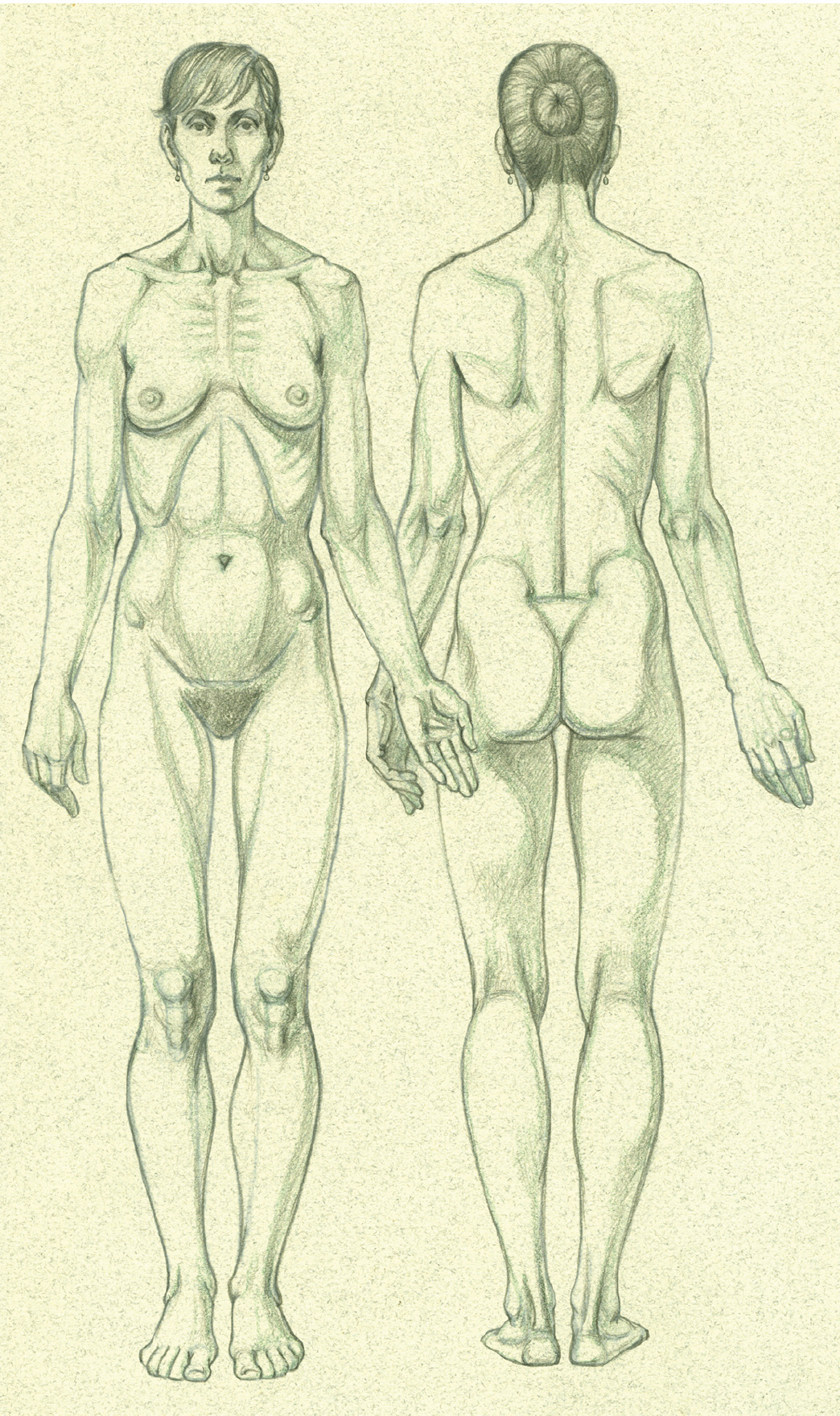
Anterior and posterior views
The Endomorph Body Type
The endomorph body type covers a wide variety of subtypes, from slightly plump, to portly, to obese. The fatty tissue throughout the body is distributed differently from individual to individual, and the physical appearance of the endomorph’s torso can range from a large bulbous shape with normal hip size (referred to as an “apple-shaped” body) to a “pear shape” caused by the accumulation of fatty tissue primarily on the abdomen, hips, and buttocks. The limbs in the endomorph type are usually thick, but the wrists and ankles may appear lean since fatty tissue does not normally accumulate in these regions unless the person is severely obese. The face is characteristically round with a short, bulky neck. Hands and fingers will appear thick and slightly pudgy, while the feet tend to broaden due to the excess weight bearing down on the supporting arches of the feet. Basic traits of the endomorph—male and female—are shown in the following drawings.
ENDOMORPH BODY TYPE
Male figure
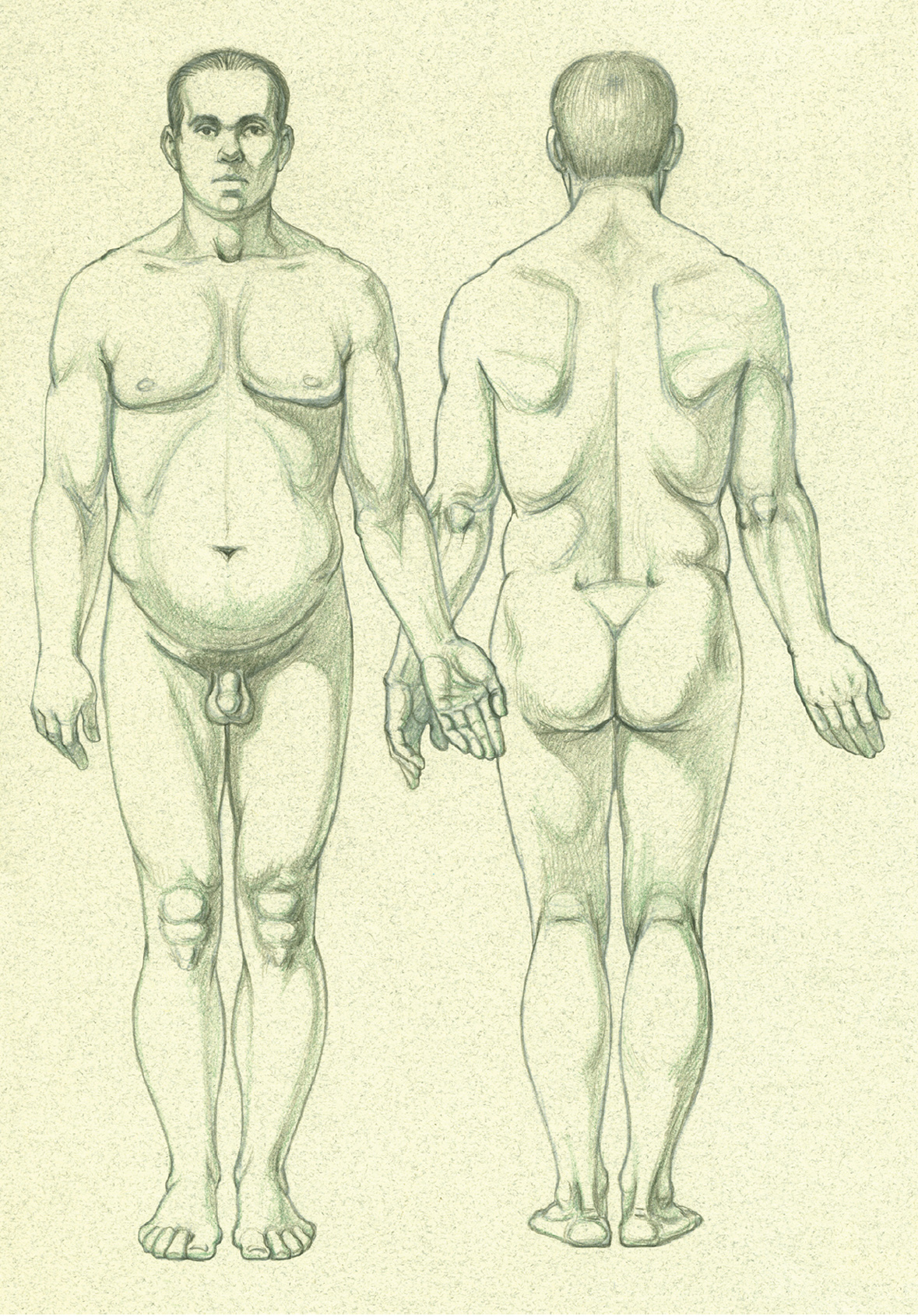
Anterior and posterior views
ENDOMORPH BODY TYPE (CONTINUED)
Female figure
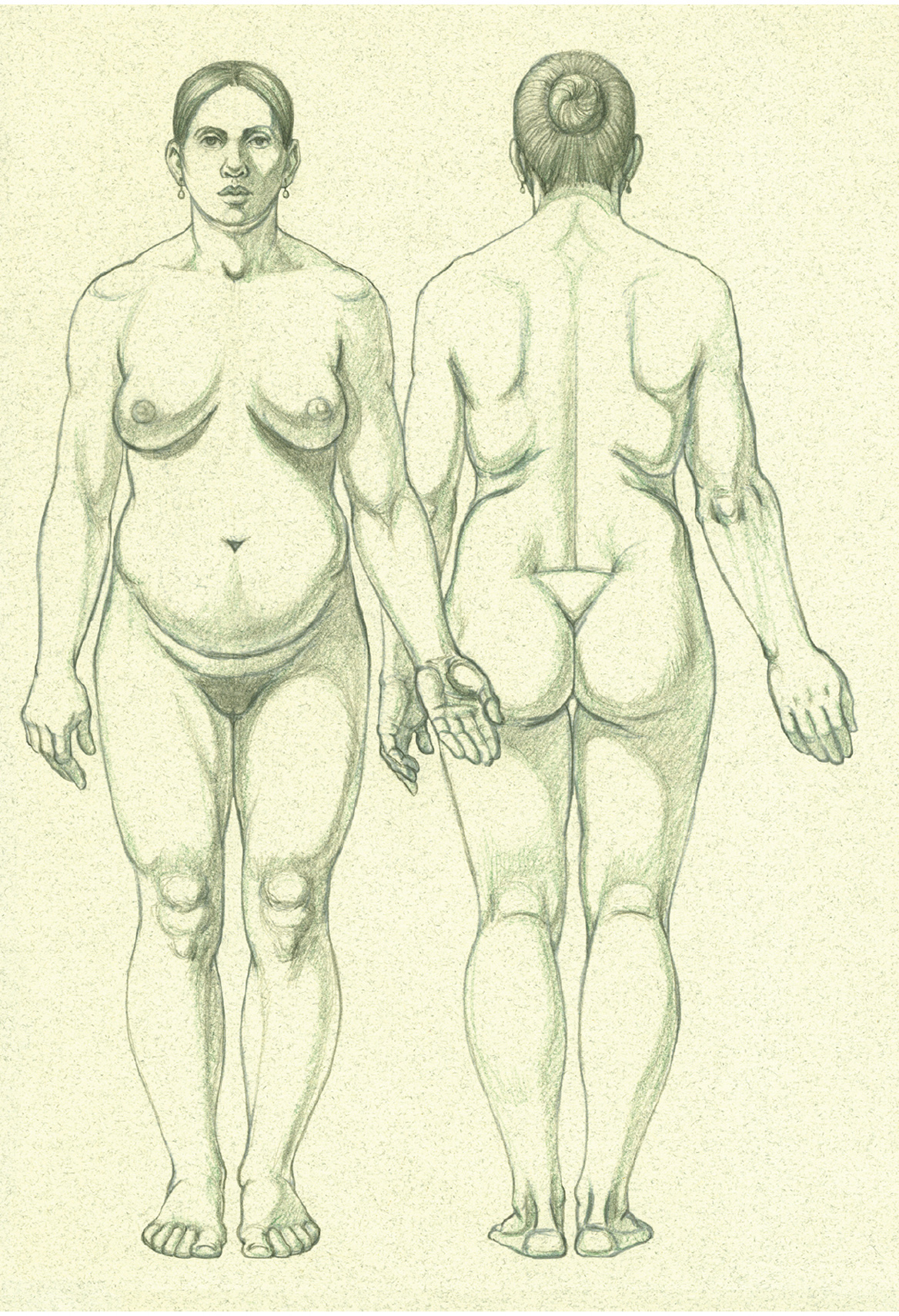
Anterior and posterior views
Surface Form Landmarks
We will now take a closer look at the various landmarks seen on the body surface, including key bony landmarks that make important contributions to the surface form. Fatty tissue’s extensive influence on surface form will be examined in more detail in the following sections.
Landmarks of the Head and Neck
We begin this section with front and side views of the male and female head, opposite and below, which identify the basic surface form landmarks, including key bony landmarks. When depicting a face realistically, always be aware of the general shape of the cranium. Although hair might obscure most of the skull’s ostrich-egg shape (see this page), you should always indicate the general width and height of the head as you are setting up the facial forms. And always remember that although the facial bones are covered by muscles and a layer of soft subcutaneous tissue, they importantly serve as the bony scaffolding for the facial muscles. Connective-tissue structures such as the cartilage of the nose and ear and the softer-tissue forms of the lips and eyes are easily seen.
SURFACE FORM LANDMARKS OF THE HEAD AND NECK—MALE AND FEMALE
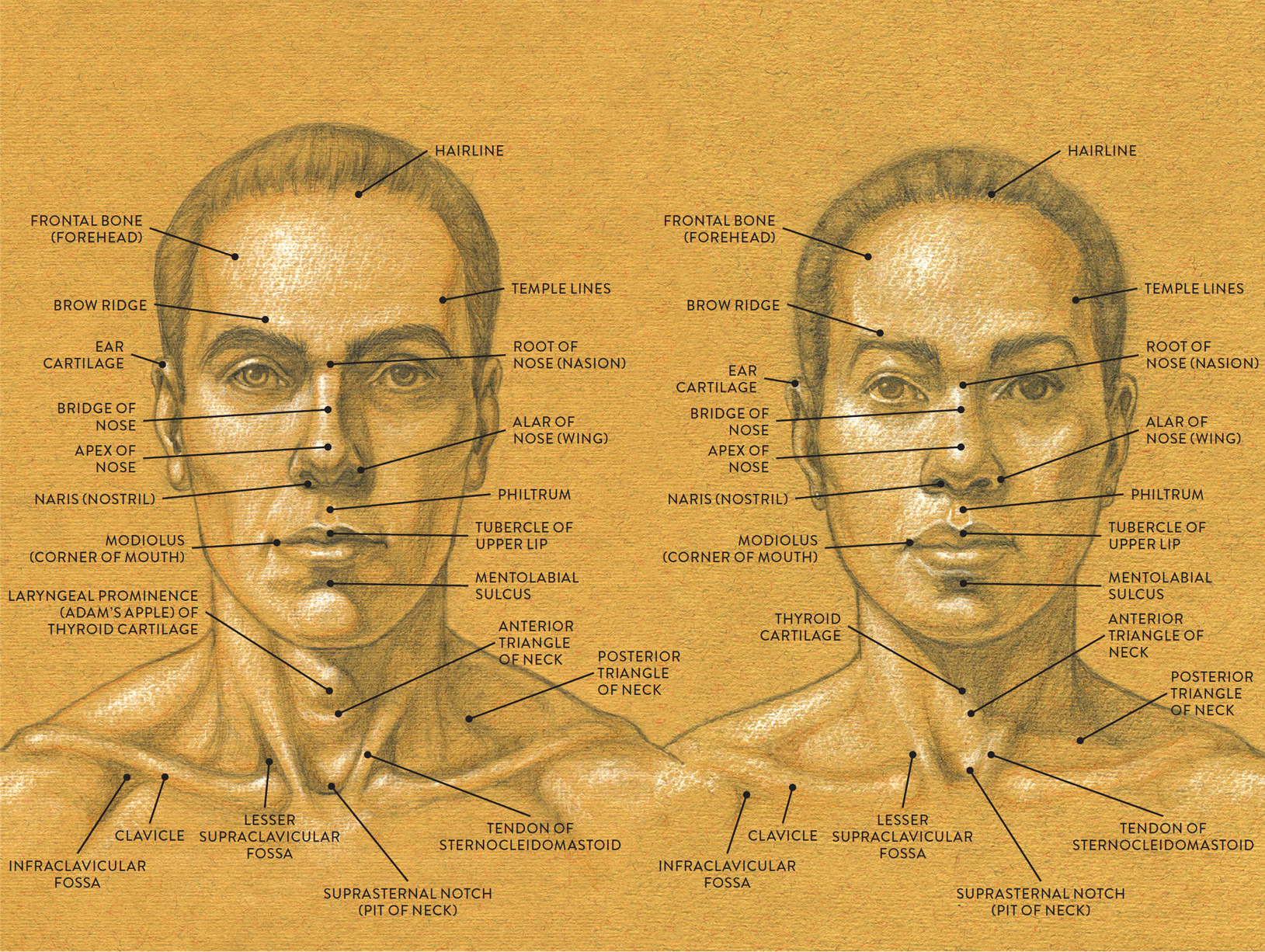
LEFT: Male head, anterior view
RIGHT: Female head, anterior view
SURFACE FORM LANDMARKS OF THE HEAD AND NECK—MALE AND FEMALE
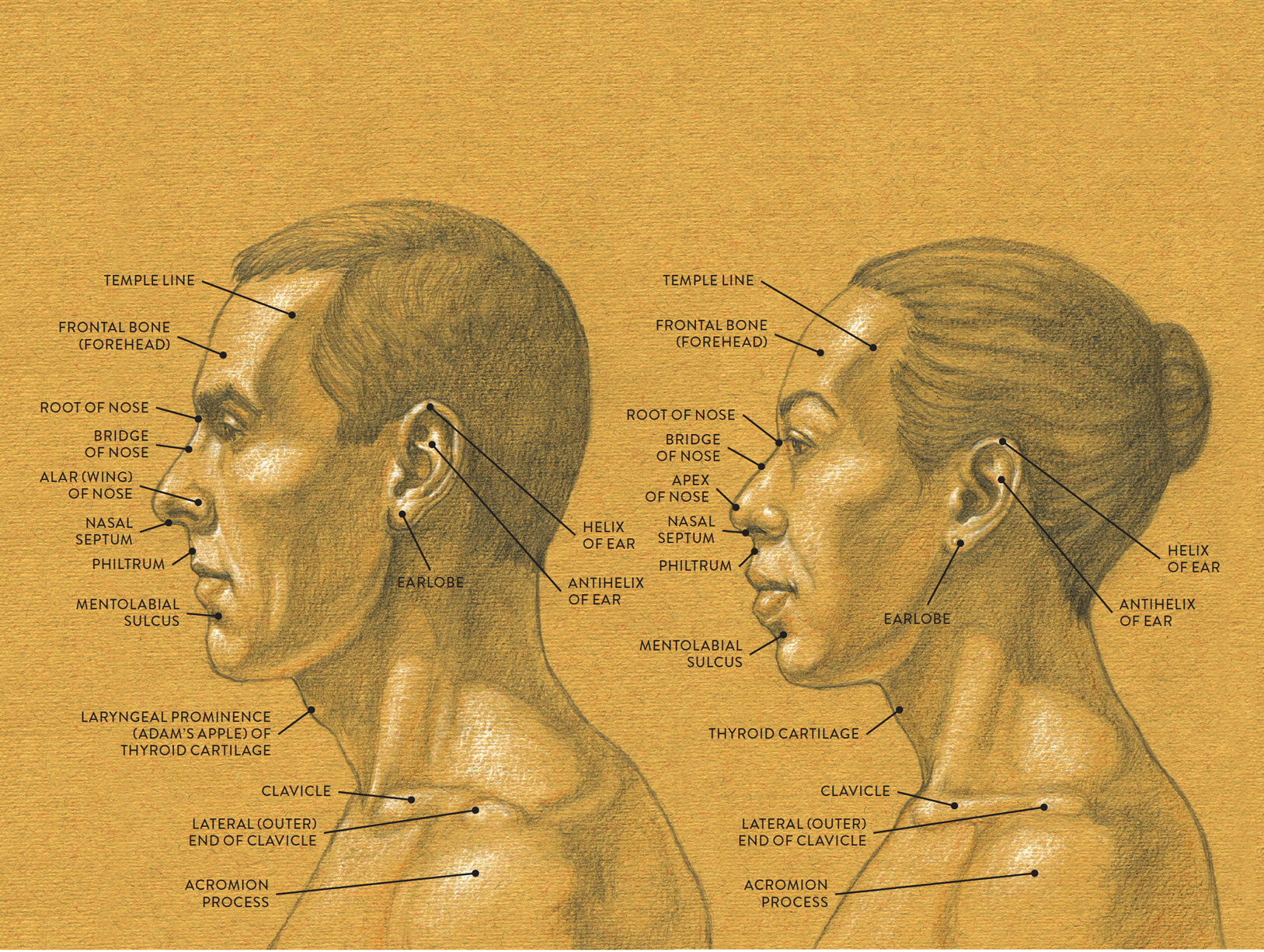
LEFT: Male head, lateral view
RIGHT: Female head, lateral view
Landmarks of the Eye Region
The spherical shape of the eye is suspended within the orbit (eye socket) by a series of thin muscles and cushioned by orbital fat. Attaching on the outer rim of the orbit is a thin membrane-like sheathing called the orbital septum, which inserts into the eyelids. Positioned over the orbital septum is the orbicularis oculi muscle.
There are many subtle variations on the way the eyelids wrap over the front portion of the eyeball, depending on whether the fat pads surrounding the eye influence the lids. In some eyes there is a crease above and parallel to the curve of the eye. Identified as the back-of-the-eye crease, it can be a subtle crease or a deep fold. As the upper lid closes, the back-of-the-eye crease temporarily disappears, returning when the lid opens. Other eyes have a different type of upper-lid structure, called an epicanthic fold. It falls close to the edge of the upper lid and partially covers the inner corner of the eye. As a result, there is no strong crease at the upper back portion of the eye. Fatty tissue pads soften the region of the upper and lower lids. There are countless variations of these eye folds throughout the world.
