Biology of Humans
16. The Urinary System
In Chapter 15a we learned that water is perhaps the most important nutrient. Indeed, while we can survive for several weeks without food and its component nutrients (such as fats, proteins, and carbohydrates), most people survive only a few days without water. In this chapter we focus on the urinary system and maintenance of fluid balance in the body. Specifically, we consider the critical roles that kidneys play in maintaining homeostasis by removing wastes from the body and regulating the volume, solute concentration, and pH of blood.
Eliminating Waste
Excretion is the elimination of wastes and excess substances from the body. Metabolic wastes include carbon dioxide, water, heat, salts, and nitrogen-containing molecules such as ammonia, urea, uric acid, and creatinine. Kidneys and other organs that eliminate metabolic wastes help to maintain homeostasis.
The organs that eliminate wastes and excess essential ions—such as hydrogen (H+), sodium (Na+), potassium (K+), and chloride (Cl-)—are shown in Figure 16.1. Lungs and skin eliminate heat, water, and carbon dioxide (as the gas CO2 from the lungs and as bicarbonate ions, HCO3-, from the skin). Skin also excretes salts and small amounts of urea and uric acid.
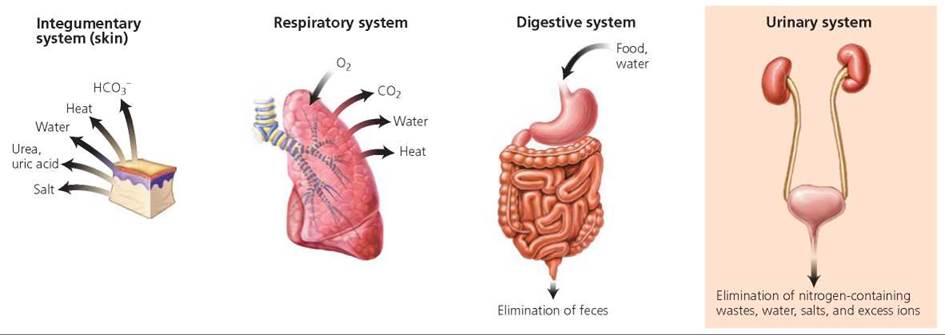
FIGURE 16.1. Organs from several systems eliminate wastes of different kinds from the body. The kidneys, organs of the urinary system, play a major role in the excretion of nitrogen- containing wastes, water, salts, and excess ions.
Minor amounts of other substances, such as alcohol, are also eliminated from the skin and lungs. (Alcohol excretion by the lungs forms the basis of the breathalyzer test.) Organs of our gastrointestinal tract eliminate solid wastes and some metabolic wastes. Defecation is the elimination of feces from the digestive tract. Feces contain undigested food, bacteria, water, bile pigments, and sloughed-off epithelial cells (see Chapter 15).
· Proper fluid balance is critical to homeostasis. We challenge the balance of fluids in our bodies through diet and exercise. In the face of such challenges, our kidneys help to achieve the correct balance by filtering the blood and regulating its volume and solute concentration.
Our focus in this chapter is the kidneys, which are the organs of the urinary system that form urine. Urine, a yellowish fluid, is a mix of water and solutes. Through urine, the body excretes water, salts, excess ions, urea, uric acid, and creatinine. Ammonia is formed in the liver during the breakdown of amino acids. Because ammonia is toxic, the liver converts it to urea, a less harmful waste. Uric acid is formed during the recycling of nitrogen-containing bases of nucleotides (see Chapter 2). In excess, uric acid may form crystals in the synovial fluid of joints (particularly in the big toe), causing the painful condition called gout. Creatinine is generated in skeletal muscle from the breakdown of creatine phosphate, a compound that serves as an alternative energy source for muscle contraction.
Components of the Urinary System
The urinary system consists of two kidneys, two ureters, one urinary bladder, and one urethra (Figure 16.2). The main function of this system is to regulate the volume, pressure, and composition of the blood. The kidneys are the organs of the urinary system that accomplish this task by regulating the amount of water and dissolved substances that are removed from and returned to the blood. Substances not returned to the blood form urine.

FIGURE 16.2. Organs of the urinary system (labeled on the left side) and their relation to major blood vessels (identified on the right side)
Urine from the kidneys travels down muscular tubes called ureters to the urinary bladder. Each ureter is 25 to 30 cm in length. Peristaltic (wavelike) contractions begin where the ureters leave the kidneys and travel down the ureters, pushing urine toward the urinary bladder. Depending on the rate of urine formation, up to five peristaltic waves occur per minute. Each ureter enters the urinary bladder through a slit-like opening. The urinary bladder is a muscular, expandable organ that temporarily stores urine until it is excreted from the body. Urine leaves the body through the urethra, a tube that transports urine from the urinary bladder to the outside of the body through an external opening. The female urethra transports only urine. The male urethra, however, carries urine and reproductive fluids (but not simultaneously). The reproductive function of the male urethra is discussed in Chapter 17.
What would you do?