TWO TYPES OF EYE FOLDS
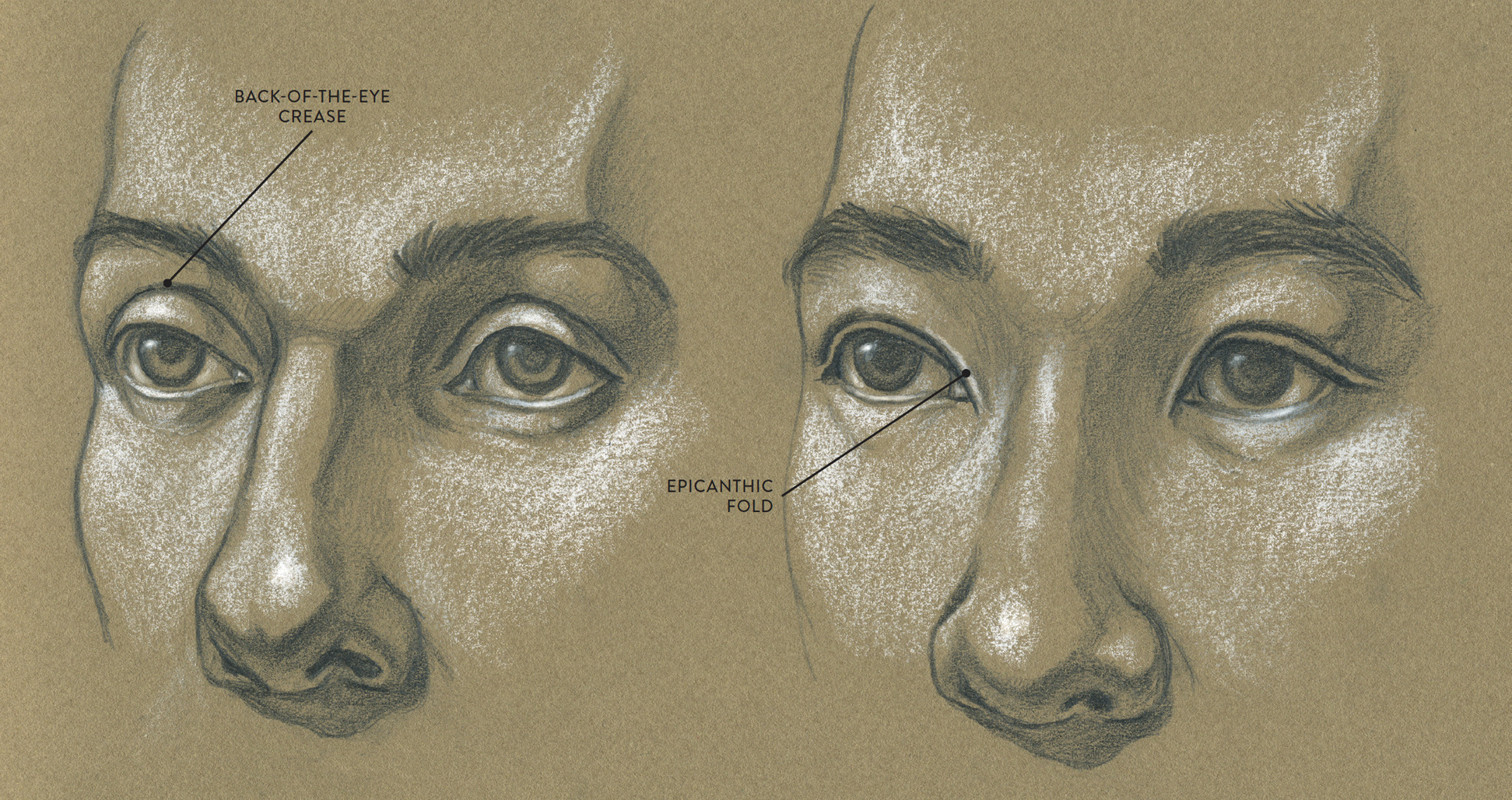
LEFT: This fold parallels the upper curve of the eye.
RIGHT: This fold is close to the edge of the upper lid, partly covering the inner corner of the eye.
The inner corner of the eye, called the medial angle of the eye, has an extremely small triangular depression containing a pink fleshy structure called the lacrimal caruncle. The outer corner of the eye, where the upper and lower lids meet, is called the lateral angle of the eye.
The iris is the colored disc of the eye. Irises come in various shades of brown, green, blue, and gray, with some eyes containing a mixture of brown and green pigments, producing hazel-colored eyes. At the center of the iris is the pupil, an aperture that fluctuates in size (see this page).
Landmarks of the Nose
The nose structure essentially consists of the nasal bone and the nasal cartilages. The immense variation in nose shapes is caused by differing shapes of the nasal bone and cartilages, as well as differing widths of the nasal cavity.
The nose begins between the eyes at what is called the root of the nose (nasion). The top plane of the nose is referred to as the dorsum of the nose or bridge of the nose. If the nasal bone is positioned at an acute angle, the bridge of the nose will be more pronounced, possibly with a subtle or prominent bump at the transition between the nasal bone and the cartilage. If the nasal bone is flatter, then the bridge of the nose will be lower, generally with a smoother transition between the nasal bone and the cartilage.
Along the midline of the nose is the septal cartilage, which also acts as a partition within the nasal cavity. The nasal septum, a continuation of the septal cartilage, is seen as the soft-tissue structure between the nostrils (sing., naris; pl., nares).
The lower part of the nose is constructed of cartilages and soft-tissue forms. The lateral nasal cartilage is attached to each side of the nose; the greater alar cartilage creates the general shape of the tip of the nose (apex of the nose). The characteristics of this cartilage vary: The tip of the nose can be small, large, spherical, angular, wide, or narrow and can point upward or droop downward.
The wings of the nose (alar of nose) are composed of fibrous connective tissue and fatty tissue surrounding each nostril. Some noses have a wide nasal cavity, producing a broader nose in which the wings of the nose are farther apart. A smaller nasal cavity produces a narrower nose, with the wings of the nose closer together. Smaller cartilages, called the lesser alar cartilage, are situated near or on the wings of the nose but are usually not detected on the surface form.
Between the nasal septum and the upper lip is a vertical, trenchlike depression in the skin called the philtrum. Depending on the space between the bottom of the nose and the upper lip, the philtrum can be long or short. Also, the shape of the upper lip can influence the width of the philtrum, making it narrower or wider.
Landmarks of the Mouth Region
The upper and lower lips are actually part of the orbicularis oris muscle. Lips can vary in size and shape depending on the relationship between the upper and lower dental arches, the positions of the maxilla and mandible, and the placement of the teeth. The upper and lower lips can be thick, curving, and sensuous or thin, angular, and tense. They can also be wide or narrow, projecting or receding.
At the center of the upper lip a small projection called the tubercle of the upper lip. It contains a small amount of fatty tissue that helps create its shape. This tubercle can be quite prominent or very subtle.
At each corner of the mouth is a small mound in the skin called the modiolus. Several facial muscles insert here. Fatty tissue gives the modiolus a slight bulge, sometimes creating a small fold in the skin.
Surrounding both the upper lip and lower lip, at the vermillion border of the lips, is a thin ridge consisting of fibrous connective tissue called the lip rim. It usually catches highlights, making it easier to see against the darker pigment of the lips.
On a relaxed face, the nasolabial fold is a soft plane change near the outer wing of the nose and the outer edge of the orbicularis oris muscle. When a person smiles or laughs this furrow lengthens and can become an obvious semicircular fold in the skin (see this page). As a face ages, this fold transforms into a noticeable permanent crease that descends in a curving alignment from the wing of the nose toward the outer corner of the mouth.
Positioned immediately below the lower lip and above the chin region is a small indentation in the skin called the mentolabial sulcus, which simply means “furrow between the lip and chin.” This depression can be obvious, especially if the lower lip is full and prominent, or shallow if the lower lip is rather thin.
The following life study shows many of the landmarks of the eye region, nose, and mouth region; the accompanying anatomical study reveals the structures beneath the skin.
LANDMARKS OF THE EYE REGION, NOSE, AND MOUTH REGION
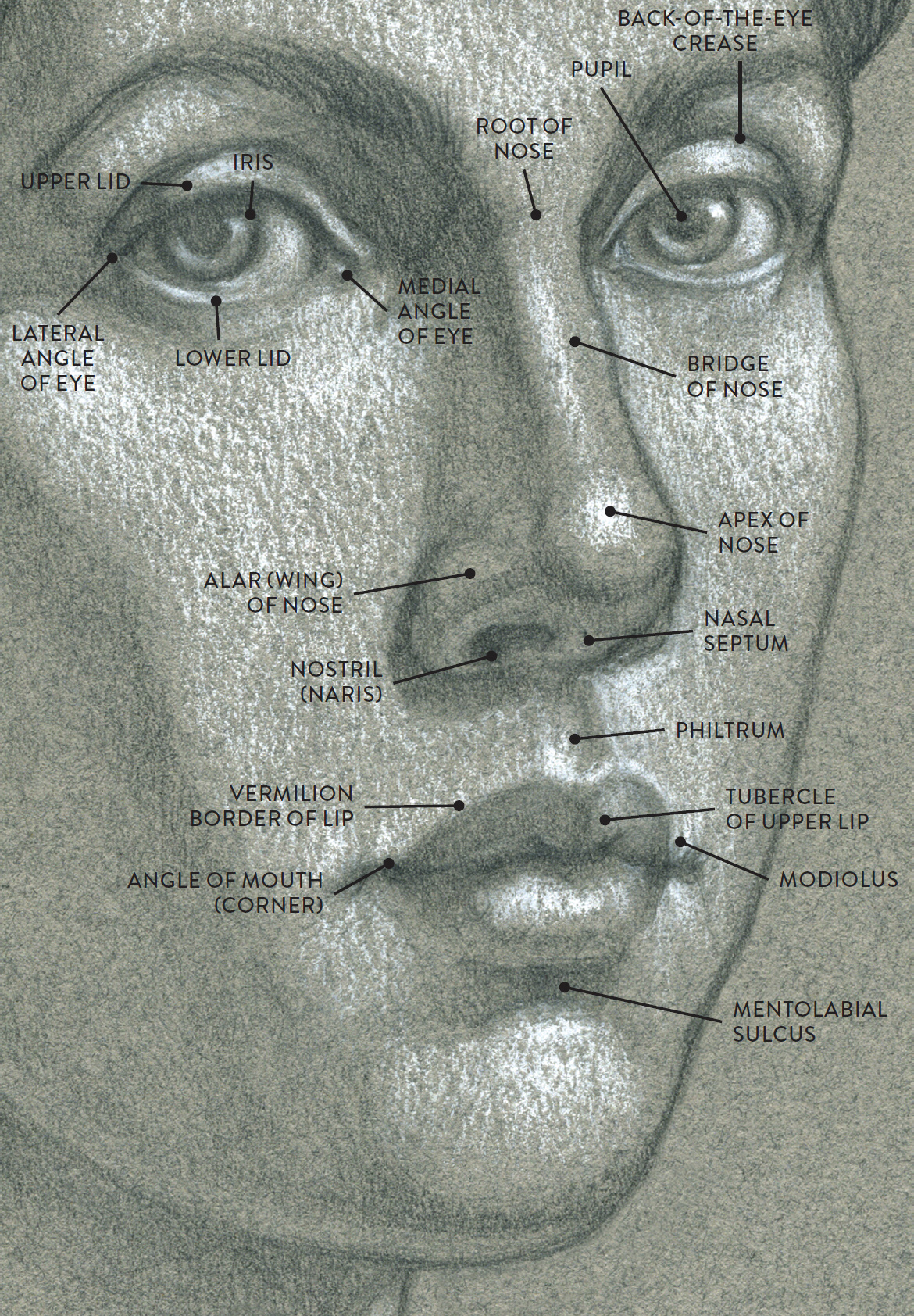
Life study of face in cropped three-quarter view
LANDMARKS OF THE EYE REGION, NOSE, AND MOUTH REGION
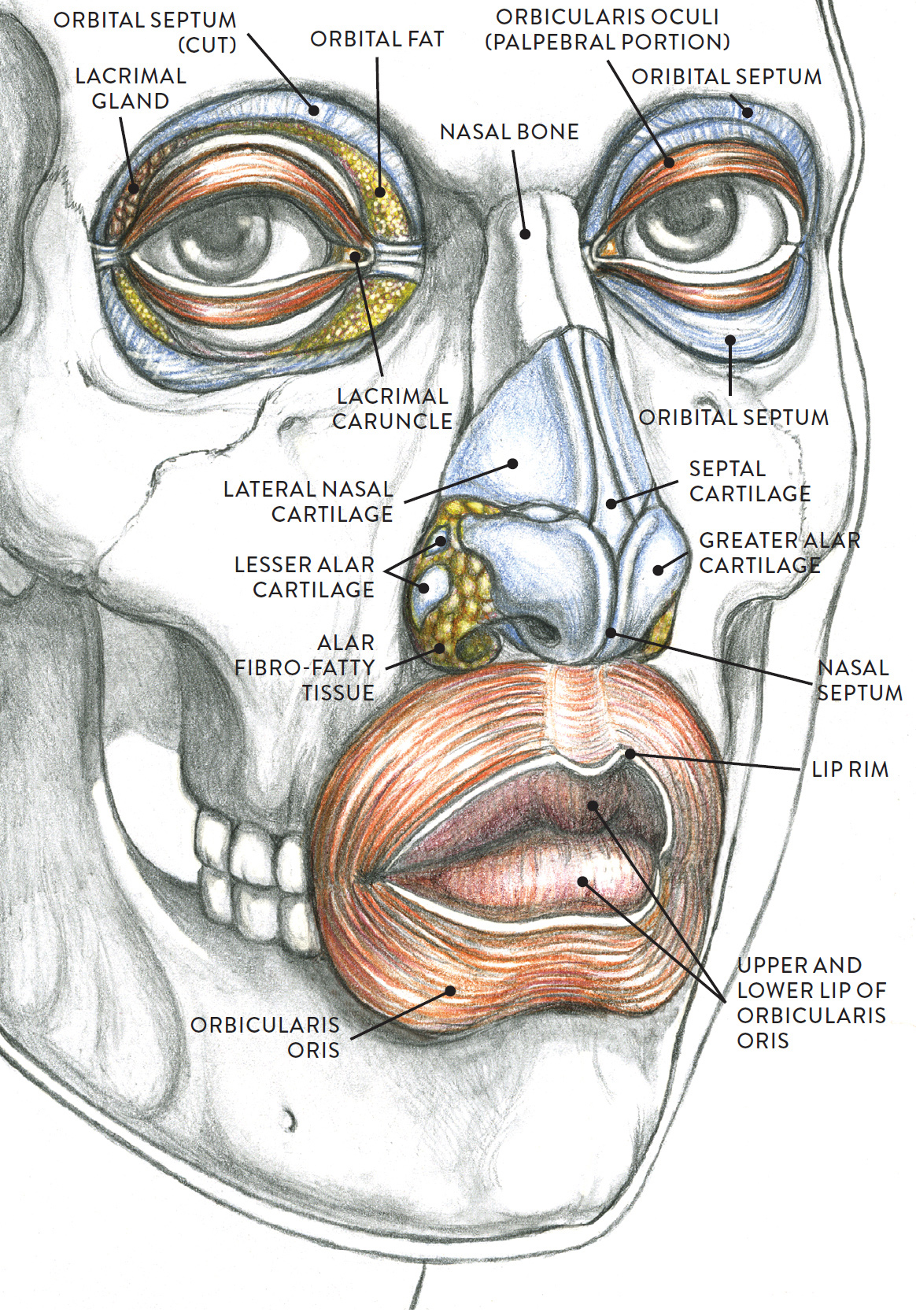
Anatomical study
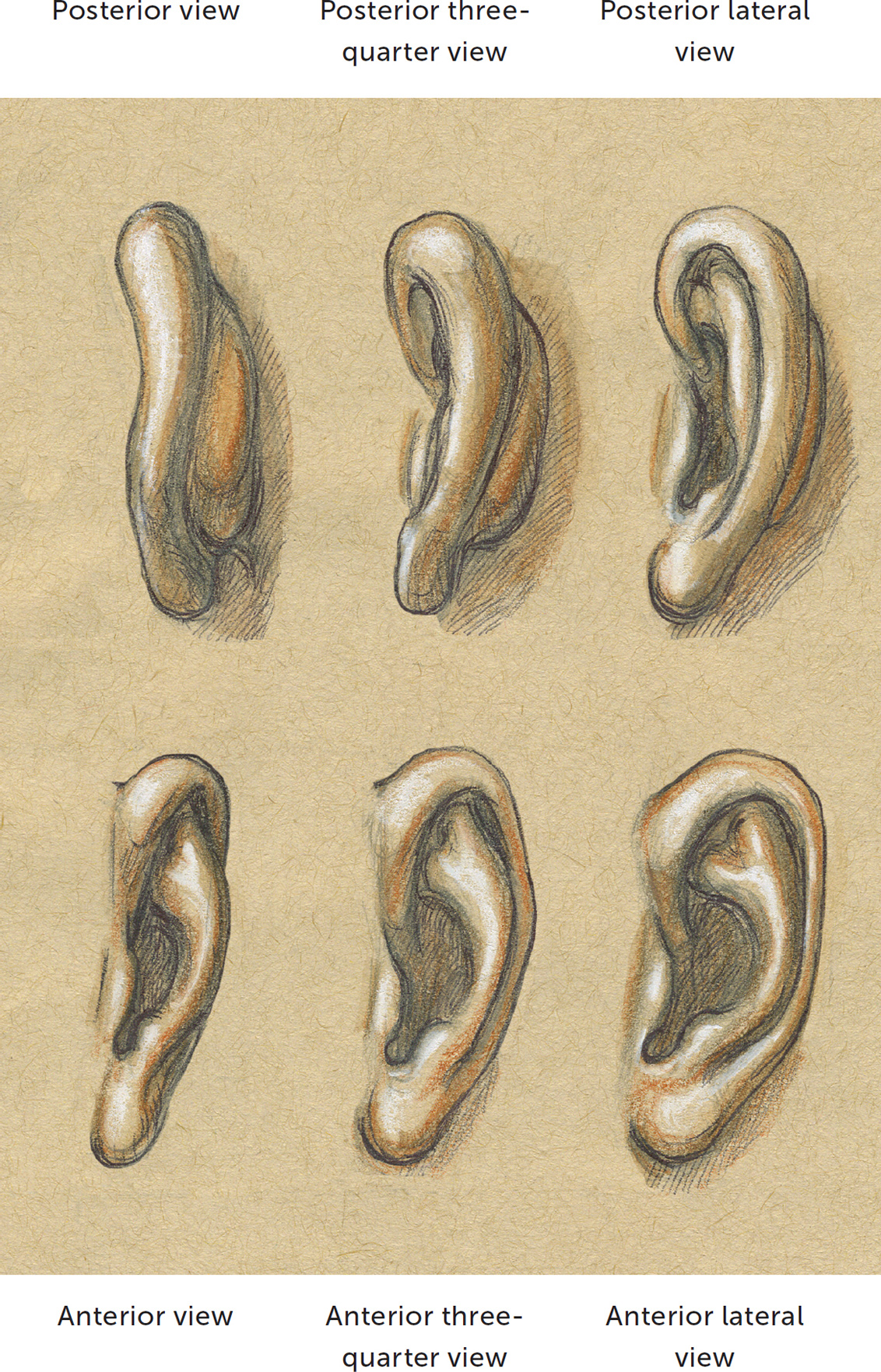
Landmarks of the Ear
Ears can lie snugly against the head or project outward. They can be small or large, angular or curved. Their tubular forms can be thick or delicate. The ear structure is comprised mainly of cartilage, while the earlobe contains fibrous fatty tissue.
The form of the ear is convoluted, consisting of a bowl-like structure, called the concha, and spiraling tubular forms attaching around and within the bowl. The outer tubular rim is called the helix, and the inner tubular rim is called the antihelix. As the antihelix sweeps toward the ear lobe a small bump called the antitragus is seen. In front of the ear canal (external auditory meatus) is a small protruding (though somewhat flattened) cartilage form called the tragus. Between the tragus and antitragus is the ear notch.
FORMS OF THE EAR, AND ITS PLACEMENT ON THE CRANIUM
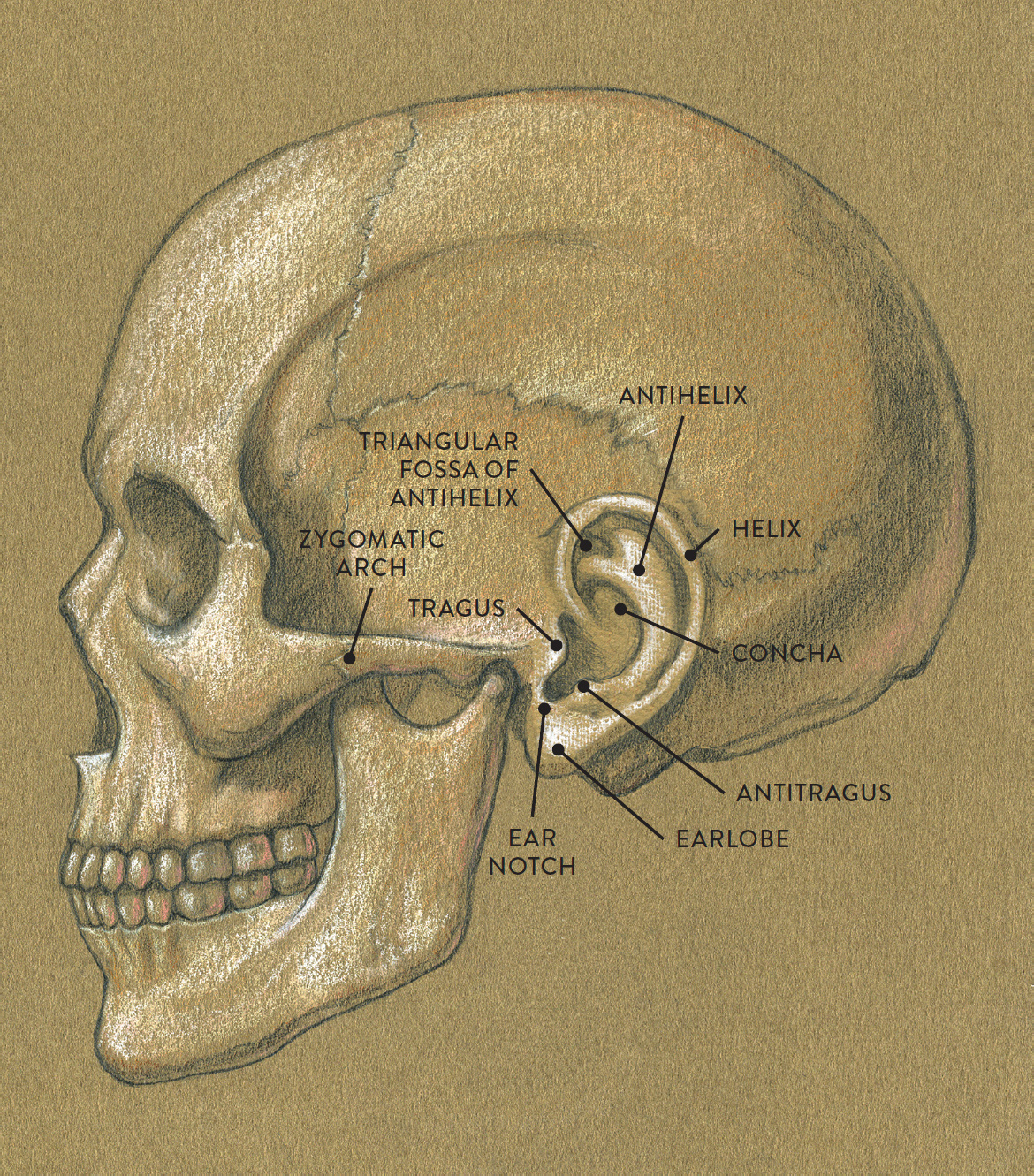
Lateral view
The earlobes are made not of cartilage but of fatty and fibrous tissue. On some ears the lobes can hardly be detected, while in others they have an obvious fleshy shape. Some earlobes can be quite prominent, appearing as large hanging flaps. This can result from the aging process or from the lobe’s being stretched by heavy earrings or disc-like plugs (gauges) inserted in the lobe.
The ear is positioned over the ear canal at the end of the zygomatic arch. The drawing at left shows the ear’s placement on the cranium (as seen from the side), as well as its various forms. The following study Views of a Left Ear, shows how dramatically the ear changes shape when viewed from various perspectives.
VIEWS OF A LEFT EAR
Hair Characteristics
The hair is part of the integumentary (skin) system, because hair follicles (the bulblike forms that produce individual hairs) are located in the epidermis and dermis layers of the skin.
Depicting Hair
The shape, texture, and growth pattern of hair are essential elements for figurative artists to consider. The style of a person’s hair can, after all, be part of his or her unique character or identity (think, for example, of Albert Einstein, Princess Diana, Elvis Presley, or Bob Marley).
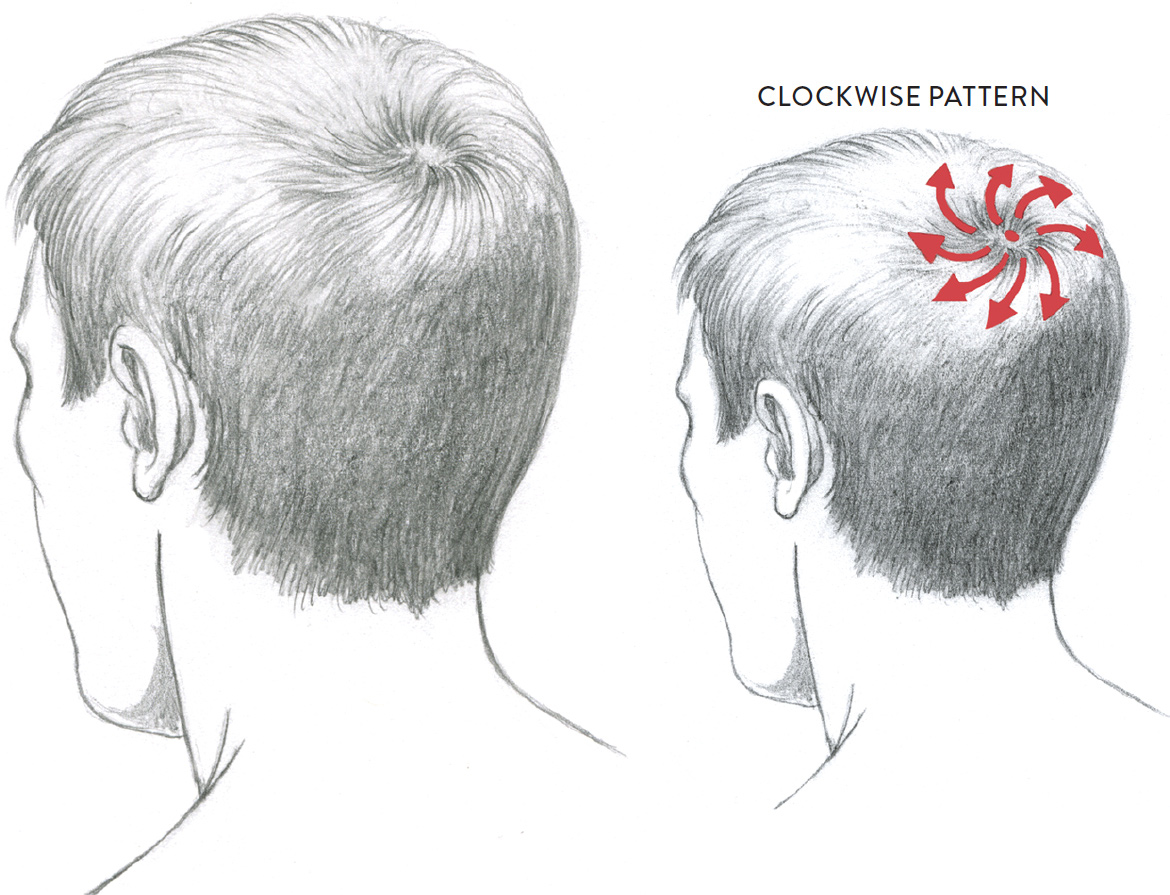
Hair emerging from the scalp creates a border, called the hairline, around the upper face, swinging around the ears and the back of the neck (nape). Hair growth patterns include the hair whorl, located toward the upper back portion (the crown) of the head. The hair whorl, shown in the following drawing, usually appears as a vortex of hair growing in a swirling, circular motion, either clockwise or counterclockwise. Some people have a reversed tuft of hair emerging upward from the center of the hair whorl, commonly called a cowlick.
STUDY OF A HAIR WHORL
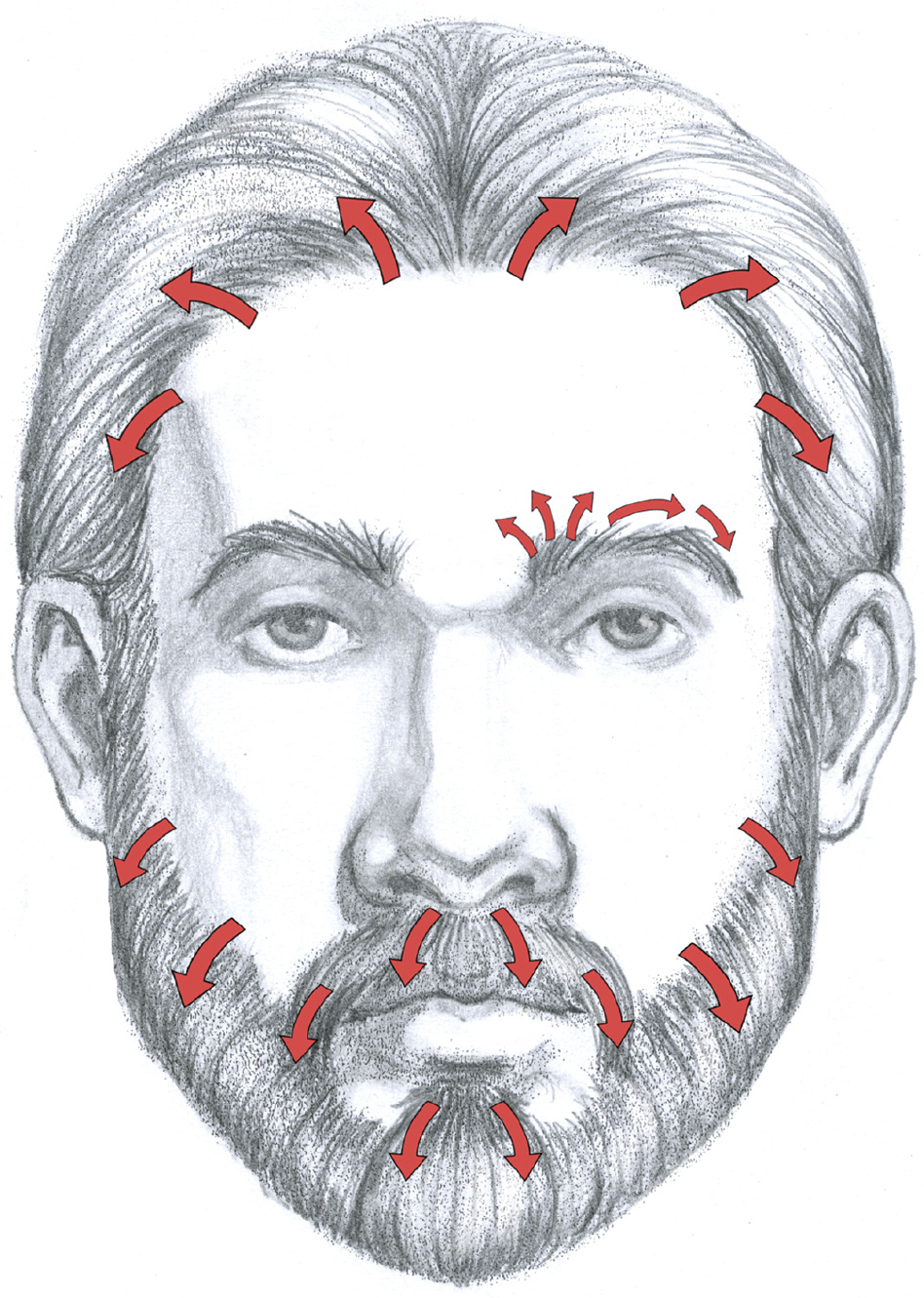
As with the hair of the head, the growth patterns of facial hair—eyebrows, sideburns, mustaches, beards—are directional, as shown in the next drawing. Indicating this directionality is essential to an accurate depiction.
DIRECTIONAL GROWTH PATTERNS FOR HAIR, EYEBROWS, AND BEARDS
Most hair stylists agree that there are four basic hair types: wavy, curly, very curly, and straight. These four types are shown in the drawing on this page. Wavy hair has a gentle spiraling movement throughout its length. Curly hair can be somewhat tight (in ringlets) or more relaxed. When depicting curly hair, look for curl clusters—sections of hair that move in different spiraling patterns. Very curly hair grows in a tight spiraling formation. It can be braided close to the cranium, or strands of hair can be twisted together, appearing as small springy locks that gently flare outward from the head. It can also be allowed to grow naturally into elongated cylindrical coils, called locks (or locs). Straight hair can be any length, trimmed straight across or layered. Short straight hair can be spiky, flaring out from the skull; as straight hair grows longer, gravity pulls the strands downward.
BASIC HAIR TYPES
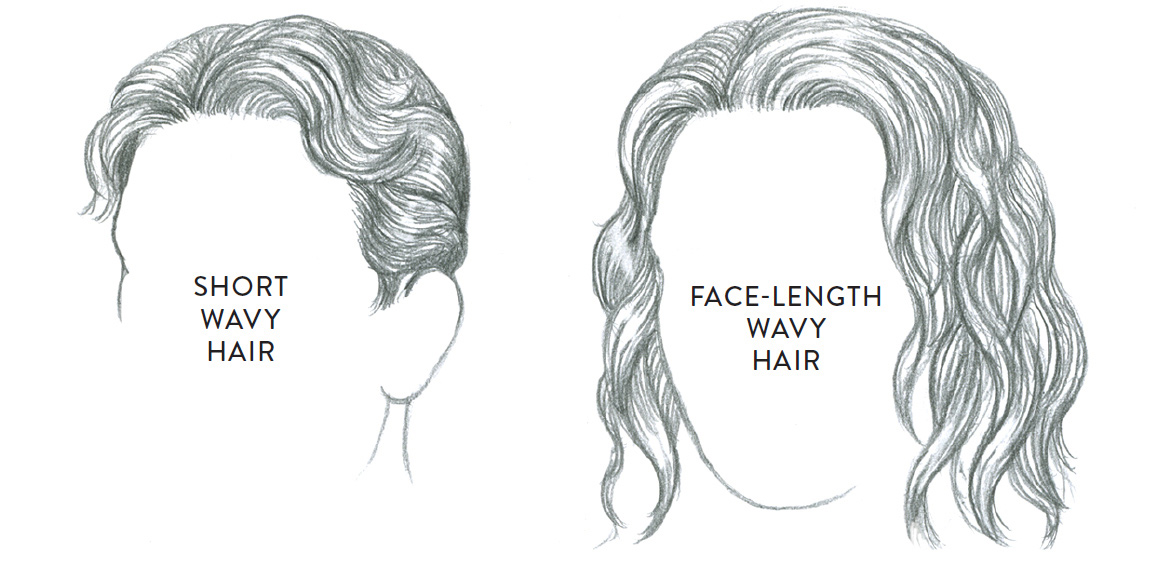
Wavy hair
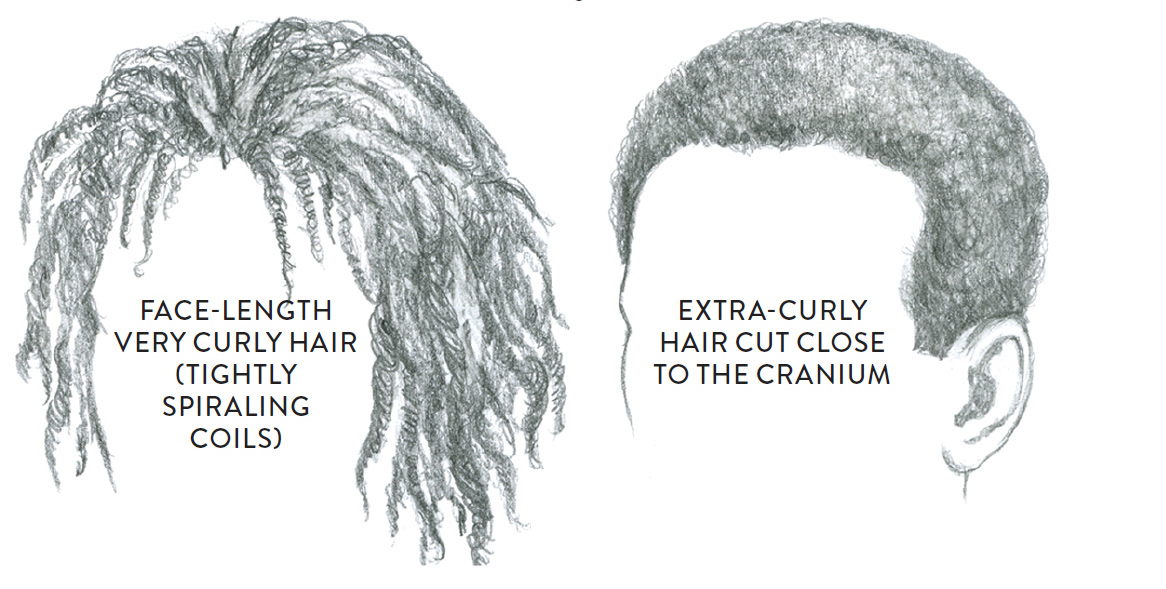
Very curly hair
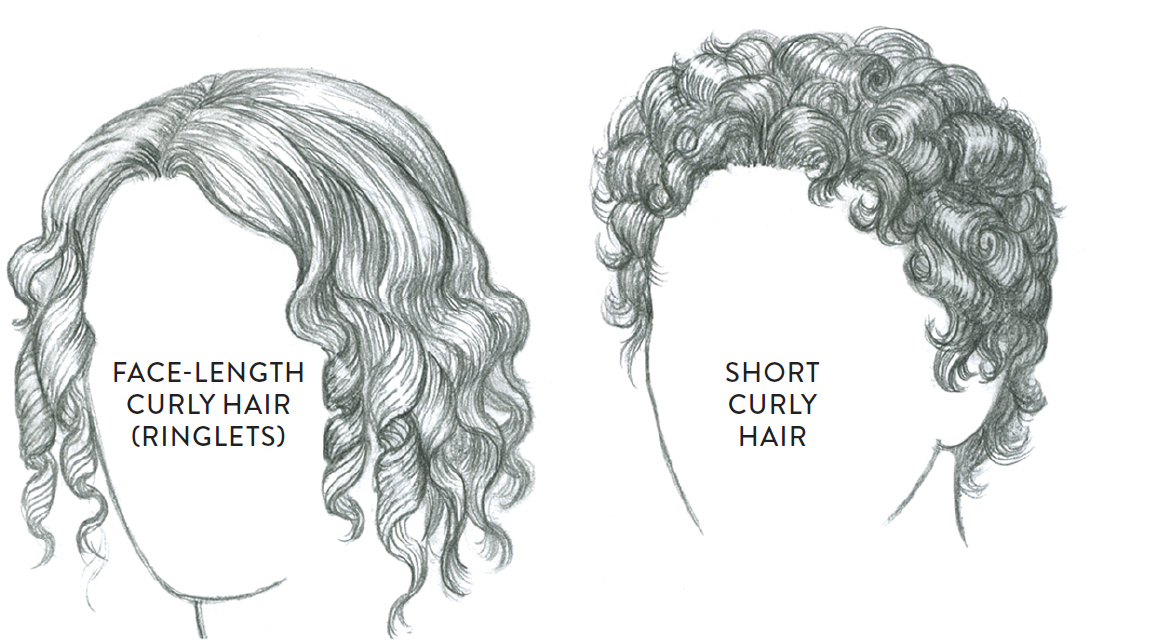
Curly hair
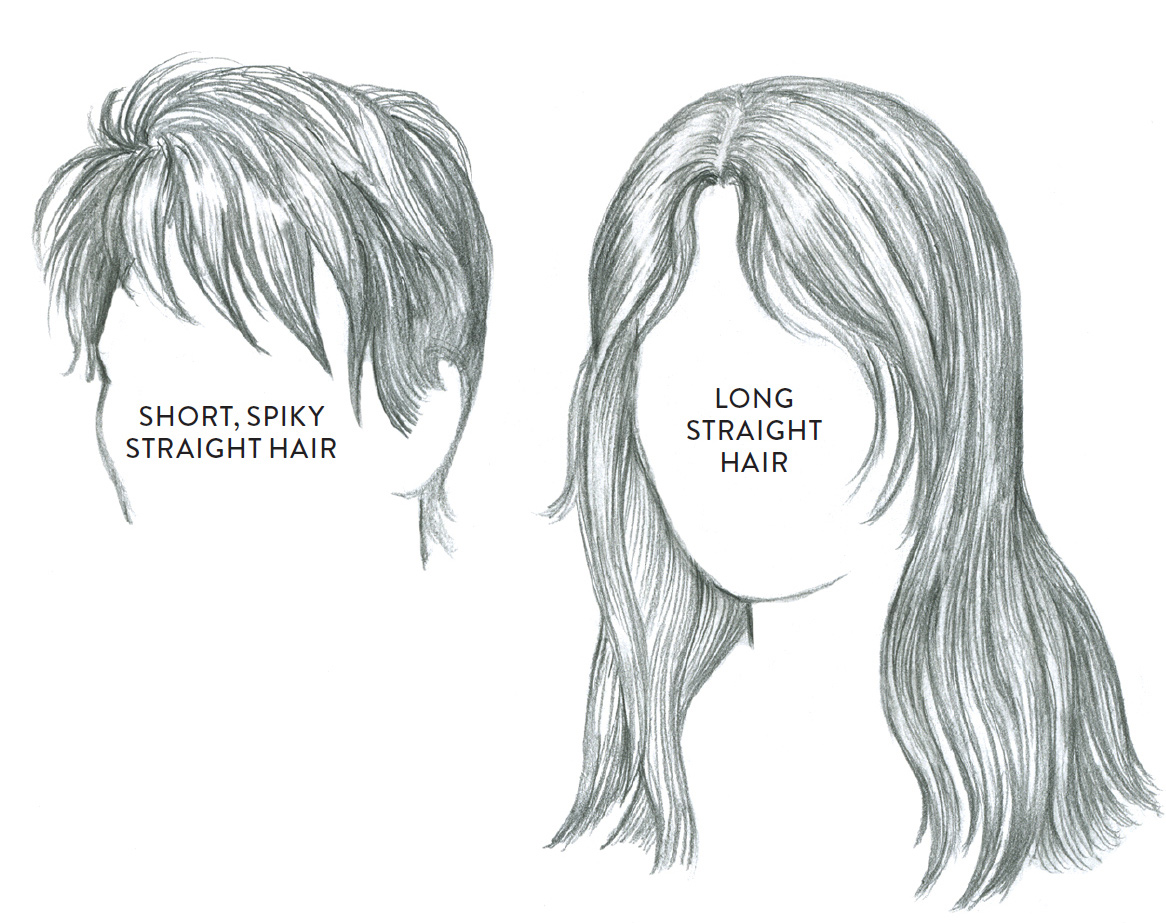
Straight hair
Landmarks of the Torso
Let’s begin our survey of the surface landmarks of the torso with the three drawings that follow, which show the landmarks of the anterior and posterior portions of the male and female torso as well as those landmarks visible from a lateral (side) view. These are followed by discussions of the anterior and posterior landmarks, respectively.