In the United States, bladder cancer is the fifth most common cancer and one of the 10 most deadly. Because it tends to recur, long-term monitoring of patients is essential. This makes bladder cancer costly; in fact, it ranks fifth among all cancers in total costs. Despite these statistics, bladder cancer receives relatively little national attention. It also receives comparatively few resources. When compared with breast, colorectal, prostate, and lung cancer, bladder cancer ranked last in research funding per case in 2007. If you were given the responsibility of deciding how to allocate funds for research on different diseases, what would you base your decision on? Would you consider incidence, risk of death, or cost? What about the potential for improvements in prevention, diagnosis, and treatment?
Kidneys and Homeostasis
Our kidneys are reddish brown in color and shaped like kidney beans. Each one is about the size of a fist. They are located just above the waist, sandwiched between the parietal peritoneum (the membrane that lines the abdominal cavity) and the muscles of the dorsal body wall. The slightly indented, or concave, border of each kidney faces the midline of the body. Perched on top of each kidney is an adrenal gland.
The kidneys are covered and supported by several layers of connective tissue (Figure 16.3). The outermost layer is a tough, fibrous layer that anchors each kidney and its adrenal gland to the abdominal wall and surrounding tissues. Beneath this layer is a protective cushion of fat (the middle connective tissue layer, also called the adipose capsule). The innermost layer covering the kidneys is a layer of collagen fibers that protects the kidneys from trauma.

FIGURE 16.3. Structure of the kidney
Structure of the Kidneys
One ureter leaves each kidney at a notch in the concave border, as shown in Figure 16.3. This notch is also the area where blood vessels enter and exit the kidney. The renal arteries branch off the aorta and carry blood to the kidneys. The renal veins carry filtered blood away from the kidneys to the inferior vena cava, which transports the blood to the heart.
Each kidney has three regions: an outer region, the renal cortex;a region enclosed by the cortex, the renal medulla; and an inner chamber, the renal pelvis (see Figure 16.3). The renal cortex begins at the outer border of the kidney, and portions of it, called renal columns, extend inward between the pyramid-shaped subdivisions (renal pyramids) of the renal medulla. The narrow end of each renal pyramid joins a cuplike extension of the renal pelvis. As we will soon see, urine produced by the kidneys eventually drains into the renal pelvis and out the ureter to the urinary bladder.
Nephrons
Nephrons are the microscopic functional units of the kidneys and are responsible for the formation of urine. Each kidney contains 1 million to 2 million nephrons.
Structure of nephrons. A nephron has two basic parts: the renal corpuscle and the renal tubule, as shown in Figure 16.4. The renal corpuscle is the portion of the nephron where fluid is filtered from the blood. It consists of a tuft of capillaries, the glomerulus;and a surrounding cuplike structure, the glomerular capsule (sometimes called Bowman's capsule). Within the glomerular capsule is a space that is continuous with the lumen of the renal tubule. Blood enters a glomerulus by an afferent (incoming) arteriole. Inside the glomerular capillaries, water and small solutes move from the blood into the space within the glomerular capsule and then into the renal tubule, where they are considered filtrate (a fluid similar to blood plasma but typically lacking proteins). The blood then leaves the glomerulus by an efferent (outgoing) arteriole. The renal tubule is the site where substances are removed from and added to the filtrate. This tubule has three sections: the proximal convoluted tubule, the loop of the nephron (sometimes called the loop ofHenle), and the distal convoluted tubule. The proximal convoluted tubule, its name reflecting its location nearest the glomerular capsule, has cells with many tiny projections called microvilli. Microvilli allow the efficient removal (reabsorption) of useful substances from the filtrate, which are eventually returned to the blood (see later in this discussion). The loop of the nephron resembles a hairpin turn, with a descending limb and an ascending limb. Next comes the distal convoluted tubule, its name reflecting this section's more distant location from the glomerular capsule. The loop of the nephron and the distal convoluted tubule have cells with few or no microvilli. The distal convoluted tubules of many nephrons empty into a single collecting duct; many collecting ducts eventually drain into the renal pelvis. The renal pelvis is connected to the ureter. Urine exits the kidney by way of the ureter and moves into the urinary bladder.

FIGURE 16.4. Structure of the nephron
About 80% of the nephrons in our kidneys are confined almost entirely to the renal cortex; they have short loops that dip only a short distance into the renal medulla. The remaining 20% have long loops that extend from the cortex deep into the renal medulla. Once in the medulla, the loops of these nephrons turn abruptly upward, back into the cortex, where they lead into distal convoluted tubules. As we will see, the nephrons whose loops extend deep into the medulla play an important role in water conservation.
Functions of nephrons. The kidneys are crucial for maintaining homeostasis. For one thing, they filter wastes and excess materials from the blood. Indeed, over the course of one day, two healthy kidneys filter all the blood in the body 30 times! They also assist the respiratory system in the regulation of blood pH. Finally, the kidneys maintain fluid balance by regulating the volume and composition of blood and urine.
To understand what occurs in the kidneys, we must examine the work of nephrons. Nephrons perform three functions: (1) glomerular filtration, (2) tubular reabsorption, and (3) tubular secretion.