SURFACE FORM LANDMARKS OF THE TORSO—MALE AND FEMALE
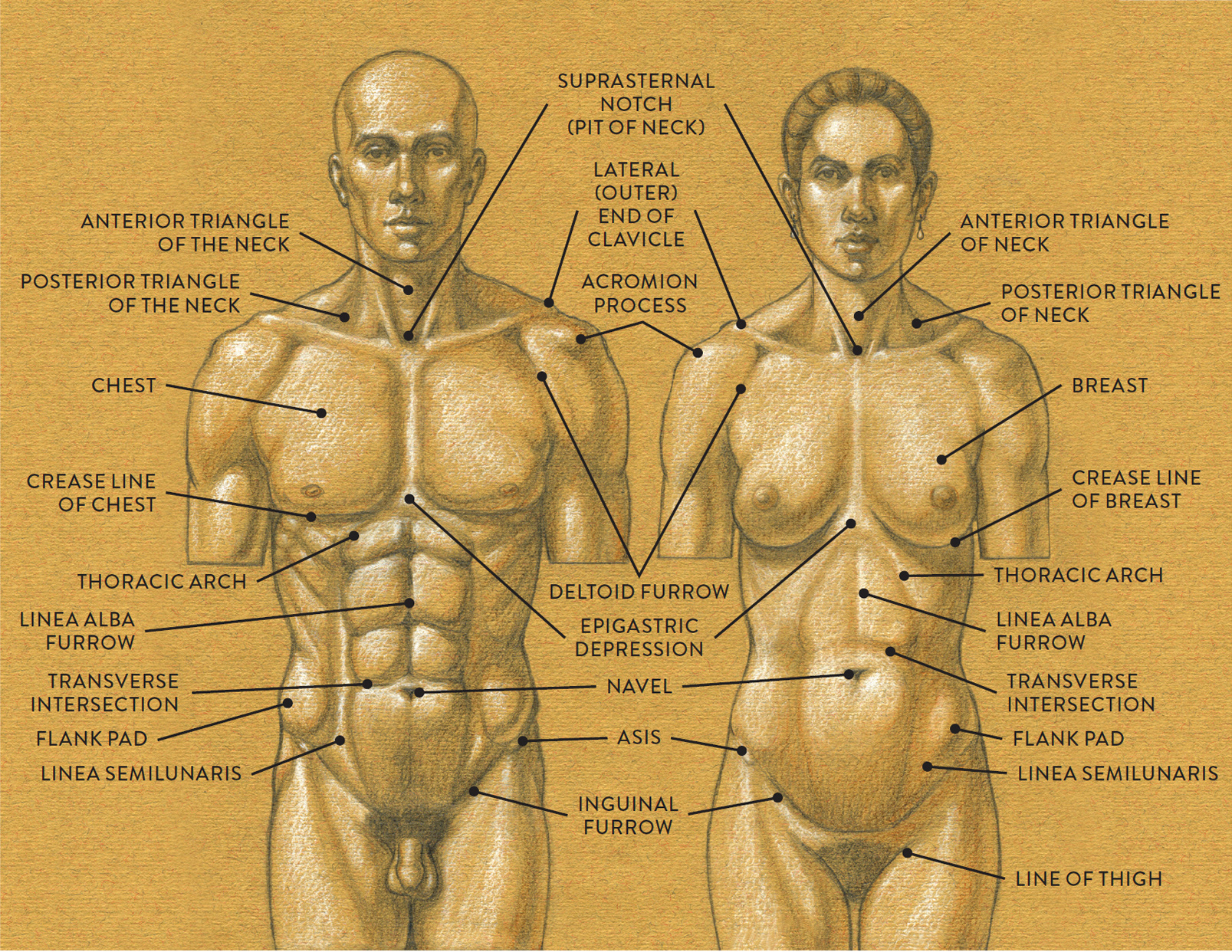
LEFT: Male torso, anterior view
RIGHT: Female torso, anterior view
SURFACE FORM LANDMARKS OF THE TORSO—MALE AND FEMALE
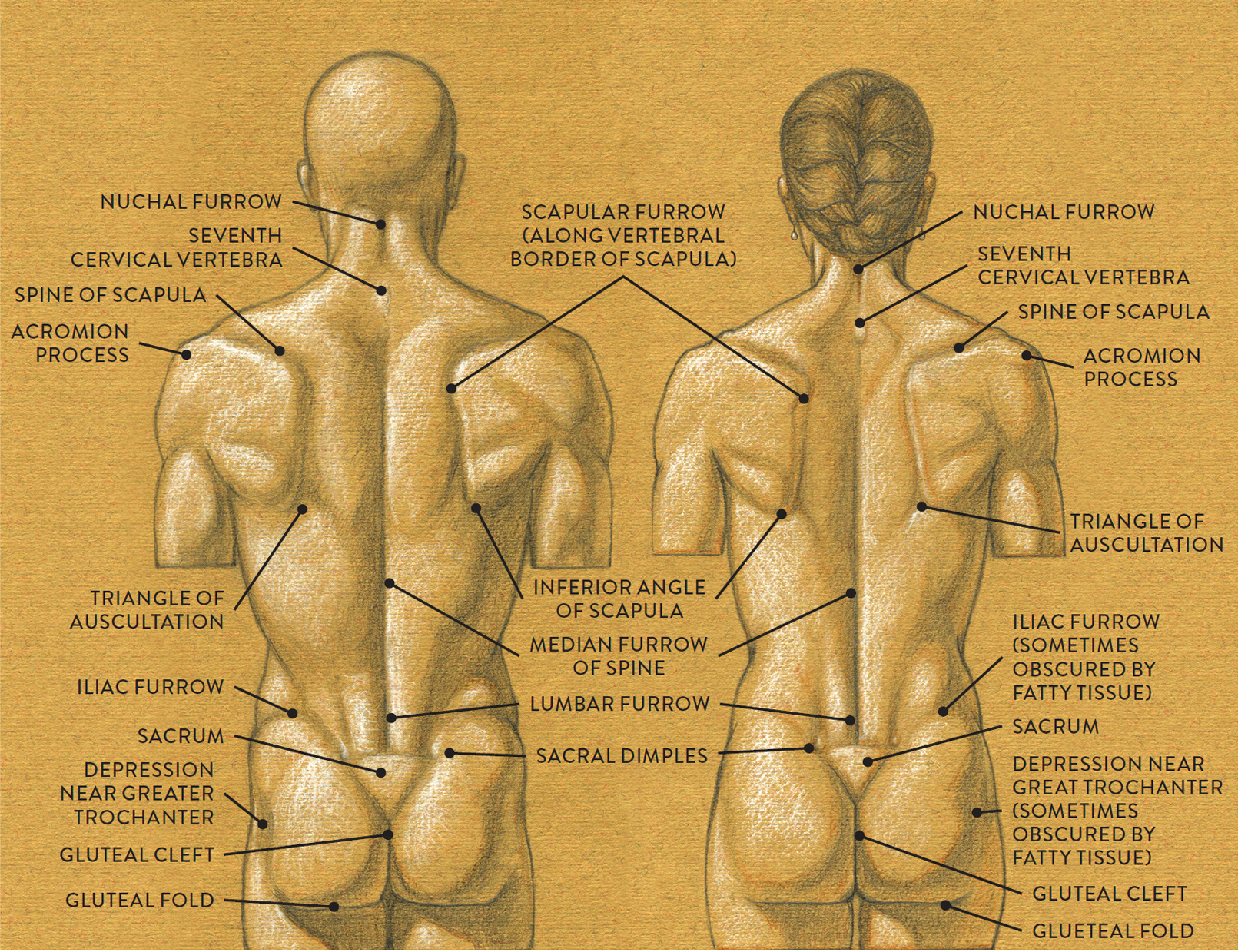
LEFT: Male torso, posterior view
RIGHT: Female torso, posterior view
SURFACE FORM LANDMARKS OF THE TORSO—MALE AND FEMALE
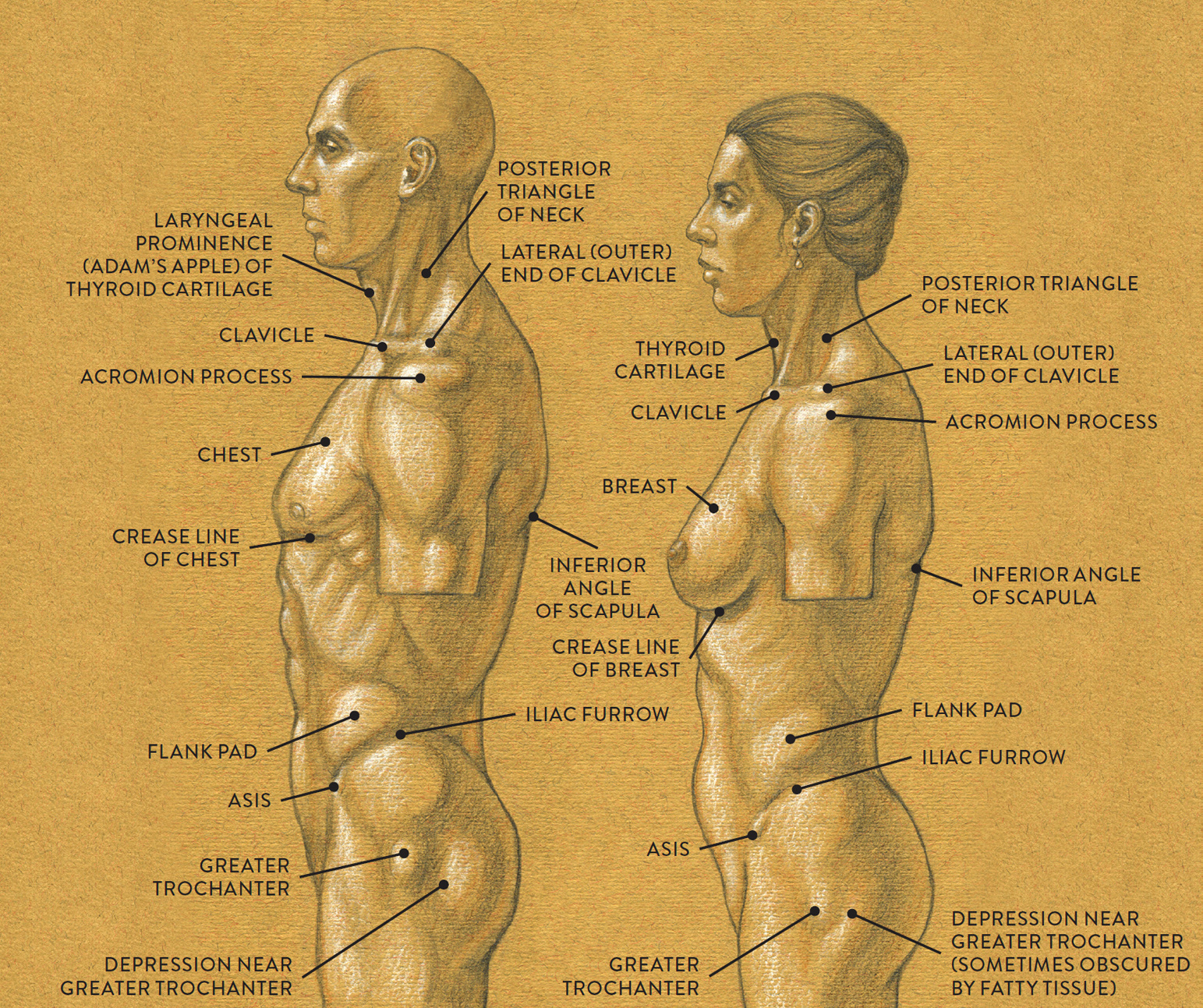
LEFT: Male torso, lateral view
RIGHT: Female torso, lateral view
Landmarks of the Anterior Region of the Torso
The crease line of the chest (or crease line of the breast) is the natural base of the chest/breast region. The skin located at the base of the chest/breast is anchored or fused to the deep fascia to help contain the soft-tissue forms of the chest. On smaller chests/breasts, this lower border is more like a subtle crease or furrow; on fuller breasts the lower border is a deeper fold.
On the front of the torso near the base of the sternum (xiphoid process) is a small triangular depression called the epigastric depression. From the xiphoid process a fibrous band of connective tissue called the linea alba continues in a vertical alignment down the abdomen to attach into the pubic bone. It creates a vertical furrow (linea alba furrow) on the surface from the base of the sternum to the navel and sometimes below the navel.
Located between the outer edge of the rectus abdominis muscle and the inner edge of the external oblique muscle is a furrow called the linea semilunaris. It widens near the ASIS of the pelvis and the inguinal ligament. The horizontal furrows of the abdomen, known as transverse intersections, are fibrous bands that interrupt the muscle fibers of the rectus abdominis muscle. When the figure dramatically bends forward from the waist, rolls occur along these transverse intersections.
The navel is located in the linea alba. The placement of the navel is usually at the lowest intersection of the transverse lines of the rectus abdominis, slightly below the waist. The subcutaneous fat in this area tends to make the navel appear like a deep depression in the skin. However, some navels are small elevations, similar in shape to a small button, hence the colloquial term “belly button.” Depending on the action of the torso (stretching, compression, bending sideways, or twisting), the navel will slightly change shape. It may stretch vertically or horizontally or appear round and craterlike, but it will always remain on the linea alba.
The inguinal ligament attaches from each ASIS (the bony bump at each anterior protrusion of the iliac crest of the pelvis) into the pubic bone. It creates a subtle crease, called the inguinal furrow, on the surface of the skin. It can appear as a soft curve sweeping from one ASIS toward the other ASIS, with the lower part of the curve anchoring on the pubic bone, or it can be more angular, especially on leaner or more muscularly defined torsos. The inguinal furrow is actually a flexor crease linking the skin to the deep fascia and helping keep the soft-tissue forms in place.
Depicting the Genitalia
From an artistic perspective, the genitals are merely forms of the nude body. Artists who draw, paint, and sculpt the nude need to be aware of the basic shapes of the genitalia and know how to place them correctly on the body.
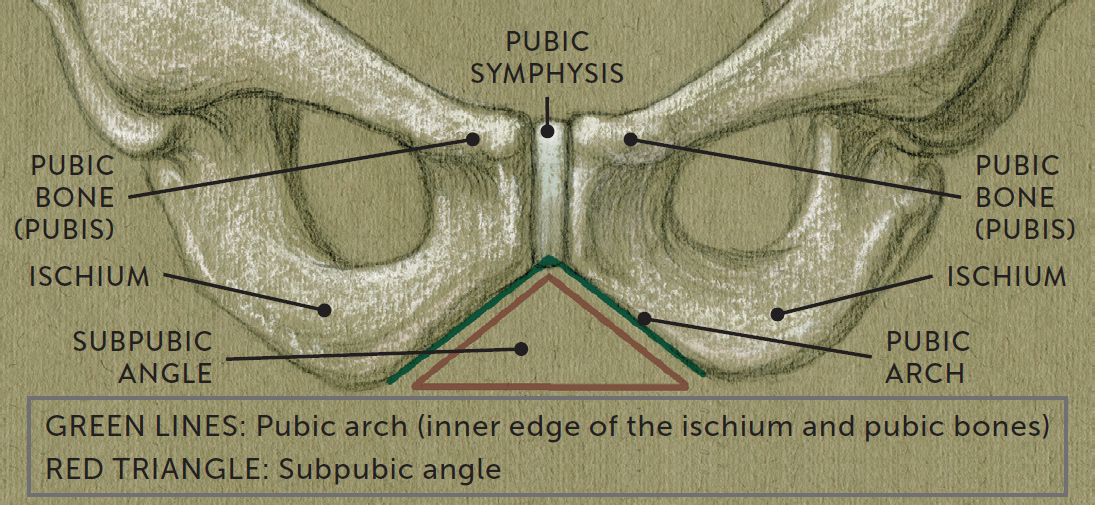
The outer portions of the genitalia of both sexes are located in the subpubic angle (the space within the pubic arch of the pelvis bone), shown in the drawing at right. If the genitalia are placed too high on the figure, they might appear to be positioned on bone, which, anatomically, they are not.
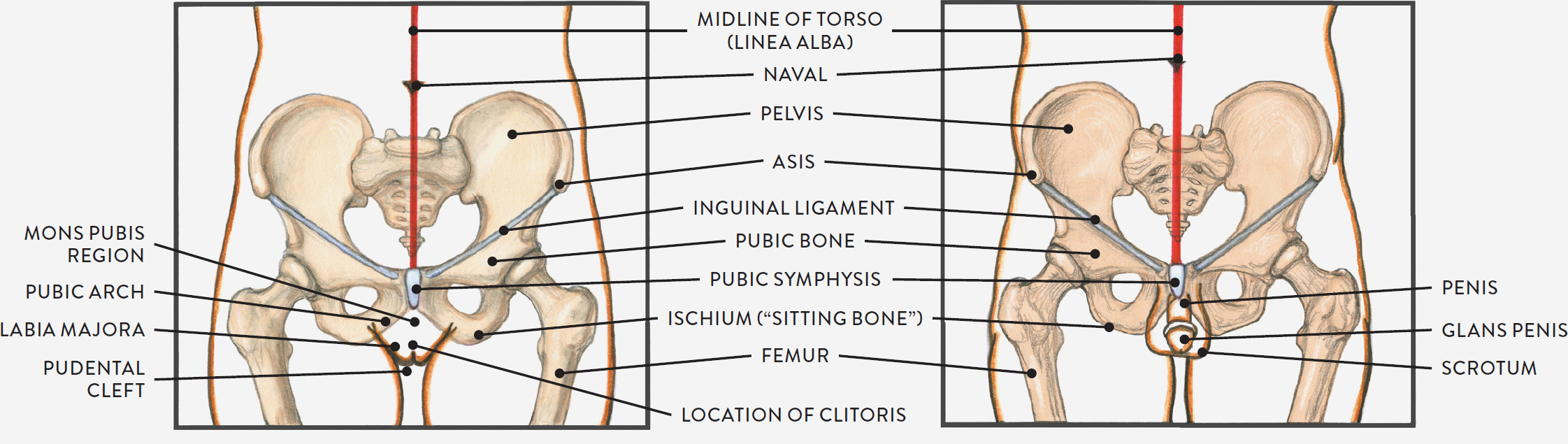
The placement of the genitals is shown in the life studies and accompanying diagrams opposite. On women, a large fat pad (pubic fat pad) positioned below the inguinal ligament and over the pubic symphysis produces a soft triangular fleshy mound called the mons pubis, also known as the mount of Venus. A cleft, called the pudental cleft, occurs on the skin starting near the base of the mons pubis. Beneath the upper part of the pudental cleft is the clitoris, a small erectile organ. On either side of the pudental cleft are two skin folds containing adipose tissue. These folds are called the labia majora and are usually covered with hair.
THE PUBIC ARCH AND SUBPUBIC ANGLE
On men, there are two simple shapes to locate—the tubular shape of the penis and the pouch-like shape of the scrotum, containing the two testes (testicles). The length and width of the penis vary among individuals. In uncircumcised men, loose skin covers the entire length of the penis, overlapping the tip, called the glans penis. When the penis has been circumcised, the glans penis is exposed. The glans is very smooth and similar in shape to an acorn or the cap of a mushroom. The location where the penis emerges, below the inguinal ligament and pubic symphysis, should align with the midline of the torso. From there, the penis might lean in any direction (left or right, upward or downward) according to the placement of the upper legs and the scrotum in a given pose.
SOFT-TISSUE FORMS OF THE GENITALIA IN RELATION TO THE PELVIS
LIFE STUDIES OF GENITALIA, WITH PLACEMENT DIAGRAMS
Torso Study of a Male Figure
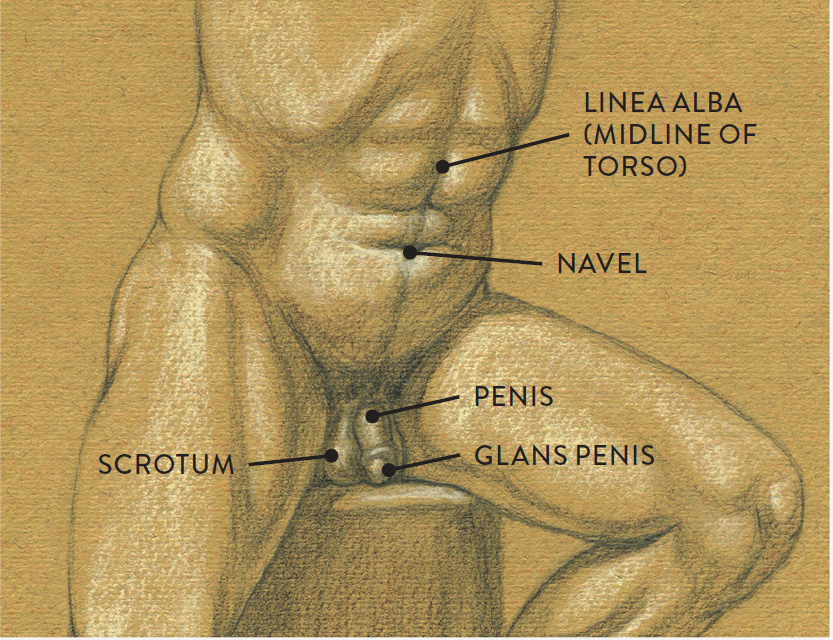
Graphite pencil, colored pencil, and white chalk on toned paper
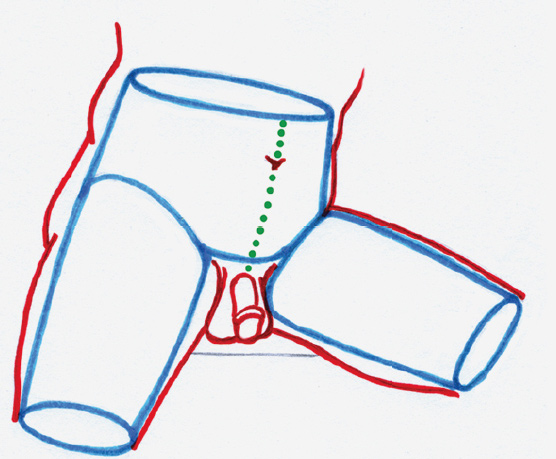
Placement diagram
BLUE LINES: Structure
RED LINES: Soft-tissue forms
DOTTED GREEN LINE: Midline of torso
Torso Study of a Female Figure
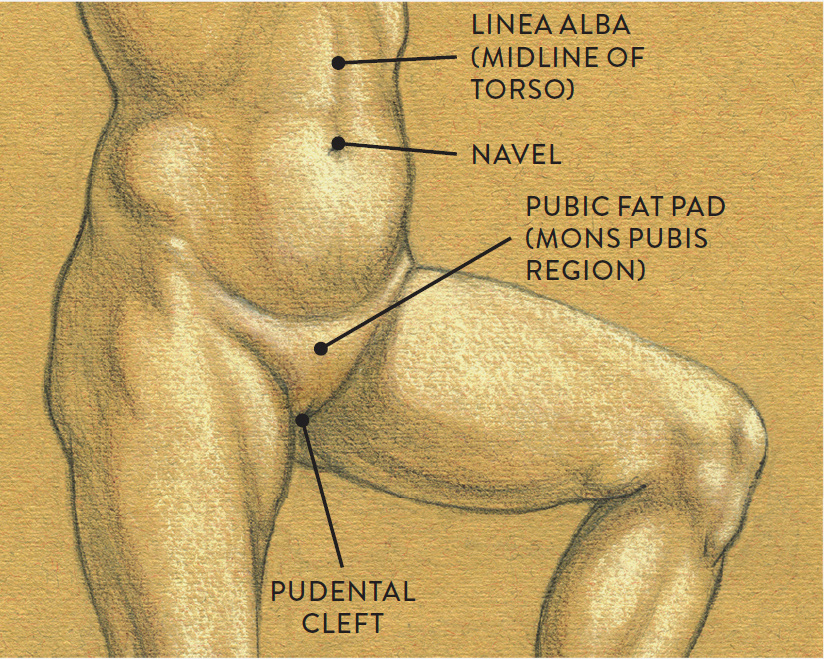
Graphite pencil, colored pencil, and white chalk on toned paper
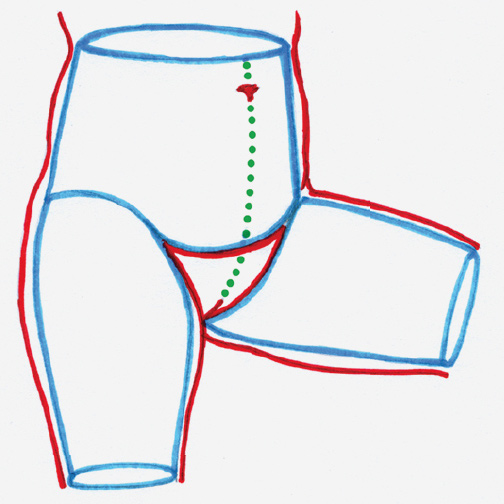
Placement diagram
BLUE LINES: Structure
RED LINES: Soft-tissue forms
DOTTED GREEN LINE: Midline of torso
The shape of the scrotum can vary, looking like a peach in cooler temperatures or when the thighs are positioned close together in sitting poses. In standing poses, when the scrotum is influenced by gravity (or when the temperature is warmer), it becomes slightly elongated and has the shape of a pear or avocado.
Landmarks of the Posterior Region of the Torso
The nuchal furrow is a subtle vertical furrow that is sometimes seen on the back of the neck. This is the location of the nuchal ligament, which is a flat, triangular ligament that attaches at the back of the skull and along the spinous processes of the cervical vertebrae of the neck. Fibers of the trapezius muscle flank both sides of the nuchal ligament, causing the furrow, which tends to be more apparent on leaner or more muscular figures.
An elongated furrow called the scapular furrow can at times be detected on the surface at the inner (vertebral/medial) border of the scapula. This furrow helps identify where the scapula is positioned on the rib cage.
A very small triangular depression called the triangle of auscultation can occur at the vertebral border of the scapula near the bottom tip (inferior angle of the scapula); it is also surrounded by the outer border of the trapezius muscle and the upper border of the latissimus dorsi muscle. Its base, or “floor,” is a portion of the rhomboid major muscle. Auscultation means “listening,” and the depression came by its name because it is where a doctor places a stethoscope to listen to a patient’s lungs. This small surface landmark can help artists identify the position of the lower end of the scapula. Although in some poses a small depression occurs in this region, in other poses a small triangular budge will appear, which is actually a portion of the rhomboid muscle contracting.
Along the vertebral column a deep, trenchlike furrow may occur, especially in dynamic poses when the vertebral column is bending back (extension) or the arms and shoulders are pushing back. These actions cause the sacrospinalis and trapezius muscles to contract into thick cylindrical forms. In the thorax region, this furrow is called the median furrow of the spine, but it is referred to as the lumbar furrow when it appears in the lumbar region. The sacrospinalis muscle is smaller in the lumbar region and produces two small cylindrical forms immediately above the sacrum bone when there is tension in the back. Small furrows on the outer edges of these columnlike forms can occasionally be detected on the surface.
On posterior and side views of the torso, a furrow called the iliac furrow is sometimes seen in the skin between the muscular forms of the external oblique (flank pad) and the iliac crest. The flank pad is sometimes enhanced with a layer of fatty tissue, which can give it a rather prominent round shape on the surface form.
The sacrum bone is padded with a thin layer of connective tissue, producing a soft, sometimes slightly bulging triangular shape, called the sacral triangle, on the surface. The top border of the sacral triangle runs from one PSIS (posterior superior iliac spine) to the other. The sacral dimples are two small indentations, located near the PSIS landmarks, that are produced by the underlying fascia’s attachments to the ends of the iliac crest. Even though these dimples are quite small, they are important surface landmarks because they indicate the top border of the sacrum.
The gluteus maximus muscles attach along the outer edge of the sacrum, one on either side. As they move away from the lower point of the sacrum in opposite directions, they create a deep vertical crevice called the gluteal cleft. The gluteal fold is a horizontal skin crease bordering the lower region of the gluteus maximus. It is created by a straplike fibrous tissue band called the buttock suspensory ligament, which contains fatty tissue. When the leg is standing vertically, the gluteal fold is indicated as a strong horizontal crease sweeping away from the gluteal cleft; when the leg bends, this crease relaxes and temporarily disappears on the surface form, as shown in the following life study.
LIFE STUDY SHOWING GLUTEAL CLEFT AND GLUTEAL FOLD
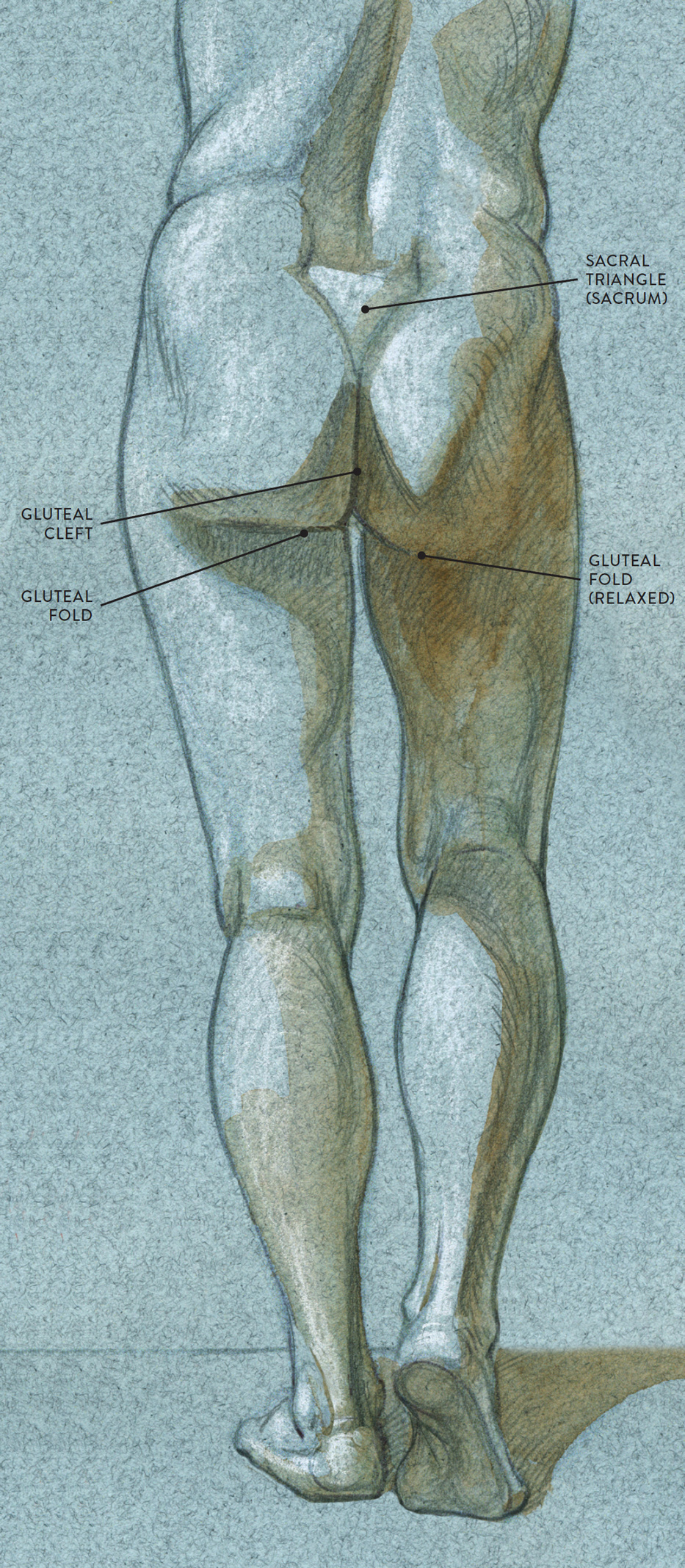
Ballpoint pen, watercolor wash, and white chalk on toned paper.
Landmarks of the Arm and Hand
The next drawing gives a visual overview of the surface landmarks of the upper limb—the upper and lower arm and the hand. Each portion of the upper limb is discussed separately in the sections that follow.
SURFACE FORM LANDMARKS OF THE UPPER AND LOWER ARM AND HAND
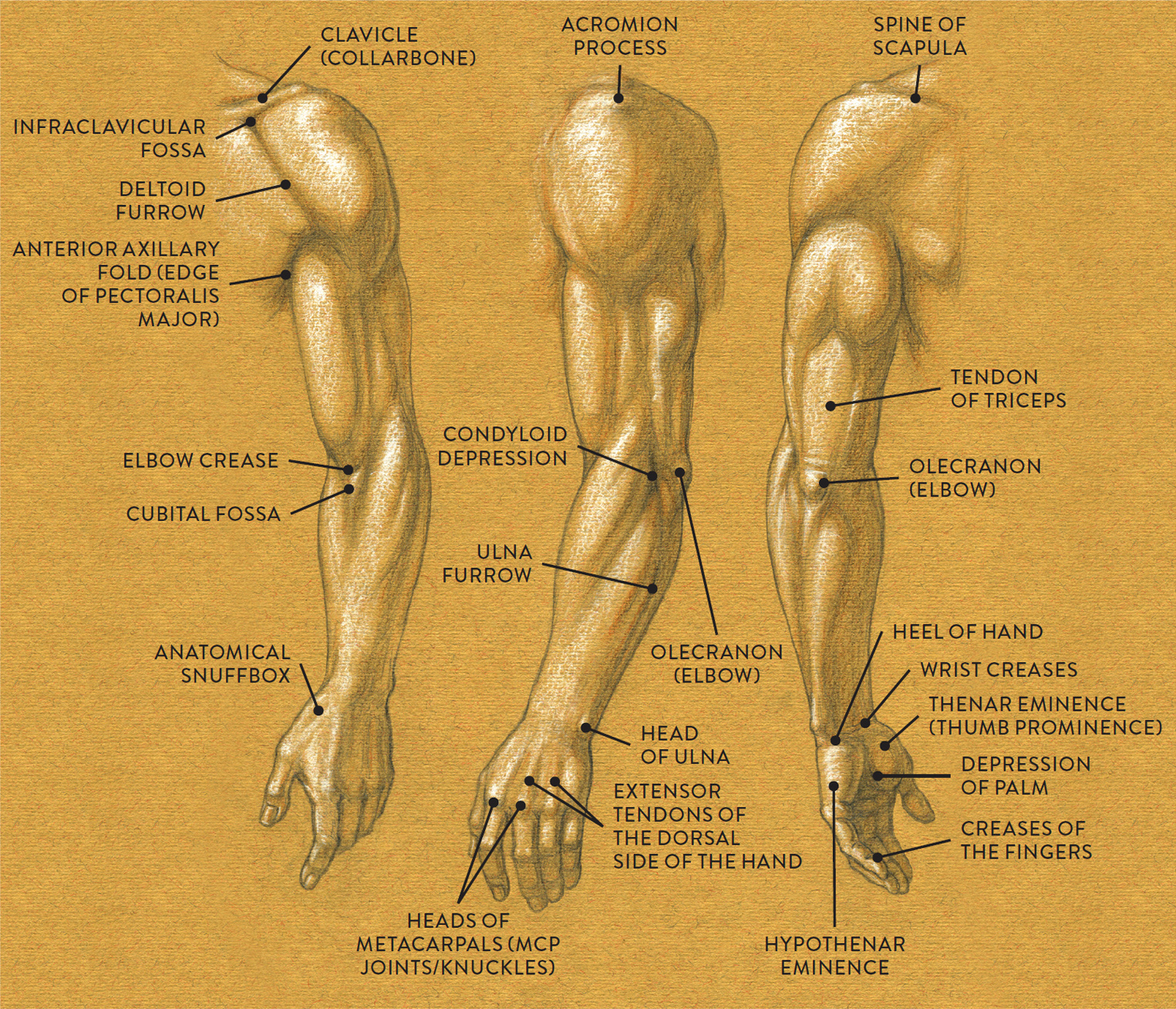
Left arm
LEFT: Anterior view
CENTER: Lateral view
RIGHT: Posterior view
Landmarks of the Upper Arm
The main muscles of the upper arm are easy to detect on a muscularly defined arm: the biceps brachii in front views, the triceps brachii in back views, and the deltoid, which is visible in most views (front, side, and back). Skin furrows may run along the outer borders of these muscles. Between the deltoid and the pectoralis major is a skin furrow called the deltoid furrow; this also marks the transition of planes between these two muscles.
The anterior axillary fold is the outer border of the pectoralis major muscle of the chest as it inserts into the upper arm (humerus). It is seen quite clearly when the arm is pulled away (abducted) horizontally from the torso. The thick outer portion of the pectoralis creates the front (anterior) wall of the armpit (axilla).
Landmarks of the Elbow Region
Several small surface landmarks are located in the elbow region. On the anterior (front) side is the elbow crease, which is considered a flexor crease because it is located at the joint of the elbow where a tremendous amount of bending (flexion) movement occurs. Immediately below this crease is a triangular depression within the skin called the cubital fossa. Its shape is created by the borders of the pronator teres and the brachioradialis muscles. As the skin pulls over this region, it dips slightly, causing the triangular depression, which can only be detected on a straight arm. As the lower arm bends against the upper arm, the elbow crease deepens to an obvious fold and the cubital fossa is no longer visible.
Near the lateral (outer) epicondyle of the humerus is a small depression or dimple called the condyloid depression, which can be seen when the lower arm is straight or extended. This indentation is between the extensor carpi radialis longus muscle (part of the radial muscle group) and the anconeus muscle near the elbow (olecranon). On a muscularly defined arm, this depression appears as an inverted V-shaped furrow. When the lower arm bends, the dimple disappears and the bony protrusion of the lateral epicondyle of the humerus appears on the surface.
On the posterior portion of the elbow region is the obvious bony landmark of the elbow (olecranon), a small round bony protrusion occurring on the upper part of the ulna bone. It is most noticeable when the lower arm bends. On the straight arm, the elbow is harder to detect on the surface, but minor skin creases above it indicate its whereabouts. On a muscular arm, the triceps tendon might be seen on the surface as it anchors into the olecranon.
Landmarks of the Lower Arm
An elongated skin furrow called the ulnar furrow can usually be detected in the lower arm. It follows along the ulna bone on the posterior border of the ulna, from the elbow (olecranon) to the outer wrist (head of ulna). This furrow occurs between the flexor carpi ulnaris muscle and the extensor carpi ulnaris muscle of the lower arm.
Wrist creases are subtle horizontal creases across the wrist that are usually more noticeable when the hand bends forward (flexion). Creases may occur on the dorsal side of the hand at the wrist when the hand is extending back. When depicting wrist creases on a hand that is not bending, draw them extremely lightly so that they do not appear as heavy lines cutting across the base of the palm.
Landmarks of the Hand
There are many obvious surface forms on the hand, especially in the palm region, as shown in the following drawing.
SURFACE FORM LANDMARKS OF THE HAND
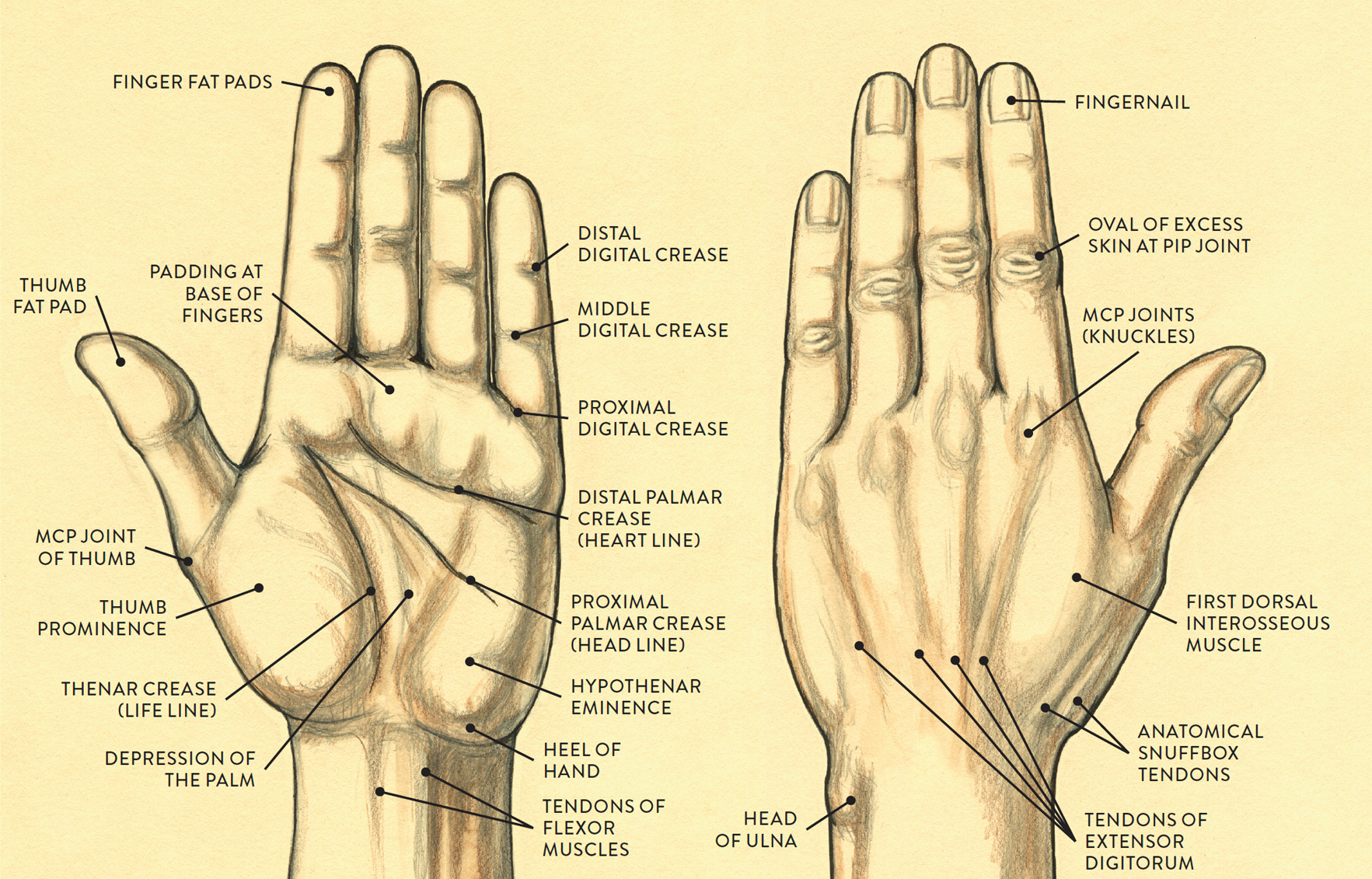
Left hand
LEFT: Palmar surface
RIGHT: Dorsal surface
The bottom portion of the hypothenar eminence contains the heel of the hand, which is the location of the pisaform carpal bone covered over with fibrous fatty tissue. At the base of the fingers on the palm side is an elongated fibrous padding. It tends to divide into rich fleshy mounds when the fingers move as a group or individually. In the central portion of the palm, between the thumb prominence, hypothenar eminence, and the padding at the base of the fingers is a large triangular depression. Known as the depression of the palm, it is the location of the palmar aponeurosis. The depression is more noticeable when the hand is cupped.
Permanent skin creases on the palm side of the hand are known collectively as flexor creases of the palm. While there are several creases in the region of the palm, three especially stand out: the thenar crease, the proximal palmar crease, and the distal palmar crease. The common names for these creases—life line, head line, and heart line, respectively—derive from the ancient art of palmistry. The thenar crease curves around the thumb prominence. The proximal palmar crease begins near the upper part of the thenar crease and descends diagonally across the palm. The distal palmar crease travels somewhat horizontally across the palm along the padding at the base of the fingers heading upward toward the second and third fingers.
Skin creases that occur at the joints of the fingers on the palmar side of the hand are known collectively as creases of the fingers (palm side). The distal digital crease is at the first joint of the finger; the middle digital crease at the middle joint; and the proximal digital crease at the base of the finger. As the fingers bend these creases deepen into prominent folds and are important to indicate, especially in foreshortened views of the fingers (advancing and receding positions). Even when the foreshortened fingers are straight, the crease lines help to describe how the finger joints are divided into different sections.
FINGER CREASES ON THE CYLINDRICAL SURFACE FORM
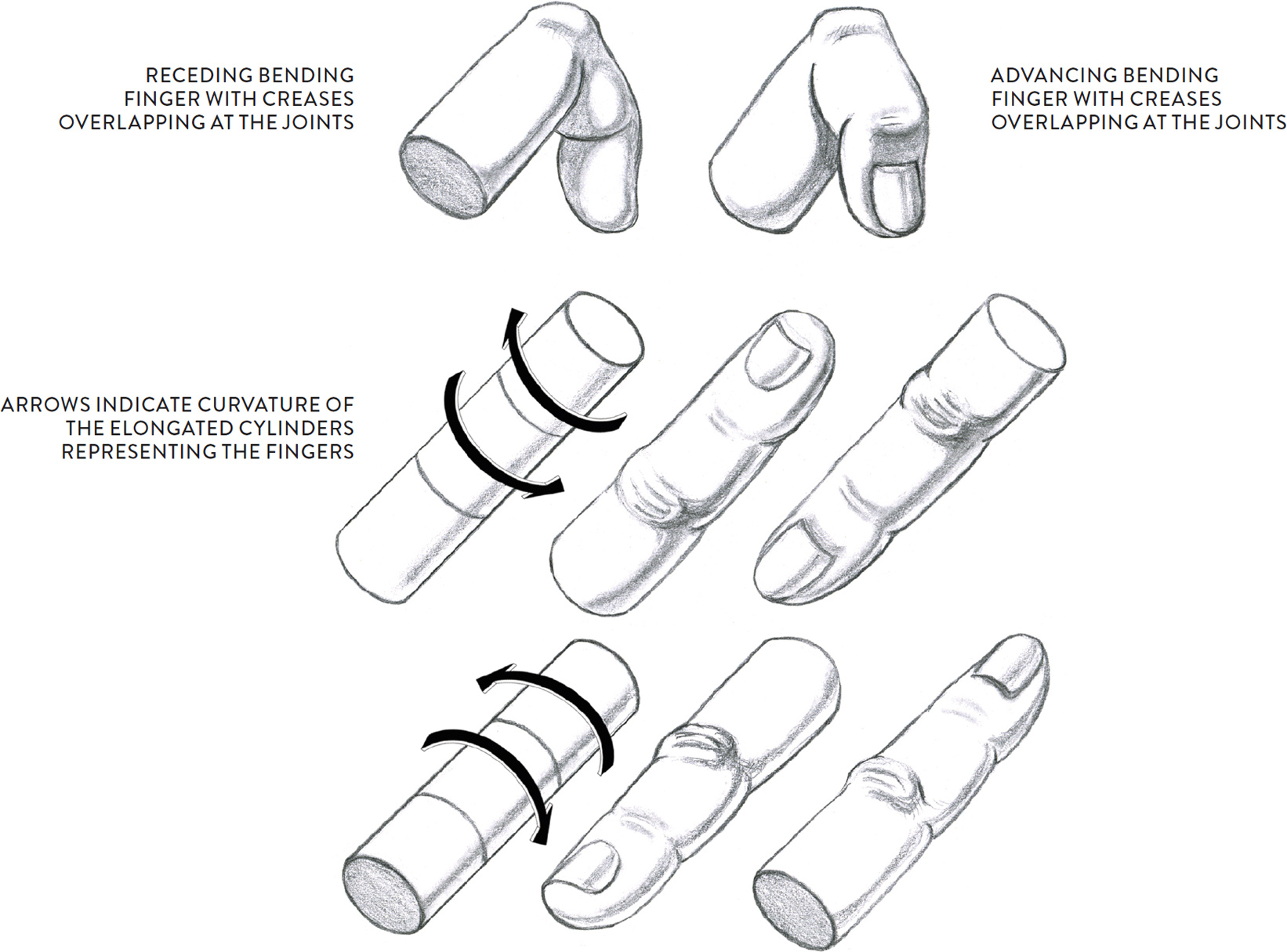
Creases follow the curvature of the finger, whether it is advancing or receding.