We can compare these functions to the steps you might take during a selective cleaning of small items from your bedroom closet. First, you might remove almost all of the small items—the valuable along with the unwanted. This activity is analogous to glomerular filtration, which removes from the blood all materials small enough to fit through the pores of the kidney's filter (discussed next). The next step in cleaning your closet might be to look through the various items you have removed and put back "the good stuff," the items worth saving. Returning valuable materials to the closet is analogous to tubular reabsorption, which returns useful materials to the blood. The final step in cleaning the closet might be to once again scan what you have in your closet and to selectively remove items, such as those in excess. This last step is analogous to tubular secretion, in which wastes and excess materials are removed from the blood and added to the filtrate that will eventually leave the body as urine. Secretion also removes from the blood substances not naturally found in the body, such as pesticides and certain drugs. Here are the three steps in more detail.
1. Glomerular filtration occurs as blood pressure forces water and small solutes from the blood in the glomerulus to the space inside the glomerular capsule (Figure 16.5). Reaching the space inside the glomerular capsule requires passing sequentially through the following three layers: (1) the single layer of endothelial cells that forms the walls of the capillaries, (2) the basement membrane just outside the capillary walls, and (3) the epithelial lining of the glomerular capsule.
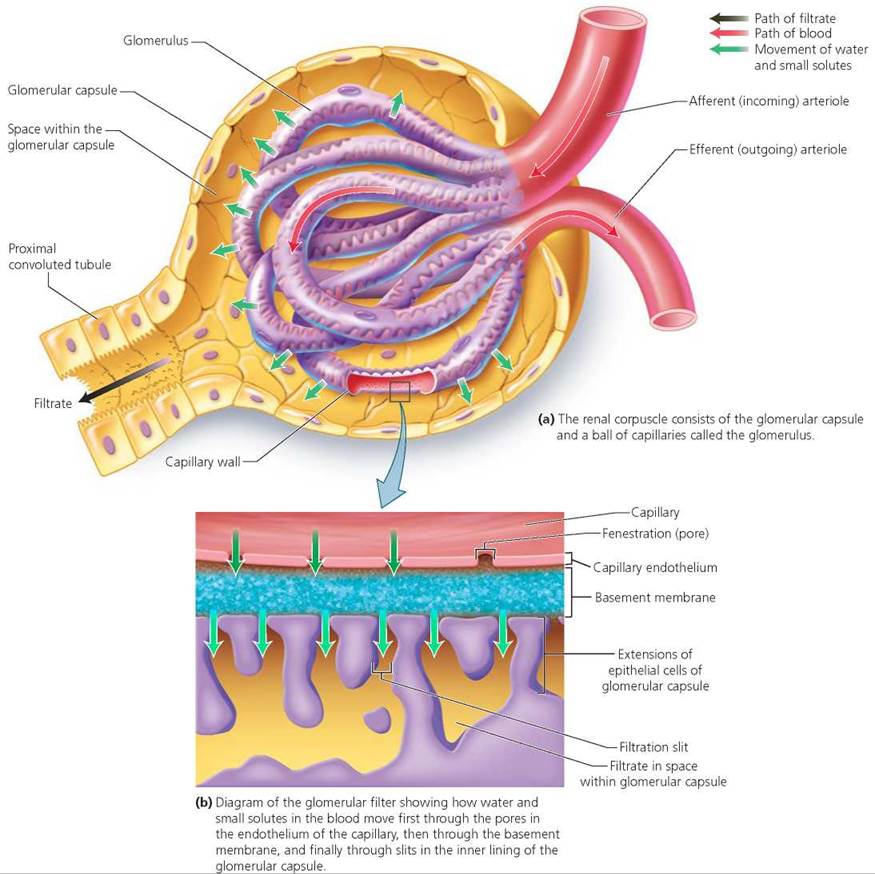
FIGURE 16.5. The renal corpuscle is the site of glomerular filtration.
Water and small solutes in the blood first move through the walls of the glomerular capillaries. The capillary walls consist of a single layer of endothelial cells; the walls of these capillaries are fenestrated, meaning they have many pores. The pores allow some substances to move out of the capillaries, but prevent red blood cells from doing so. Next, the filtered substances cross the basement membrane, a layer of protein fibers in a glycoprotein matrix. This layer restricts the passage of large proteins. Finally, the filtered substances pass through slits in the inner lining of the glomerular capsule; these slits occur in between extensions of the epithelial cells of the capsule (refer, again, to Figure 16.5). These substances are known collectively as glomerular filtrate. The concentrations of the molecules dissolved in the glomerular filtrate are approximately the same as in the blood plasma.
Several things can change the rate of filtration by the glomerulus. An increase in the diameter of afferent (incoming) arterioles brings more blood into the glomerulus and produces higher pressure in the glomerular capillaries. Higher pressure results in higher filtration rates (more filtrate produced by the kidneys each minute). A reduction in the diameter of efferent (outgoing) arterioles also produces higher pressure in glomerular capillaries and higher filtration rates. General (systemic) increases in blood pressure can also produce higher filtration rates.