On the dorsal side of the hand the skin pulls tightly against the surface. Bony landmarks include the knuckles of the hand (MCP joints) and the PIP and DIP joints of the fingers, but are only seen when the fingers are bending. The subcutaneous layer contains minimal fat on the dorsal side of the hand, and the only muscle seen on the surface is the first dorsal interosseous muscle, which appears as a triangular mass between the outstretched thumb and the hand block or as a small egg-shaped form when the thumb is held close to the hand. When the thumb is pulled upward, as in a “thumbs-up” gesture, an elongated triangular depression occurs in the skin near the inner wrist. Called the anatomical snuffbox, it is formed by the tendons of the extrinsic muscles of the thumb. (See this page for more discussion of this landmark.)
Other surface landmarks of the dorsal side of the hand include the tendons of the extensor digitorum muscle, which are more noticeable when the fingers are under tension (as when the fingers are spread apart). Veins are also noticeable, especially on the hands of older people, but most artists edit these out in briefer studies of the hands. In longer studies, tendons and veins can be indicated, though not too strongly if the hand is youthful. When depicting the hands of an elderly person in a long study, the tendons, veins, and skin creases may be emphasized to help create a sense of character.
Of the skin creases on the dorsal side of the fingers, the most obvious cluster occurs at the PIP joint. The creases appear within an oval skin mass, which is excess skin that stretches out when the finger bends to allow full flexion of the finger.
Fingernails appear shiny and hard because they are made of a material called keratin. Nails can be wedge shaped, fan shaped, square, or oval. At the base of the fingernail is a pale crescent shape called the lunula. The tip of the nail is the free edge, or free margin, which is usually a lighter color than the rest of the nail. The nail folds are located on the inner and outer side of the nail, and the border between the nail and nail fold is called the nail groove. At the base of the fingernail is the cuticle. The life study here shows all these characteristics.
STUDY OF HANDS WITH INTERTWINING FINGERS
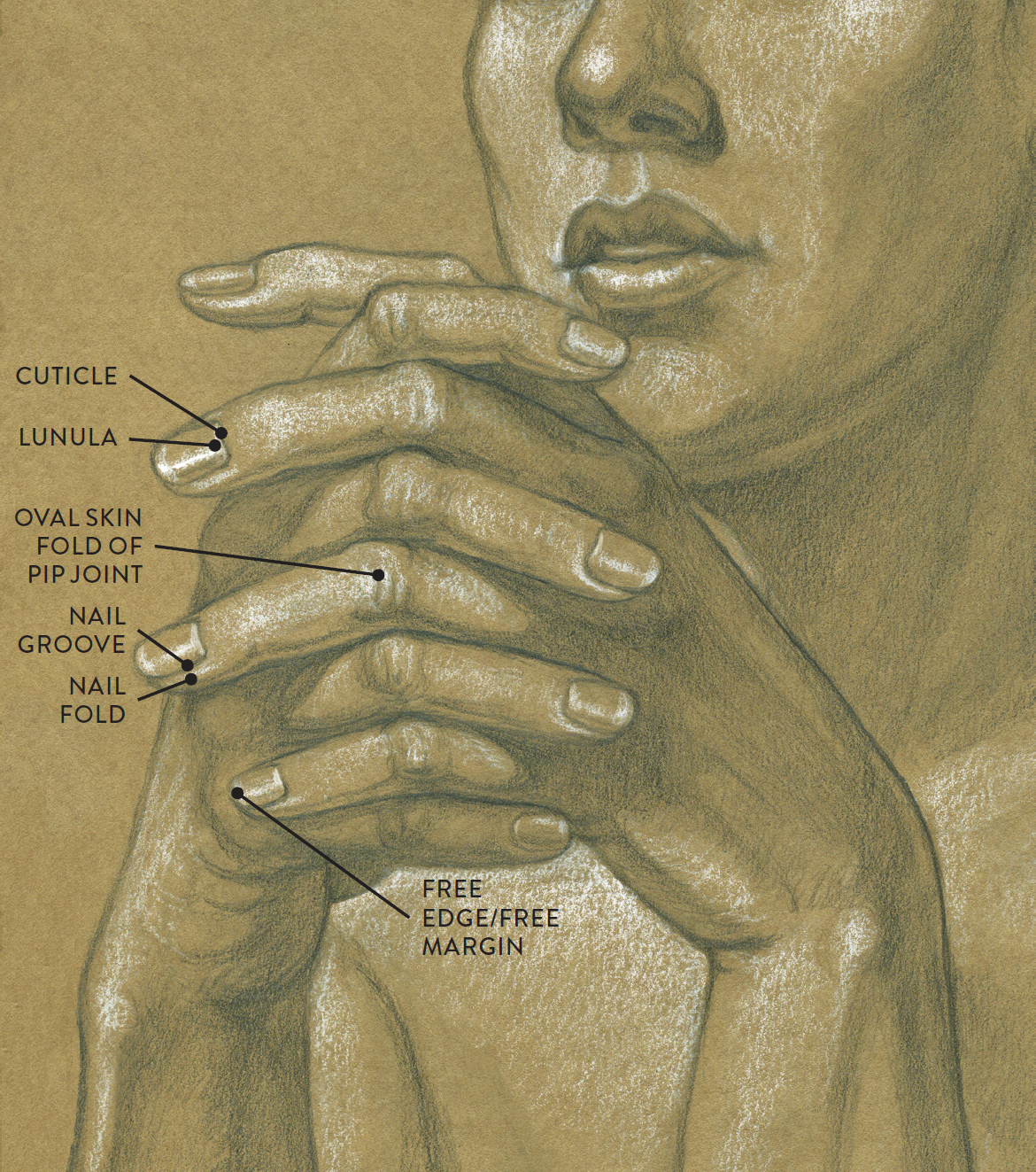
Graphite pencil and white chalk on toned paper.
Landmarks of the Leg and Foot
The following drawing gives a visual overview of the surface landmarks of the lower limb—the upper and lower leg—in lateral, anterior, and posterior views. The landmarks of each of these portions of the lower limb are discussed separately in the sections that follow, as are the landmarks of the foot.
SURFACE FORM LANDMARKS OF THE UPPER AND LOWER LEG
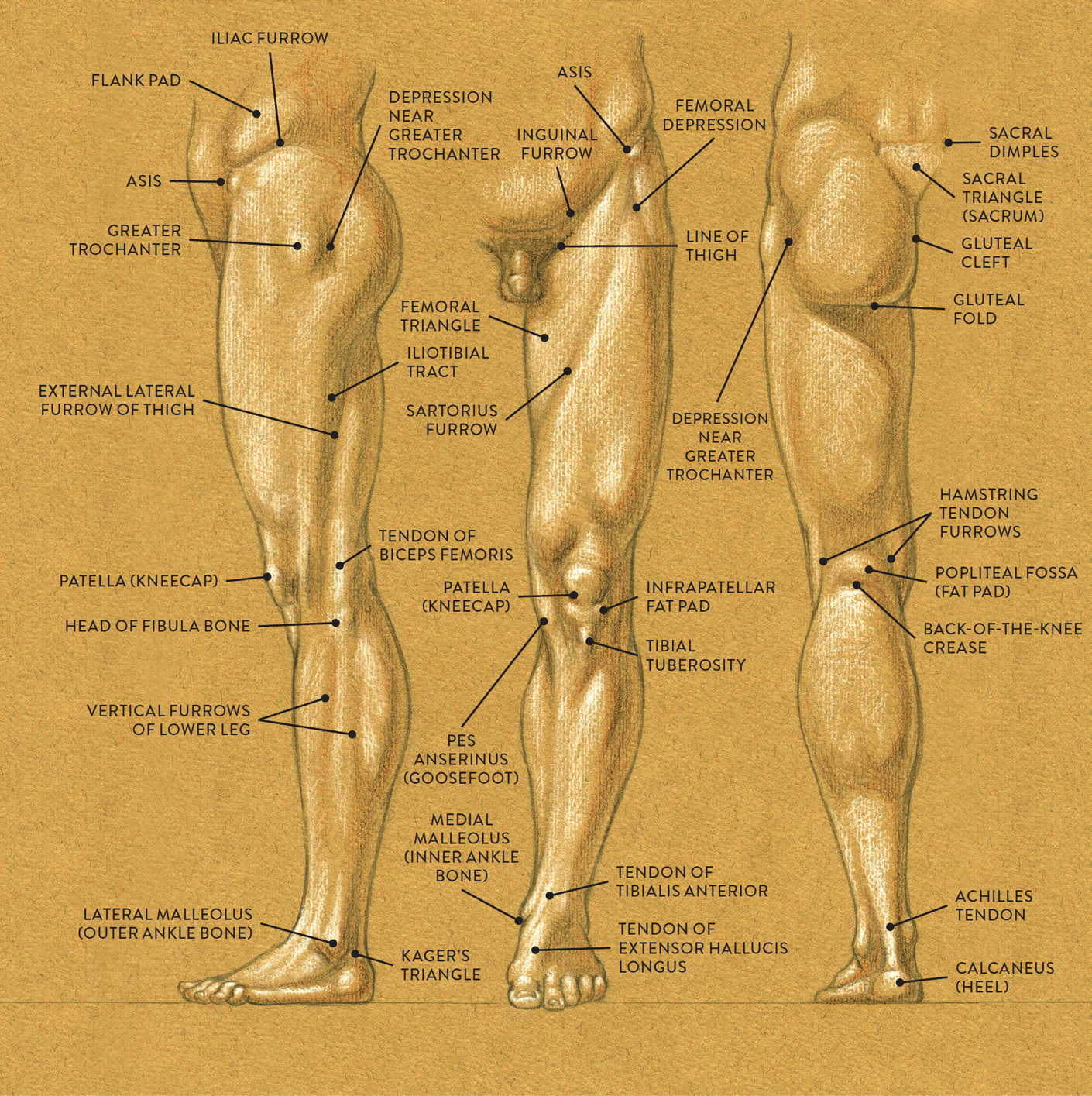
Left leg
LEFT: Lateral view
CENTER: Anterior view
RIGHT: Posterior view
Landmarks of the Upper Leg
Located on the front of the upper leg is a skin fold called the line of the thigh that marks where the upper legs connect into the torso. As the upper leg bends, this crease becomes more apparent.
On very muscular legs, a very small triangular depression called the femoral depression occurs between the inner border of the sartorius muscle near its insertion at the ASIS and the outer border of the tensor fasciae latae muscle.
At the side of the upper leg, near the prominent bump of the greater trochanter of the femur, is a large depression or hollow in the skin referred to as the depression near the greater trochanter or the retrotrochanteric groove. Following the outer border of the iliotibial tract downward is an elongated furrow called the external lateral furrow of the thigh. This furrow helps indicate the division of the quadriceps muscle group and hamstring muscles on the outer length of the upper leg.
As the sartorius muscle descends from the ASIS, its inner edge can be seen as a subtle, trenchlike furrow, called the sartorius furrow, moving downward and diagonally on the thigh. The adductor muscle group is located between the inner thigh and inner border of the sartorius muscle. Part of this triangular region is called the femoral triangle, which is bordered by the inguinal ligament, the sartorius muscle, and the medial border of the adductor longus muscle. It is seen when the thigh is flexed, abducted, or laterally rotated.
The pes anserinus (goosefoot) is formed by three tendons of the upper leg—the tendons of the sartorius, gracilis, and semitendinosus—which all wrap around the inner condyles of the femur and tibia to insert on the inner side of the knee region. The pes anserinus has an egglike shape on the surface due to the small sacs of fluid (bursa) and the fatty tissue padding this area.
Landmarks of the Knee Region
Looking at the knee region of a standing leg from the front view, you see two similar rounded forms. The upper form is the patella (kneecap), which is bone; the shape immediately below, composed of soft fatty tissue, is called the infrapatellar fat pad. Another surface landmark in this region is the patellar ligament, which attaches from the patella into the small bump on the tibia called the tibial tuberosity.
At the back of the knee region is a skin crease called the back-of-the-knee crease, with the hamstring tendons positioned on either side. One of these tendons, from the biceps femoris muscle on the outer posterior region of the upper leg, has a thick, cordlike appearance. These forms are easily seen, especially in side and three-quarter views when the knee is flexed.
Landmarks of the Lower Leg
On muscular legs, noticeable ridges occur along the outer lower leg. These vertical furrows of the lower leg appear along the sides of the peroneus muscles, which subdivide the lower leg into three ridges of muscular form. Sometimes an additional ridge, of the soleus muscle, will also appear. These furrows are especially apparent on the lean but muscular legs of joggers, bicyclists, and other athletes who use their legs extensively. If the legs have a soft layering of adipose tissue, the divisions between the lower leg muscles will not be apparent.
At the back of the lower leg, near the heel, is the Achilles tendon (calcaneal tendon). It descends from the calf muscles (gastocnemius and soleus) and tapers into a ropelike structure, inserting directly into the heel bone (calcaneus). Kager’s triangle is the triangular space between the outer ankle and the Achilles tendon.
Landmarks of the Foot
The many bones of the foot are usually obscured—on the dorsal side by extrinsic tendons from the lower leg muscles, and on the plantar side (sole) of the foot by fat pads. The most noticeable tendons on the dorsal surface are the tendon of the tibialis anterior, the tendon of the extensor hallucis longus, and the four tendons of the extensor digitorum longus. The various pads of fat and extremely thick skin on the sole help protect it from friction and serve as shock absorbers.
Positioned on the bottom of the foot below the large toe is the ball-of-the-foot fat pad, which has a thick, round shape. Located on the bottom and sides of the heel, the oval-shaped fat pad of the heel is the thickest fat pad of the foot. This fat pad buffers the heel from the friction and impact it endures in the actions of walking, jogging, and running.
Along the outer edge of the foot, the abductor digiti minimi muscle forms an elongated muscular ridge. Overlapping this muscle is fatty tissue that sweeps around to the sole, creating an elongated teardrop-shaped fat pad referred to as the lateral foot pad.
SURFACE FORM LANDMARKS OF THE FOOT
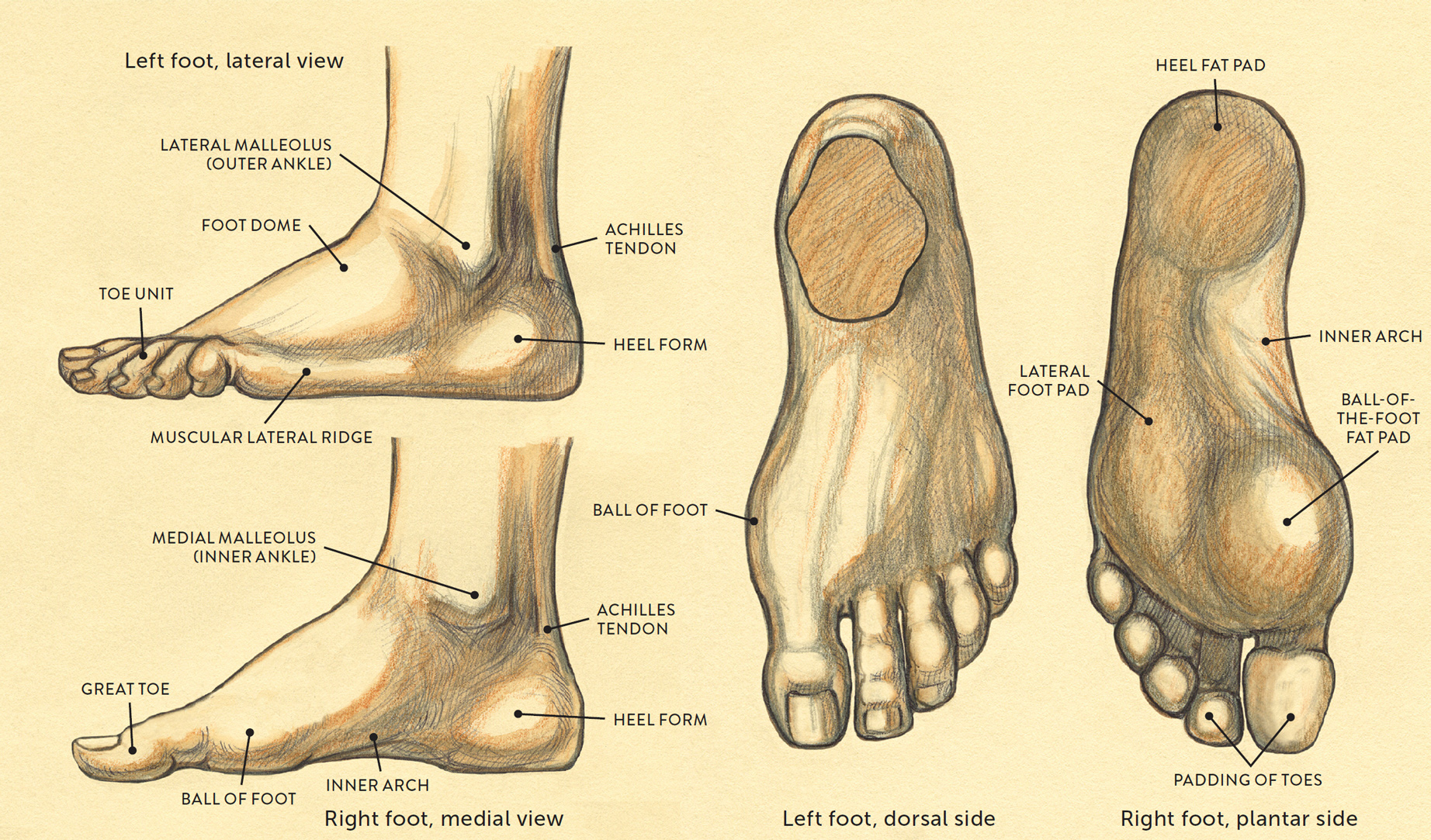
The fat pads of the toes are positioned at the tips and sides of the last bone of each toe. When viewing from underneath, the toes look like fat beads or rounded wedge shapes. The fat pad of the great toe has a chubby heart shape. There are no fat pads on the inner arch of the foot, which usually does not touch the ground; the skin here is thinner than that of the rest of the sole.
The Subcutaneous Layer
Many of the body’s surface landmarks are caused by muscles or portions of bones pushing close to the skin. The surface forms are, however, also influenced by the subcutaneous layer, also known as the superficial fascia, which lies between the skin and the deep fascia covering the muscles. This layer consists mainly of areolar connective tissue and adipose connective tissue (fatty tissue). The subcutaneous layer, which encapsulates virtually the whole body under the skin, varies in thickness from place to place. The fatty tissue layer can be quite thin in some locations, as on the bridge of the nose, or extremely thick, as in the region of the buttocks. It softens the definition of muscles by smoothing their contours, and it fills small spaces or hollows that occur between anatomical structures. Even extremely thin people have some small amount of adipose tissue within the subcutaneous layer. When an abundance of fatty tissue is present in the subcutaneous layer, it is called subcutaneous fat. When fat accumulates, it eventually alters the surface of the body, sometimes significantly.
The subcutaneous layer reacts to the dynamics of movement. Rolls in the flesh and deep creases and furrows in the skin can indicate that the subcutaneous layer is being compressed or stretched. An artist’s awareness of the subcutaneous layer can give sensuality, radiance, liveliness, or luminosity to his or her depictions of the human figure, transforming a stiff or “robotic” figure study into one with a feeling of sensual vitality.
The superficial fascia of the subcutaneous layer attaches over the deep fascia by fibrous strands of collagen. The deep fascia, positioned beneath the superficial fascia, consists of thin, usually shiny membranes appearing as broad sheets; its function is to cover individual muscles or groups of muscles to help bind them together. The superficial fascia is thicker and contains small clusters of globular yellow forms of adipose tissue.
Even though the superficial fascia layer is firmly attached to the deep fascia layer, it has great elasticity and can move very easily when the body moves. For artists, it is very interesting to see how the soft tissues of the surface stretch and compress in different directions within various poses.
Fat Pads and Fatty Tissues
A fat pad consists of a fibrous tissue membrane containing closely packed fat cells. Anatomically necessary, fat pads function as shock absorbers, especially around joints (e.g., the infrapatellar fat pad of the knee), or act as cushions protecting nerves, blood vessels, and muscle layers from impact. Sometimes a fat pad is so well concealed by the skin and surrounding forms that it may be hard to see on the surface. In other areas, the padding softens muscular forms (e.g., the malar fat pad covering some facial muscles), creating a gentle transition from one form to the next. When depicting the figure, an artist should pay attention to any soft-tissue presence that might be essential to emphasize.
The following drawings show the general locations of fat pads and other noticeable fatty-tissue shapes throughout the male and female bodies. Do remember that most of the body is encased by a continuous thin layer of fatty tissue within the subcutaneous layer; in these drawings, that encompassing layer has been removed to show only the more obvious fat pads against the background of the superficial muscle layer.