2. Tubular reabsorption is the process that removes useful materials from the filtrate and returns them to the blood. This process occurs in the renal tubule, primarily in the proximal convoluted tubule. The characteristics of the cells lining the proximal convoluted tubule make it an ideal location for reabsorption (Figure 16.6). As mentioned, these epithelial cells have numerous microvilli (projections of the plasma membrane) that reach into the lumen of the tubule. Similar in function to the microvilli in the small intestine, these microvilli dramatically increase the surface area for the reabsorption of materials. Reabsorption returns water, essential ions, and nutrients to the blood (see Table 16.1). Remarkably, as the glomerular filtrate passes through the renal tubule, about 99% of it is returned to the blood in the surrounding capillaries. Thus, only about 1% of the glomerular filtrate is eventually excreted as urine. Put another way, of the approximately 180 liters (48 gal) of filtrate that enter the glomerular capsule each day, between 178 and 179 liters (47 gal) are returned to the blood by reabsorption. The remaining 1 to 2 liters (about 0.5 to 1 gal) are excreted as urine. Imagine how much water and food we would have to consume if we did not have reabsorption to offset the losses from glomerular filtration! Some wastes are not reabsorbed at all, and will eventually be excreted; others, such as urea, are partially reabsorbed. We will see that antidiuretic hormone (ADH), manufactured by the hypothalamus and released by the posterior pituitary gland, regulates the amount of water reabsorbed in parts of the renal tubule.
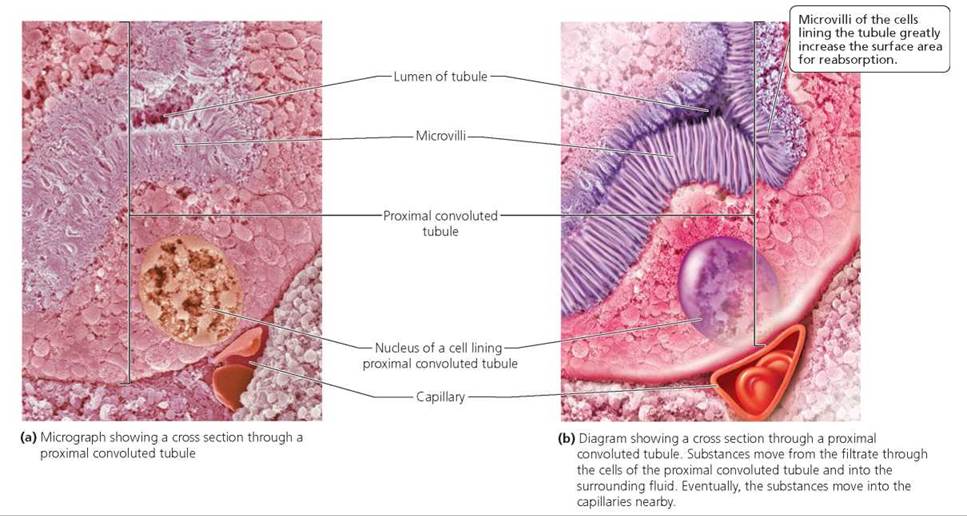
FIGURE 16.6. The proximal convoluted tubule is the site of tubular reabsorption.
TABLE 16.1. Reabsorption by Nephrons of Some Substances
|
Substance |
Amount filtered per day (in liters or grams) |
% Reabsorbed (removed from filtrate and returned to blood) |
|
Water |
180 L |
99 |
|
Glucose |
180 g |
100 |
|
Urea |
52 g |
50 |
|
Creatinine |
1.6 g |
0 |
|
Sodium ions (Na+) |
620 g |
99 |
|
Potassium ions (K+) |
30 g |
93 |
|
Bicarbonate (HCO3-) |
275 g |
100 |
3. Tubular secretion removes additional wastes and excess ions from the blood. For example, hydrogen ions (H+), potassium ions (K+), and ammonium ions (NH4+) in the blood are actively transported into the renal tubule, where they become part of the filtrate to be excreted. Tubular secretion also removes foreign substances from the blood, including pesticides and drugs such as penicillin, cocaine, and marijuana. These substances are added to the filtered fluid that will become urine. Tubular secretion occurs along the proximal and distal convoluted tubules and collecting duct.
The regions of the nephron and their roles in filtration, reabsorption, and secretion are shown in Figure 16.7 and reviewed in Table 16.2. When reviewing these, keep in mind the directions that substances move in each of the three processes: (1) during glomerular filtration, substances move from the blood into the nephron to form filtrate; (2) during tubular reabsorption, useful substances move from the filtrate within the nephron back into the blood; (3) during tubular secretion, drugs and substances in excess move from the blood into the filtrate.
TABLE 16.2. Review of Nephron Regions and Their Roles
|
Region of Nephron |
Roles* |
|
Renal corpuscle (glomerular capsule and glomerulus) |
Filters the blood, removing water, glucose, amino acids, ions, nitrogen-containing wastes, and other small molecules |
|
Proximal convoluted tubule |
Reabsorbs water, glucose, amino acids, some urea, Na+, Cl-, and HCO3 - |
|
Secretes drugs, H+, NH4+ |
|
|
Loop of the nephron |
Reabsorbs water, Na+, Cl , and K+ |
|
Distal convoluted tubule |
Reabsorbs water, Na+, Cl-, and HCO3- |
|
Secretes drugs, H+, K+, and NH4+ |
*Major reabsorbed or secreted substances are listed here.
By the end of glomerular filtration, tubular reabsorption, and tubular secretion, blood leaving the kidneys contains most of the water, nutrients, and essential ions that it contained upon entering the kidneys. Wastes and excess materials have been removed, leaving the blood cleansed. This purified blood now moves from the capillaries surrounding the nephron into small veins that eventually join the renal vein.
The final filtrate, now called urine, contains all of the materials that were filtered from the blood and not reabsorbed, plus substances that were secreted from the blood. Urine empties from the distal convoluted tubules into collecting ducts. There, more water may be reabsorbed, and some additional removal of excess substances, such as hydrogen and potassium ions, also occurs. From the collecting ducts, urine moves into the renal pelvis and leaves each kidney through a ureter. It then travels down the ureters to the urinary bladder, which stores the urine until it is eliminated from the body through the urethra. The precise composition of urine can be examined in a medical laboratory. See the Health Issue essay, Urinalysis.
Acid-Base Balance
In addition to removing wastes and regulating the volume and solute concentration of blood plasma, the kidneys help regulate the pH of blood. Recall from Chapters 2 and 14 that blood pH must be regulated precisely for proper functioning of the body. This precise regulation is achieved through the actions of the kidneys, through buffer systems in the blood, and through respiration. Buffer systems regulate pH by picking up hydrogen ions (H+) when their concentrations are high and releasing hydrogen ions when their concentrations are low. Chapter 2 described the importance of carbonic acid as such a buffer in the blood. The role of the kidneys in maintaining pH is twofold. First, by secreting hydrogen ions into the urine, the kidneys remove excess hydrogen ions from the blood, thereby increasing blood pH. Second, the kidneys help sustain the carbonic acid buffer system by returning bicarbonate to the blood. Because of their role in regulating blood pH, the kidneys ultimately influence breathing rate. Recall from Chapter 14 that chemoreceptors in the medulla of the brain respond to changes in the pH of blood (and cerebrospinal fluid) by adjusting breathing rate.
Water Conservation
Our kidneys enable us to conserve water through the production of concentrated urine. Because of their role in water conservation, the kidneys participate in the maintenance of cardiac output and blood pressure. Production of concentrated urine is performed by the 20% of our nephrons with long loops that dip deep into the renal medulla. The special ability of these nephrons to concentrate urine derives from an increasing concentration of solutes in the interstitial fluid (the fluid that fills the spaces between cells) from the cortex to the medulla of the kidneys. The most important of these solutes are sodium chloride (NaCl) and urea. Let's explore this mechanism for urine concentration by tracing the path of the filtrate as it flows through these long loops (Figure 16.8).
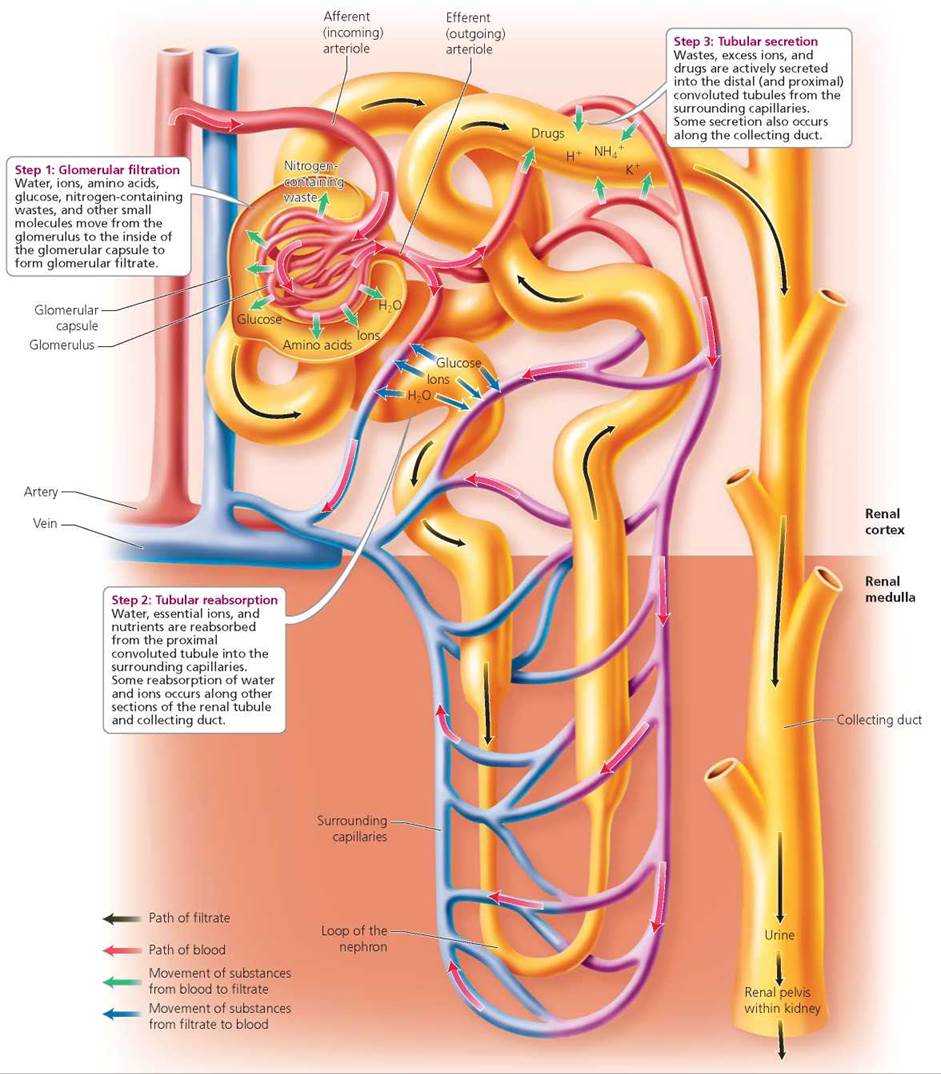
FIGURE 16.7. Overview of glomerular filtration, tubular reabsorption, and tubular secretion along the nephron
How does the structure of glomerular capillaries aid filtration?