GENERAL LOCATION OF FAT PADS AND FATTY TISSUE—MALE
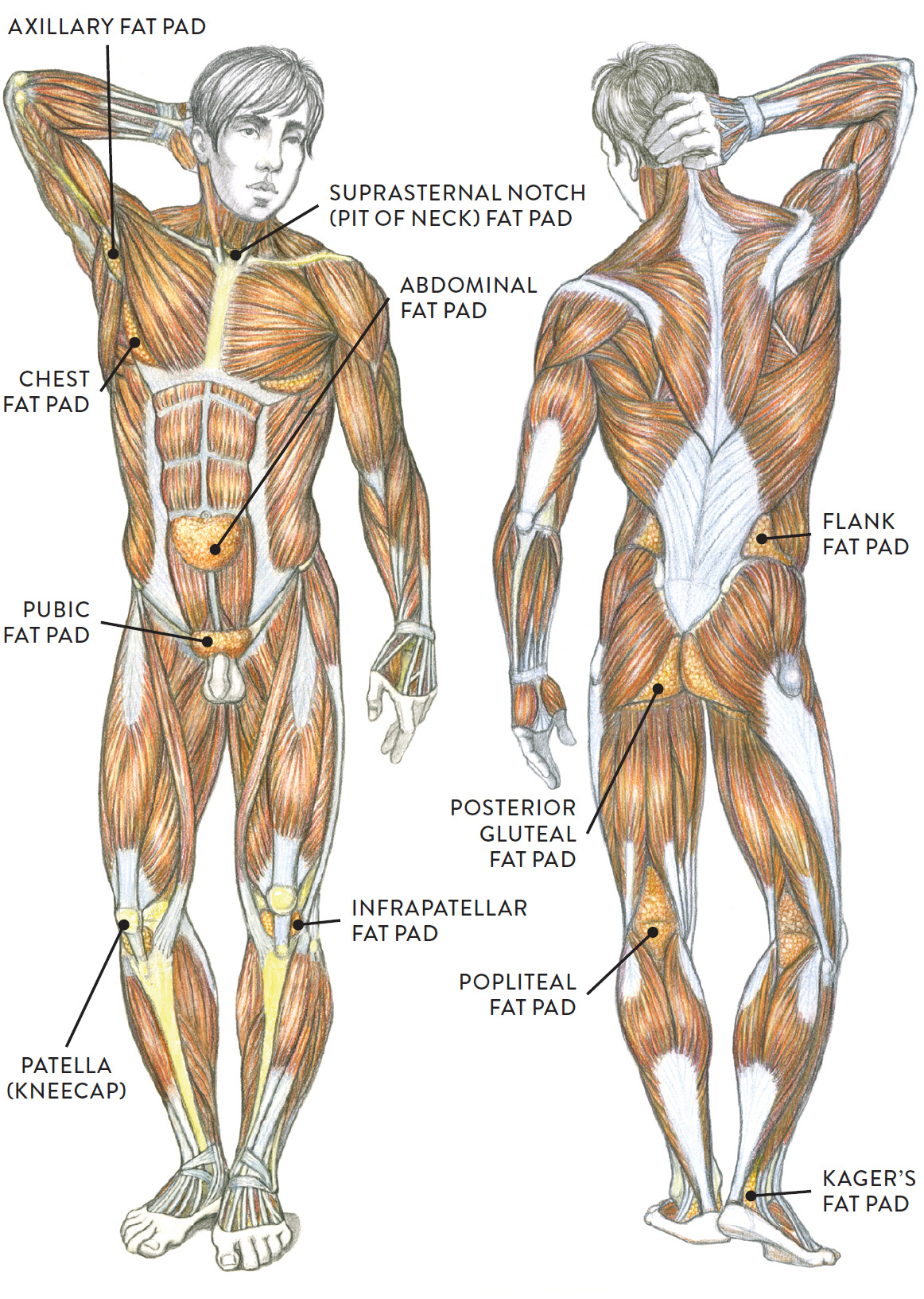
Anterior (left) and posterior (right) views
GENERAL LOCATION OF FAT PADS AND FATTY TISSUE—FEMALE

Anterior (left) and posterior (right) views
GENERAL LOCATION OF FAT PADS AND FATTY TISSUE—FEMALE

Lateral view
Fatty Tissues of the Face and Neck Region
Facial variations have much to do with the shape of the skull, but the placement of soft-tissue forms, including fatty tissues, gives the face its fleshiness and individual uniqueness. There are several compartments of fat on the face, but it is not important for artists to know each one. Being aware of the placement of these fleshy soft tissues can, however, help you avoid making the face look mechanical or robotic.
FAT PADS AND OTHER SOFT-TISSUE FORMS OF THE FACE
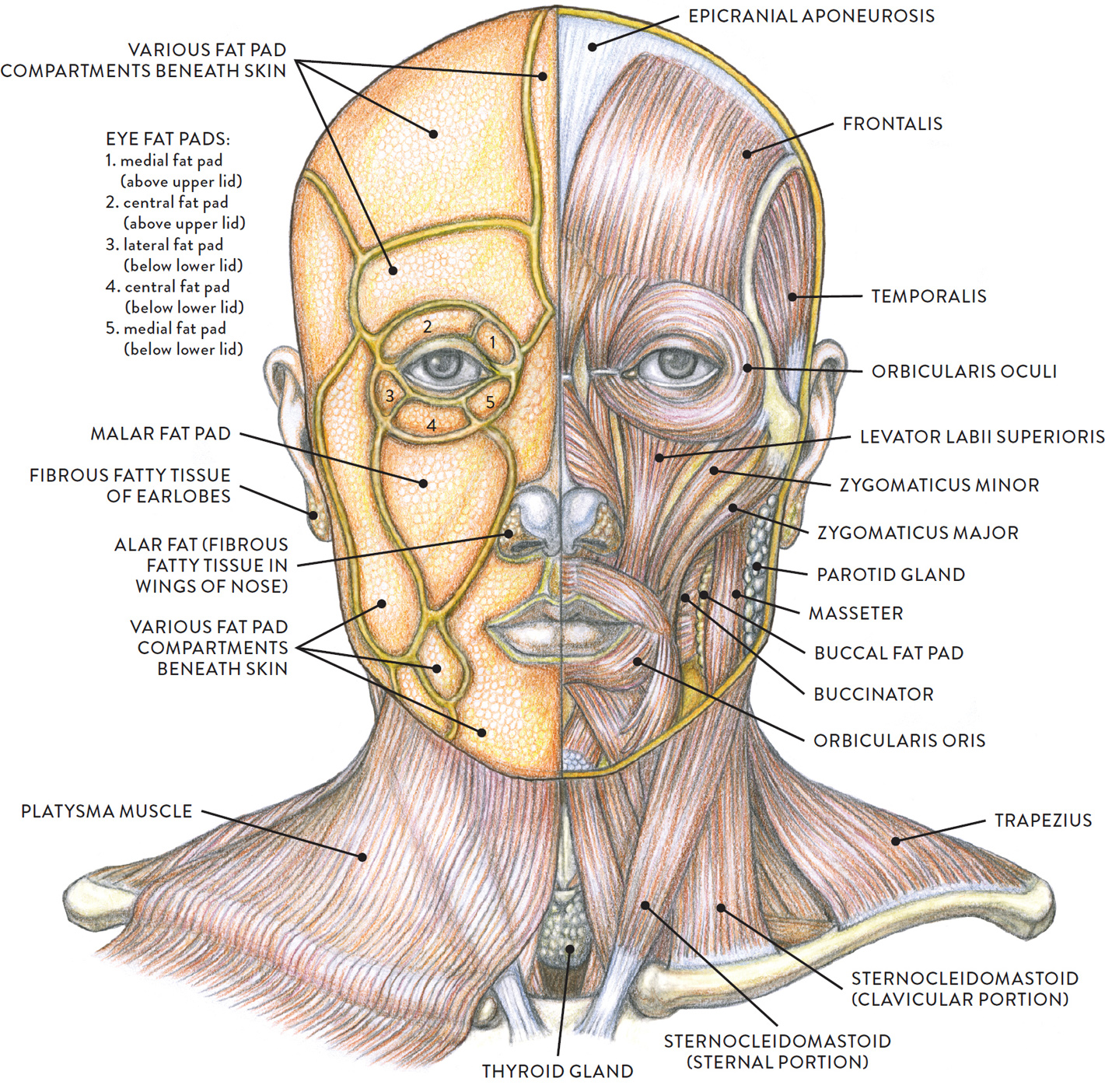
Left side: Fat pads and platysma muscle
Right side: Muscles and other soft-tissue forms
Youthful fleshiness, colloquially referred to as “puppy fat,” often gives way as a person matures. With the normal course of aging, the fatty tissues of the face become less prominent, making the face more angular. In the elderly, the fatty tissue often atrophies and begins to descend as the skin loses elasticity. This may give the upper region of the face a skull-like appearance and the lower portion of the face a sagging quality.
Several small fat pads above and below the lids of the eye flesh out the surrounding eye socket. In the upper eye region, above the upper lid, are two fat pads:
The central fat pad (or pre-aponeurotic fat pad) is an elongated fat pad located above the eye but within the orbit; this fat pad may be more apparent on eyes with the epicanthic fold. There is no fatty tissue on the actual upper lid, so when depicting that form, keep the skin of the lid somewhat thin as it wraps over the ball of the eye. The smaller medial fat pad (or nasal fat pad of the upper lid) is near the inner corner of the upper rim of the orbit.
In the lower eye region, below the lower lid, are three fat pads: The lateral fat pad (or temporal fat pad) is near the outer region of the eye, situated within the orbit near the lower lid. The medial fat pad (or nasal fat pad of the lower lid) is a small fat pad located on the medial (inner) part of the eye near the nose. The central fat pad is an elongated pad of fat located in the central portion of the bottom rim of the eye socket, directly below the lower lid. In the elderly, these pads become more apparent on the surface as they sag over time, creating what are called “eye bags.”
The mid-face region has two main fat pads: the more superficial malar fat pad and the deeper buccal fad pad. The triangular malar fat pad, on the front region of the face directly beneath the skin, partly covers the straplike zygomaticus minor and levator labii superioris muscles, giving the face its fleshy appearance. The malar fat pad is positioned close to the outer part of the orbicularis oris muscle (the round muscle of the mouth) near the nasolabial fold. While the pad often softens the surface in this area, it can appear as a triangular hollow or depression in a leaner face. In an elderly face, this fatty tissue usually sags, creating a much more pronounced nasolabial fold.
The buccal fat pad (or Bichart’s fat pad) is an deep, elongated fat pad positioned between the buccinator and masseter muscles. While we don’t usually see this fat pad on the surface, it does help fill in the spaces between the various muscles on the face.
Embedded within the superficial fascia of the neck is a very thin muscle called the platysma (see this page). On a young person this muscle is so thin that it is not noticeable unless activated in certain facial expressions or when the lower jaw is thrust forward. In the aging process this muscle loses its elasticity and begins to sag. The fatty tissue in the neck’s superficial fascia also begins to dissipate, becoming rather thin, unless the person has an abundance of fatty tissue, in which case the area under the chin and parts of the neck become thicker.
When someone has moderate to excessive layers of fat in the face and neck region, the submental fat pad under the chin can enlarge, producing what is colloquially known as a “double chin.” This extra fatty tissue often obscures the edge of the jawline as well, softening it to a curve. As a person ages, this fat pad tends to drop down slightly and bulge (herniate) between the divisions of the platysma muscle on the front of the neck, accentuating platysma banding.
A small amount of fatty tissue, called the suprasternal notch fatty tissue (or pit of the neck fat pad) occupies the suprasternal notch (pit of the neck), between the inner ends of the sternocleidomastoid tendons and the top portion of the sternum (breastbone). Generally there is not enough fat in this area to soften it out completely, so a small depression is still seen in the skin.
Fatty tissue sometimes accumulates in the area around the seventh vertebra at the base of the neck and in the mid upper back. This cervicodorsal fat pad (or dorsocervical fat pad) can become quite thick, appearing as a large bulge sometimes colloquially referred to as a “buffalo hump.” The cervicodorsal fat pad is more noticeable in obese people and the elderly (in both sexes, but mainly in females).
Fatty Tissues of the Torso
On the front of the female torso, the breasts are composed of mammary glands, fatty tissue, and connective tissue containing supportive fibrous ligaments. The fatty tissues in which the mammary glands are embedded (called breast fatty tissue or mammary fat tissue) give the breasts their overall shape. In the male chest, small, crescent-shaped pads of fatty tissue occur along the lower outer border of the pectoralis major muscle. In muscular men, these give an angular look to the forms of the chest, but in obese men, these pectoral fat pads, as well as the accumulation of excess adipose tissue generally, enlarge the forms of the chest into bulbous shapes similar in appearance to female breasts.
Breast shapes vary from woman to woman. They can be cone shaped, especially in young women, or melon shaped if there is an abundant amount of fatty tissue. In elderly women, breasts tend to look deflated, slumping on the rib cage, in part because the fatty tissue dissipates over the years.
Characteristics of the Breast
At the center of the breast form are the nipple and areola, shown in the following drawing. The nipple is a small cylindrical form projecting from the center of the areola, which is a ring of pigmented skin. The color of the areola varies among individuals, ranging from peachy and rosy colors to various shades of brown. The nipple contains an involuntary muscle which also affects the shape of the areola. In cooler temperatures, the nipple is erect and the areola contracts slightly. In warmer temperatures, the areola assumes its full disk shape and the nipple softens. In arousal, the nipple is erect and the areola is at its full shape. In males, the nipple and areola tend to be smaller and positioned lower on the chest form.
NIPPLE AND AREOLA OF BREAST
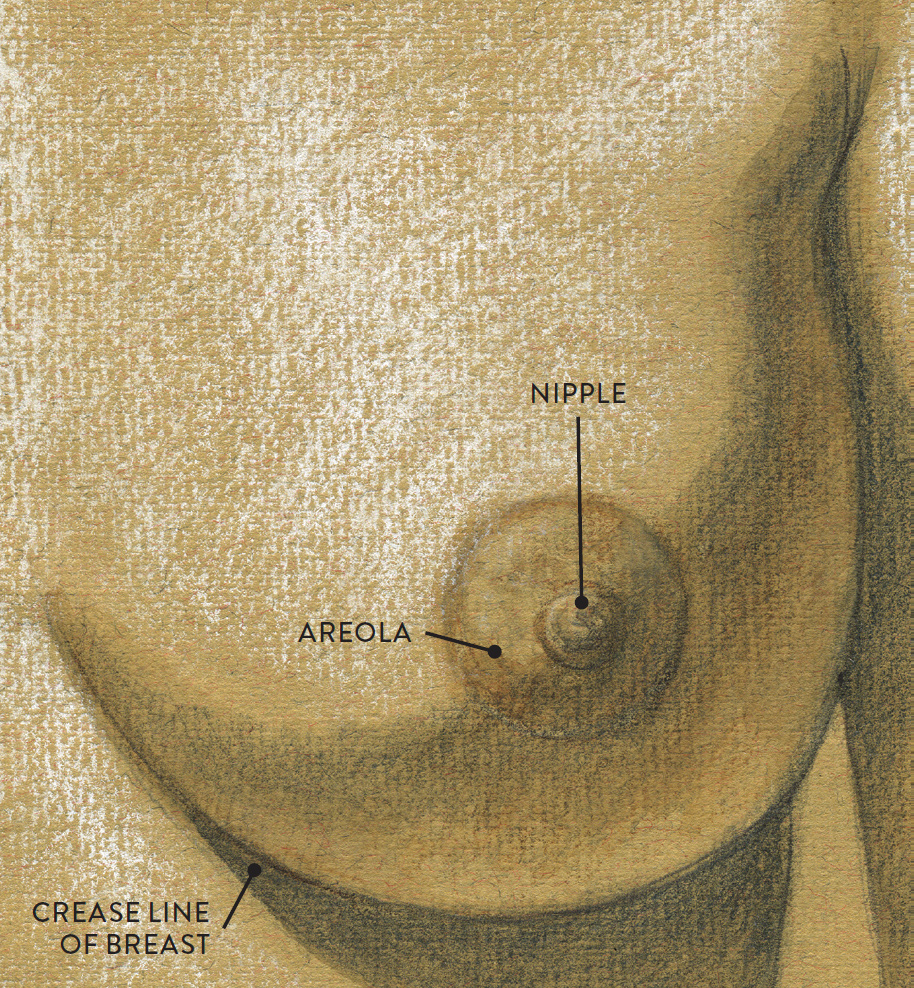
Left breast, anterior view
The breast form is quite movable on the rib cage and changes shape from pose to pose. When a woman lifts one arm overhead, the breast on that side stretches upward. If she is lying on her side, both breasts are affected by gravity and droop slightly downward. When she lies on her back, the breasts tend to flatten out from the midline, and the outer portions of the breasts roll outward, as shown in the life study Female Figure Leaning Back, below. Crossing the arms tightly in front of the torso presses the breasts closer together, forming a cleavage. If the woman leans forward, the breasts hang slightly away and downward from the rib cage, appearing pendulous. When the torso is vertical, with the arms at the sides, the breasts appear to gently fall away from the breastbone. Fatty tissue does not deposit directly on the breastbone, so there should always be a thin neutral space between the breasts. As just mentioned, however, gravity can affect the position of the breast, and its shape can cross over and in front of the breastbone in certain poses.
FEMALE FIGURE LEANING BACK
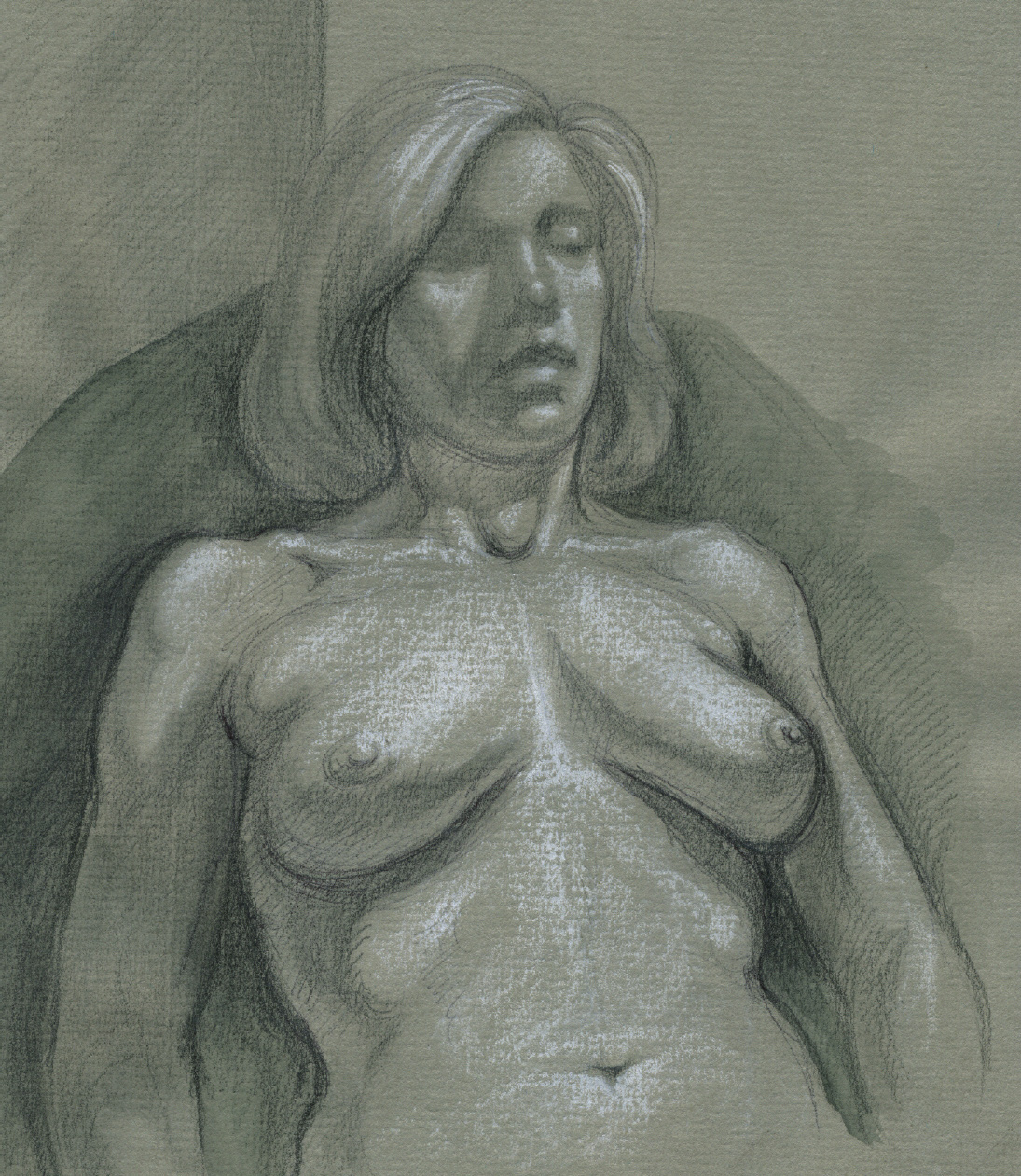
Graphite pencil, watercolor wash, and white chalk on toned paper.
The bulges at the outer sides of the lower torso below the waist are the flank pads of the external oblique muscle. A fat pad called the flank fat pad (or posterior fatty cushion) is located on the posterior lower portion of this muscle. When there is excessive fatty tissue present, the flank fat pad becomes larger, sometimes covering the entire lower portion of the external oblique muscle. Colloquial terms such as “spare tire” and “love handles” refer to excess fat on the sides of the waist around the flank portion. On women the flank fat pad surrounds the side of the torso, blending with the lateral gluteal fat pad (see this page), which covers the upper border of the pelvis (iliac crest). The anterior portion of the iliac crest (ASIS) is not covered by either muscle or fat and can usually be seen as a small bony protrusion or a dimple on the surface.
The lateral gluteal fat pad is located over the gluteus medius muscle, on or near the iliac crest of the pelvis. In individuals with substantial fatty tissue, the lateral gluteal pad merges with both the flank fat pad and the posterior gluteal fat pad, which is positioned directly over the gluteus maximus muscle, giving this area a smooth, rounded appearance. This fat pad does not cover the sacrum, sacral dimples, or greater trochanter of the femur.
On women, the posterior gluteal fat pad is usually more prominent than on men, blending with the lateral gluteal fat pad and the outer thigh fat pad to create a single mass. On more muscularly defined women, as on men, the posterior gluteal fat pad is relatively thicker in the lower region but minimal on the rest of the muscle. A furrow is sometimes noticeable immediately near the greater trochanter, which is where the gluteus maximus directly attaches into the iliotibial tract. But if the hip and upper leg have an excess amount of fatty tissue, this furrow is softened and hard to see. In the elderly, the fat in the buttock region dissipates and drops slightly downward as the connective tissue of the fascia loses its elasticity, resulting in the widening and flattening of the buttocks.
Embedded in the superficial fascia over each buttock is a slinglike fibrous tissue band called the buttock suspensory ligament. The fatty tissue contained by these slings gives the buttocks their characteristic shape. The gluteal fold (see this page) prevents the thick fatty tissue from moving downward against the hamstring muscles of the posterior upper leg, but some people have an extension of fatty tissue below the gluteal fold, referred to simply as the fat pad below the buttocks. If the fatty tissue is abundant in this area, there might be an additional skin crease (called the gluteal sulcus), and the fat pad’s shape can resemble a banana. When the upper leg bends, the fatty bulge and skin crease temporarily disappear.
Within the perimeter of the sacrum is a very thin deposit of fatty tissue referred to as the sacral fat pad (or lumbosacral fat pad). On some individuals this padding is slightly more abundant, creating a soft triangular shape within the sacrum region.
The abdominal fat pad (or Camper’s adipose layer) is subcutaneous fat located over the lower portion of the rectus abdominis muscle. It begins near the waist, surrounds the navel, and tapers toward the pubic bone, giving a soft appearance to the abdomen’s surface. In the presence of this superficial fat, the navel becomes a small, deep depression. Visceral fat (also called intra-abdominal fat or organ fat) is not subcutaneous fat; it is found in the abdominal cavity under the abdominal muscles. It serves as “packing material,” surrounding and supporting the organs. When there is an overabundance of this fat, as in extremely obese people, the abdomen significantly protrudes in what is colloquially called a “beer belly” or “potbelly.” The clinical term is abdominal obesity.
The life study Full-figured Female from the Side, shows how abundant fatty tissue is situated on the torso, especially in the pelvis region.