The walls of glomerular capillaries have pores that allow many substances (but not red blood cells) to move out of the capillaries.
Health Issue
Urinalysis
The kidneys are our body's filtering system, so the urine they produce contains substances that originate from almost all of our organs. A detailed analysis of our urine, therefore, tells us not only how the organs of our urinary tract are functioning but also about the general health of our other organs. In other words, a typical urinalysis, which assesses the physical and chemical properties of urine and evaluates whether microorganisms are present, provides an overview of a person's basic health.
Healthy urine exiting the body typically contains no microorganisms. The presence of bacteria in a properly collected urine sample usually signals infection of the urinary system. Bacteria found in a sample may be cultured to determine their identity, which can help in diagnosing the infection. Urine also may be screened for fungi or protozoans that cause inflammation within the urinary tract.
Sometimes a urine sample is contaminated because of improper collection. For example, if the perineal area has not been cleaned and the collection cup or urine is allowed to contact that area, bacteria may be introduced. (In males, this is the area between the anus and scrotum; in females, it is between the anus and vulva.) It is therefore important to be careful when collecting a urine sample.
The following physical characteristics are routinely checked in urine analyses: color; turbidity (cloudiness); pH; and specific gravity, or density, of urine (the ratio of its weight to the weight of an equal volume of distilled water). The color of urine comes from urochrome, a yellow pigment produced as a waste product by the liver during the breakdown of hemoglobin in red blood cells. The urochrome travels in the bloodstream from the liver to the kidneys, where it is filtered from the blood and excreted with urine. The color of urine varies somewhat according to diet. Beets, for example, lend urine a red color, and asparagus causes a green tinge. The color of urine also varies with concentration. More concentrated urine, such as that collected first thing in the morning, is darker than more dilute urine. An abnormal color of urine—particularly red, when followed by microscopic confirmation of the presence of red blood cells—can indicate trauma to urinary organs.
Freshly voided urine is usually transparent. Cloudy, or turbid, urine may indicate a urinary tract infection, particularly if white blood cells are detected. Healthy urine has a pH of about 6, although considerable variation may occur in response to diet. High-protein diets produce acidic urine, and vegetarian diets produce alkaline urine. An alkaline pH also is associated with some bacterial infections. Specific gravity is a measure of the concentration of solutes in urine and therefore of the concentrating ability of the nephrons within our kidneys. When urine becomes highly concentrated for long periods, substances such as calcium and uric acid may precipitate out and form kidney stones.
Quantitative chemical tests are run to assess the levels of specific chemical constituents of urine. The major constituent is water, making up about 95% of the total volume. The remaining 5% consists of solutes from the metabolic activities of our cells or from outside sources (such as drugs). Tests run on urine samples look for certain abnormal constituents of urine (such as glucose, red blood cells, or white blood cells) and for normal constituents present in abnormal amounts (such as higher-than-normal amounts of protein).
Questions to Consider
• Why would it be important for a woman to inform her doctor that she is menstruating at the time of urine collection?
• Urinalysis is often preferred over blood testing in workplace drug-testing programs. What might explain this preference?
The solute concentration of the filtrate passing from the glomerular capsule to the proximal tubule is about the same as that of blood. As the filtrate moves through the proximal convoluted tubule, large amounts of water and salt are reabsorbed (recall from our earlier discussion of reabsorption that nutrients are also reabsorbed at this time). This reabsorption produces dramatic reductions in the volume of filtrate but little change in its solute concentration (because both water and salt are reabsorbed). However, when the filtrate enters the descending limb of the loop of the nephron, major changes in solute concentration begin (Figure 16.8). This path takes it from the cortex to the medulla.
Along the descending limb, water leaves the filtrate by osmosis (a special type of diffusion described in Chapter 3). The departure of water creates an increase in the concentration of solutes, including sodium chloride, within the filtrate. The concentration of salt in the filtrate peaks at the curve of the loop, setting the stage for the next step in the process of urine concentration. Now the filtrate moves up the ascending limb of the loop. As it does so, large amounts of sodium chloride are actively transported out of the filtrate into the interstitial fluid of the medulla. Water, however, remains in the filtrate because the ascending limb is not permeable to water. When the filtrate reaches the distal convoluted tubule in the cortex, it is quite dilute. In fact, the filtrate is hypotonic to body fluids. (Recall from Chapter 3 that hypotonic means having a lower solute concentration than another fluid. Hypertonic means having a greater solute concentration than another fluid. Isotonic means having the same solute concentration as another fluid.) The filtrate then moves into a collecting duct and begins to descend once again toward the medulla. This pathway is one of increasing salt concentration in the interstitial fluid because of all the salt that was transported out of the filtrate as it ascended the loop. Collecting ducts are permeable to water but not to salt (antidiuretic hormone increases the permeability of the collecting duct to water; see Figure 16.8). Thus, as the filtrate encounters increasing concentrations of salt in the fluid of the inner medulla, water leaves the filtrate by osmosis. With this departure of large amounts of water, urea is now concentrated in the filtrate. In the lower regions of the collecting duct, some of the urea moves into the interstitial fluid of the medulla. This leakage of urea contributes to the high solute concentration of the inner medulla and thus aids in concentrating the filtrate. The remaining urea is excreted.
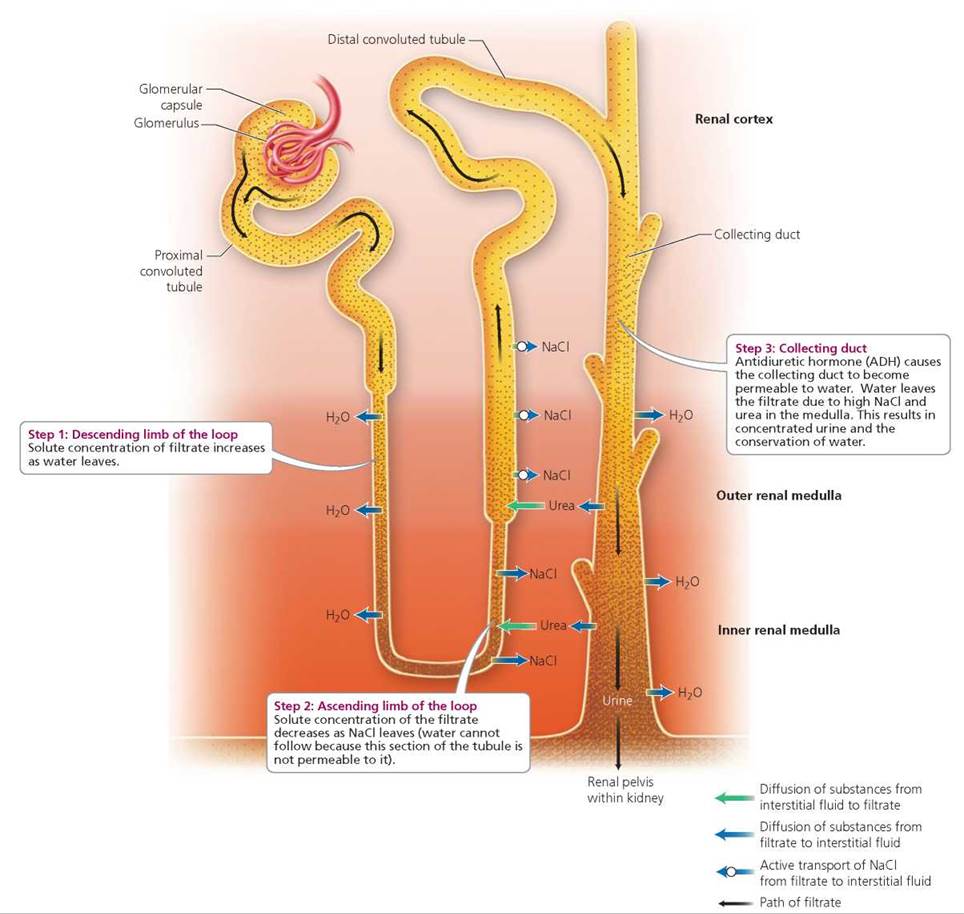
FIGURE 16.8. Some nephrons have loops that extend deep into the medulla. These nephrons are responsible for water conservation. The steps by which these nephrons concentrate urine and conserve water are shown here. Stippling indicates solute concentration of the filtrate within the nephron and collecting duct. The color gradient behind the nephron and collecting duct indicates solute concentration in the interstitial fluid of different regions of the kidney (renal cortex, and outer and inner renal medulla; darker is more concentrated).
At its most concentrated, urine is hypertonic to blood and interstitial fluid from any other part of the body except the inner medulla, where it is isotonic. Together, the loop of the nephron and collecting duct maintain extraordinarily high solute concentrations in the interstitial fluid of the kidneys, making possible the concentration of urine and conservation of water by the kidneys.