FULL-FIGURED FEMALE FROM THE SIDE
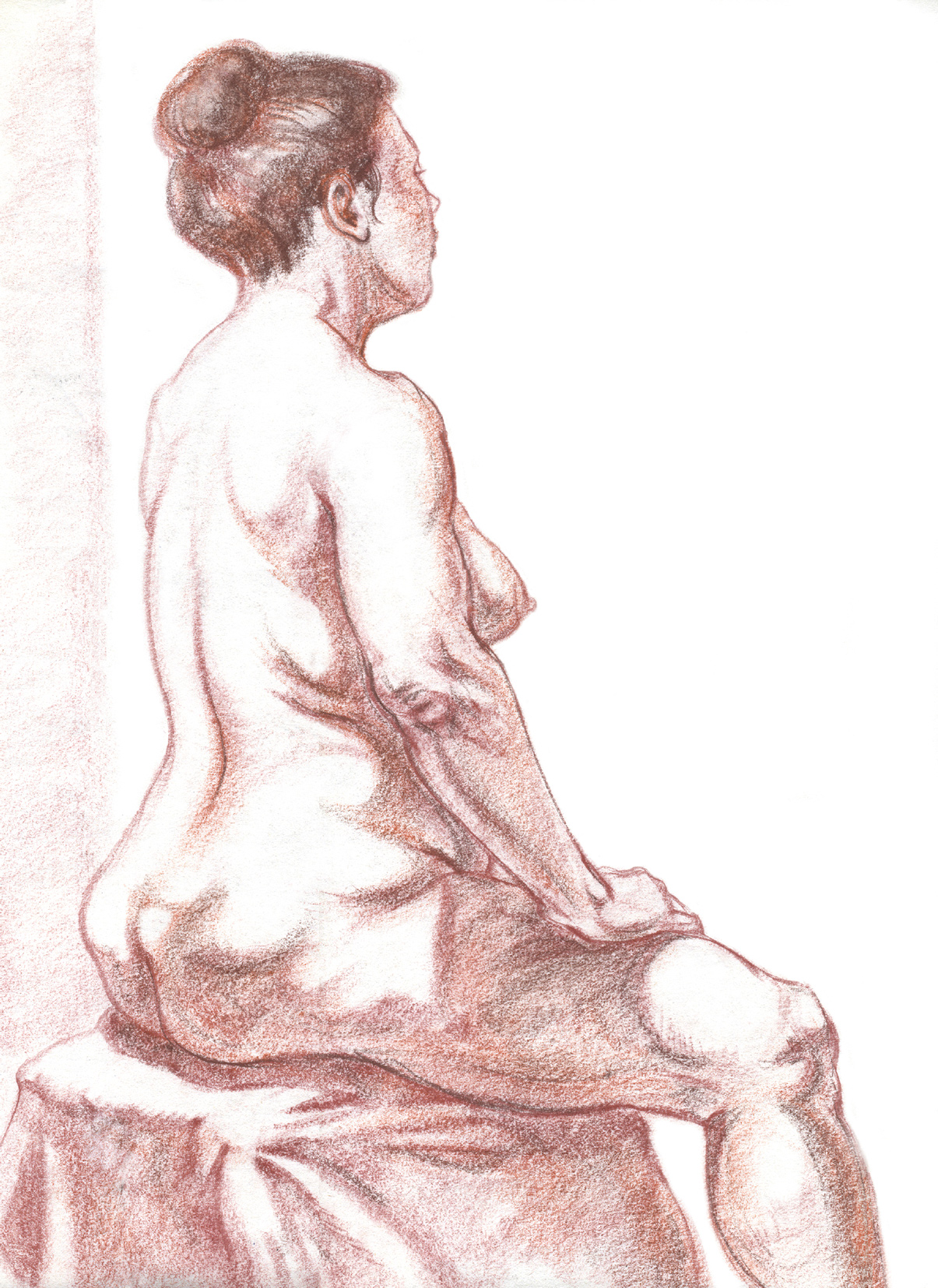
Sanguine and brown Conté crayon on newsprint.
A fat pad called the pubic fat pad (also known as the mons pubis, mons veneris, and mount of Venus) is positioned on top of the pubic bone and immediately below the inguinal ligament of the external oblique muscle, which attaches directly into the pubic bone. This pubic fat pad creates an obvious triangular shape in women. In men, the pubic fat pad is more subtle; it does, however, create a bridge of fatty tissue positioned directly beneath the inguinal ligament (the curving furrow from each ASIS to the pubic bone) and the line of the thigh (a skin fold that marks where the upper legs connect into the torso). In elderly men, this fat pad can become quite prominent, tending to sag downward.
Fatty Tissues of the Arm and Hand
There is usually a layer of fatty tissue located in the posterior upper arm region, around the outer head of the triceps muscle near the deltoid. This posterior upper arm fat pad tends to be more common in women.
Axillary fatty tissue (also called axilla fatty tissue or axillary fat) fills in the hollow of the armpit, covering the intersection of the several muscles that connect with the humerus in this location. This fatty tissue protects the nerves, blood vessels, and lymph nodes located in the armpit region.
The palm side of the hand is thick with muscular forms and fatty tissue, as shown in the following drawing, while the back of the hand shows very little evidence of fatty tissue. The palm’s superficial fascia consists of dense fibro-fatty tissue that is firmly attached to the palmar aponeurosis and covers the two muscle groups of the palm (the thenar group and the hypothenar group), serving as a protective padding for the palm area. There is also an elongated cushion of fibrous fat located at the base of the fingers on the palm side. Fat pads are also positioned on the palmar side of each finger, particularly in the vicinity of the fingertips, and on each thumb.
FAT PADS OF THE PALM
Study of Hand, Palm View

Graphite pencil, ballpoint pen, and sanguine colored pencil on white paper.
Diagram of fat pads
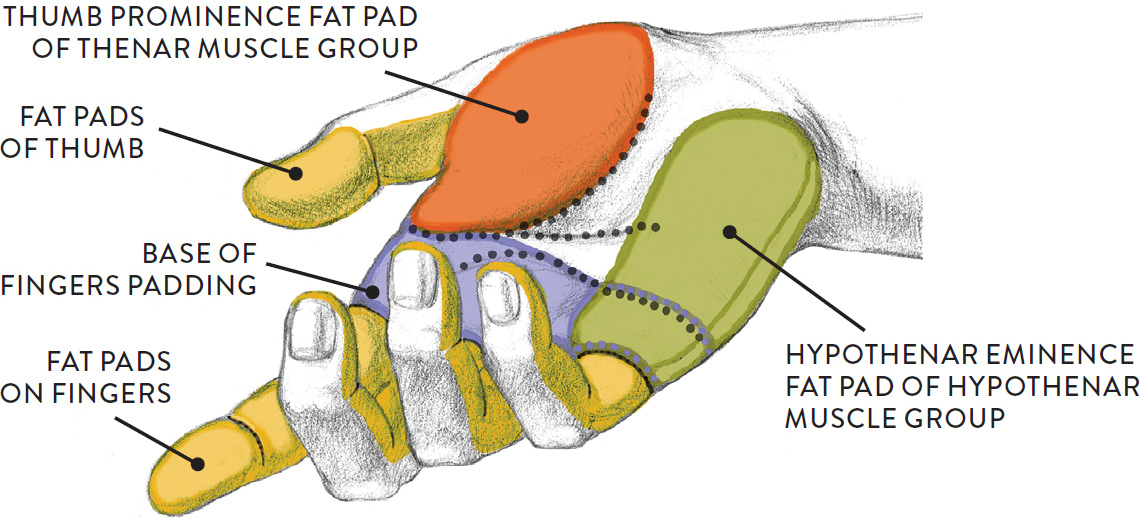
Diagram of fat pads
DOTTED LINES: FLEXOR CREASES OF PALM
Fatty Tissues of the Leg
The upper leg region has various fat pads, mainly on the inner and outer thighs, as well as in the knee region. On muscular legs, the fat layer is minimal, except perhaps around the knee joint.
STUDY OF A PAIR OF LEGS AND THE KNEE REGION
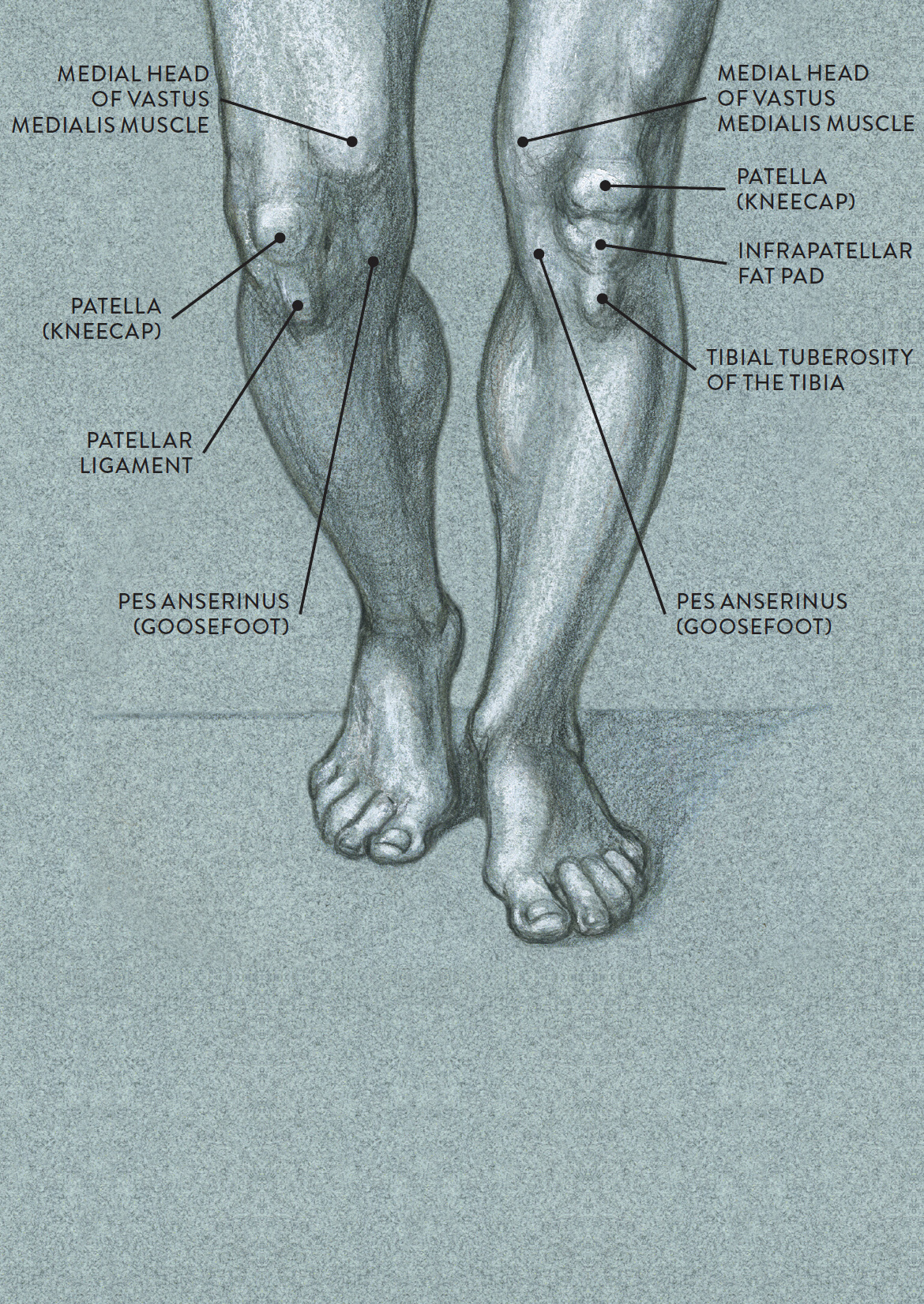
Ballpoint pen, graphite pencil, gray marker, and white chalk on toned paper.
The outer thigh fat pad (or subtrochanteric fat) is a fatty distribution covering a portion of the outer quadriceps muscle (vastus lateralis) and usually positioned below the greater trochanter bone of the femur. (This partly explains why we can see the knoblike form of the greater trochanter in many views of the leg.) In women, the outer thigh fat pad usually blends with the posterior gluteal fat pad, creating a continuous softened shape throughout the hip and buttock region and making women’s hips appear wider than men’s, sometimes resembling flaring riding breeches. Another fat pad, called the inner thigh fat pad, is located on the upper half of the inner thighs and covers part of the adductor muscles.
The infrapatellar fat pad (or fat pad of the knee) is located on the front of the leg directly below kneecap (patella). It is positioned behind the patellar ligament—the straplike form running from the patella to the tibial tuberosity of the tibia bone. When the leg is straight, this fat pad can be quite prominent in all body types, often resembling a softened heart-shaped form. When the leg bends, the patellar fat pad is no longer noticeable on the surface. Study of a Pair of Legs and the Knee Region, on this page, shows the infrapatellar fat pad and other surface landmarks of the knee region.
At the back of the knee region is a diamond-shaped hollow, called the popliteal fossa, between the tendons of the hamstring muscles and the upper portion of the calf muscle (gastrocnemius). Within this hollow is a small pad of fat, called the popliteal fat pad, that acts as a cushion for the joint and helps protect the nerves and blood vessels in this space. When the leg is straight, the fat pad appears as a bulge positioned directly above the back-of-the-knee crease and between the hamstring tendons. Shallow vertical grooves appear in the skin next to the tendons on either side of the bulging fat pad. When the leg bends, the fat pad disappears from view and a deep hollow is seen, along with the prominent hamstring tendons. The differing appearances of this region are shown in the following drawing.
POPLITEAL FOSSA AND POPLITEAL FAT PAD
Bent leg shows hollow in popliteal fossa.
POPLITEAL FOSSA AND POPLITEAL FAT PAD (CONTINUED)
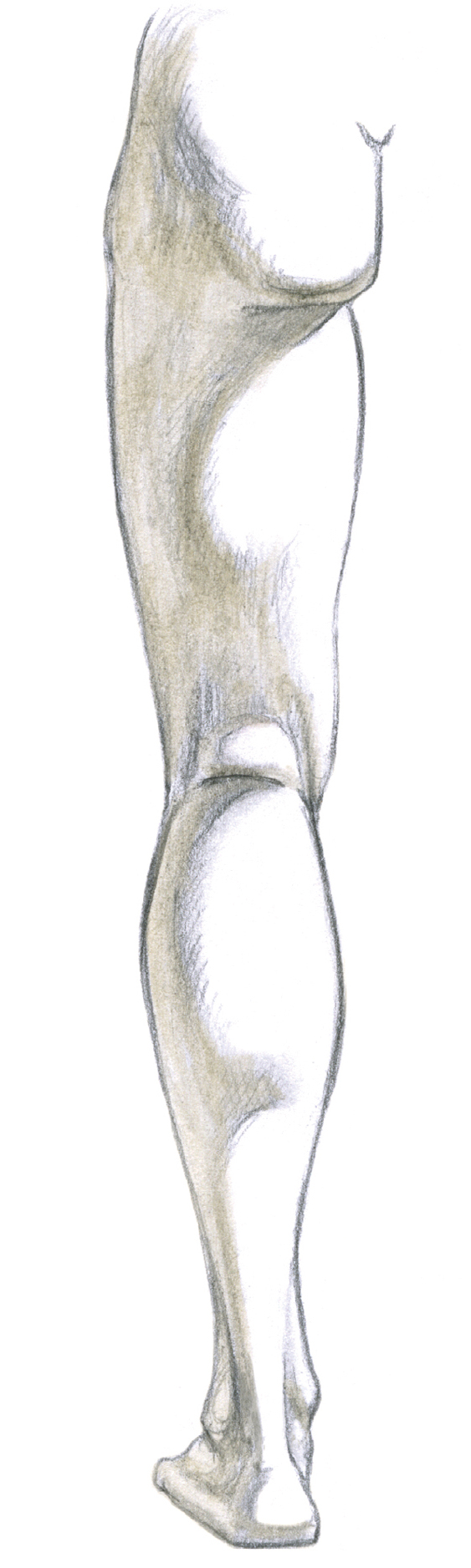
Straight leg shows fat pad in popliteal fossa.
POPLITEAL FOSSA AND POPLITEAL FAT PAD (CONTINUED)
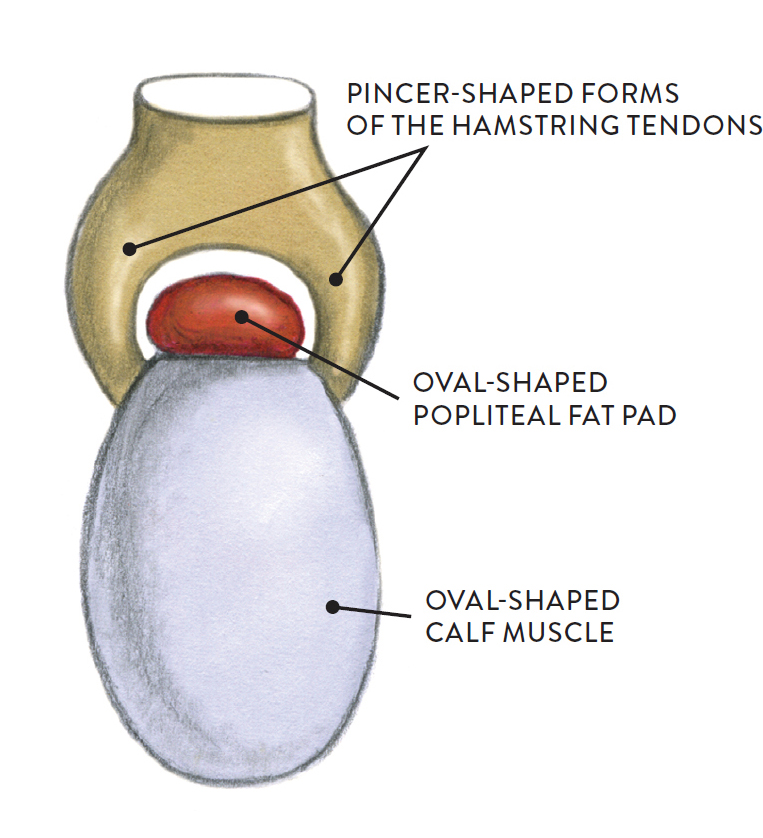
Basic shapes for back of knee region.
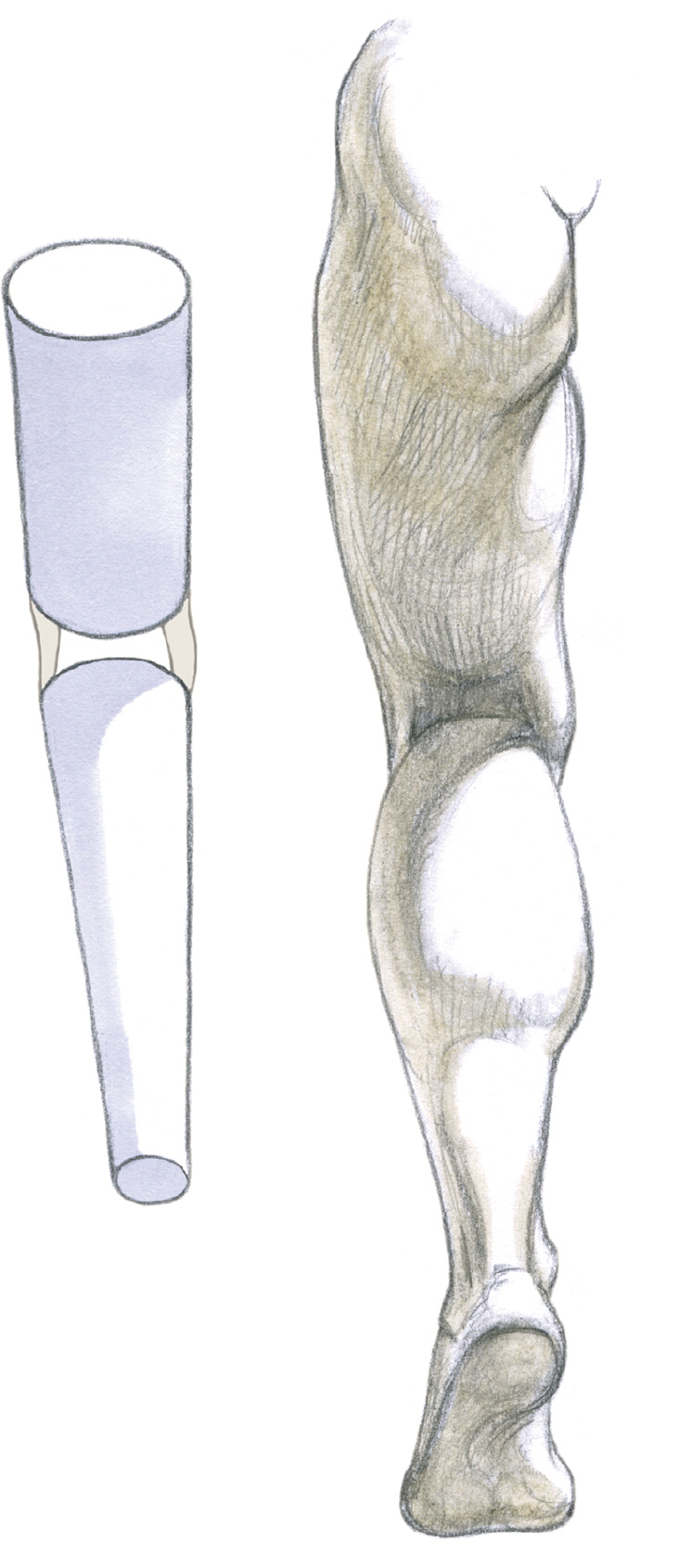
On the inner side of the knee is the attachment site for three tendons from the sartorius, gracilis, and semitendinosus muscles. These tendons wrap around the inner condyles of the femur and tibia and form a tendinous triangle called the pes anserinus, meaning “goosefoot.” (The tendons’ webbed appearance is similar to the foot of a goose.) Small sacs of fluid (pes anserinus bursa) are positioned between the tendons, giving this area a slightly thickened form. On some individuals (especially women), a pad of fatty tissue (the goosefoot fat pad) is distributed over the tendons of the pes anserinus, creating a large egglike shape on the surface, especially in a standing leg. This surface form is positioned slightly lower than the inner head of the vastus medialis muscle of the quadriceps. When the leg bends at the knee, the fatty tissue becomes less prominent or completely disappears, revealing the medial condyles of the femur and tibia bones.
A small amount of fatty tissue called the Kager’s fat pad (or pre-Achilles fat pad) occupies the triangular space called the Kager’s triangle between the Achilles tendon, the top portion of the calcaneus (heel bone) and the posterior edge of the flexor hallucis longus muscle and its tendon.
The several fat pads of the sole of the foot have already been introduced, above (see this page).
SITTING FIGURE DEPICTED IN PLANES
Pen and gray markers on white paper.