Hormones and Kidney Function
Our health depends on our keeping the salt and water levels in our body near certain optimum values. This, as we have seen, is an important job of the kidneys. It is also a challenging job, because our activities produce constant fluctuations in those levels. For example, on a hot day or after exercise, we may lose body water and salts through perspiration. In contrast, eating a tub of salted popcorn at the movies can boost our salt intake. The kidneys must deal with these challenges and adjust the concentration of solutes in the urine and in the blood to keep water and salt levels in our body relatively constant.
Three hormones—ADH, aldosterone, and atrial natriuretic peptide—adjust kidney function to meet the body's needs (Table 16.3). Antidiuretic hormone (ADH) is manufactured by the hypothalamus and then travels to the posterior pituitary for storage and release. This hormone regulates the amount of water reabsorbed by the collecting ducts. The hypothalamus responds to changes in the concentration of water in the blood by increasing or decreasing secretion of ADH. Decreases in the concentration of water in the blood stimulate increased secretion of ADH, as shown in Figure 16.9. Higher levels of ADH in the bloodstream then increase the permeability to water of the collecting ducts of nephrons, resulting in more water being reabsorbed from the filtrate. The movement of increased amounts of water from the filtrate back into the blood results in increased blood volume and pressure and production of small amounts of concentrated urine.
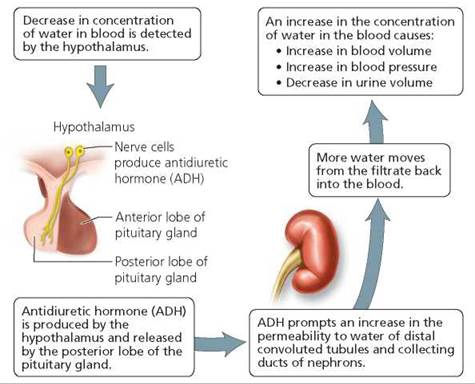
FIGURE 16.9. Regulation of blood volume and blood pressure by ADH
TABLE 16.3. Review of Some Hormones That Influence Kidney Function
|
Hormone |
Effect on Water and Solute Reabsorption in Nephron |
Effect on Blood Volume and Pressure |
Urine Produced |
|
Antidiuretic hormone (ADH) |
Increases permeability to water of collecting ducts, resulting in more water moving from filtrate to blood |
Increases |
Concentrated |
|
Aldosterone |
Increases reabsorption of Na+ by distal convoluted tubules and collecting ducts, resulting in more water following Na+ as it moves from filtrate to blood |
Increases |
Concentrated |
|
Atrial natriuretic peptide (ANP) |
Decreases reabsorption of Na+ by distal convoluted tubules and collecting ducts, resulting in more Na+and water remaining in filtrate |
Decreases |
Dilute |
Just the opposite occurs when the concentration of water in the blood increases. In this case, the release of ADH is inhibited, thereby reducing water reabsorption from the filtrate. Reduced water reabsorption causes reduced blood volume and pressure and the production of large amounts of dilute urine. Alcohol, too, inhibits the secretion of ADH, causing reduced water reabsorption by the kidneys and production of large amounts of dilute urine. Thus, it makes little sense to try to quench your thirst and restore body fluids by drinking an alcoholic beverage on a hot day. Substances such as alcohol that promote urine production are called diuretics. Diabetes insipidus, a disease characterized by excretion of large amounts of dilute urine, is caused by a deficiency of ADH (see Chapter 10).
Aldosterone is released by the adrenal cortex. It increases reabsorption of sodium by the distal convoluted tubules and collecting ducts. Aldosterone accomplishes this task by stimulating the synthesis of sodium ion pumps and sodium channels in cell membranes along the distal convoluted tubules and collecting ducts; at these locations, sodium ions are reabsorbed, usually in exchange for potassium ions. Sodium reabsorption is important because water follows sodium. As more sodium is transported out of the nephron into the capillaries, increased amounts of water go with it, resulting in increased blood volume and pressure and the production of small amounts of concentrated urine.
What stimulates the release of aldosterone? Ultimately, it is the blood pressure in the afferent (incoming) arteriole carrying blood to the glomerulus. The blood pressure in this arteriole is monitored by a part of the nephron called the juxtaglomerular apparatus, a group of cells located where the distal convoluted tubule contacts the afferent arteriole (Figure 16.10). When the blood pressure in the afferent arteriole drops, so does the glomerular filtration rate. In turn, this drop in filtration rate reduces the volume of filtrate within nephrons. Cells within the juxtaglomerular apparatus respond by releasing the enzyme renin. Renin converts angiotensinogen, a protein produced by the liver, into another protein, angiotensin I. Angiotensin I is then converted by yet another enzyme into angiotensin II. Angiotensin II is the active form of the protein that stimulates the adrenal gland to release aldosterone. Aldosterone increases reabsorption of sodium and water by the distal convoluted tubules and collecting ducts of nephrons, resulting in increased blood volume and pressure. These changes increase the filtration rate within the glomerulus, resulting in an increased volume of filtrate within the nephron.
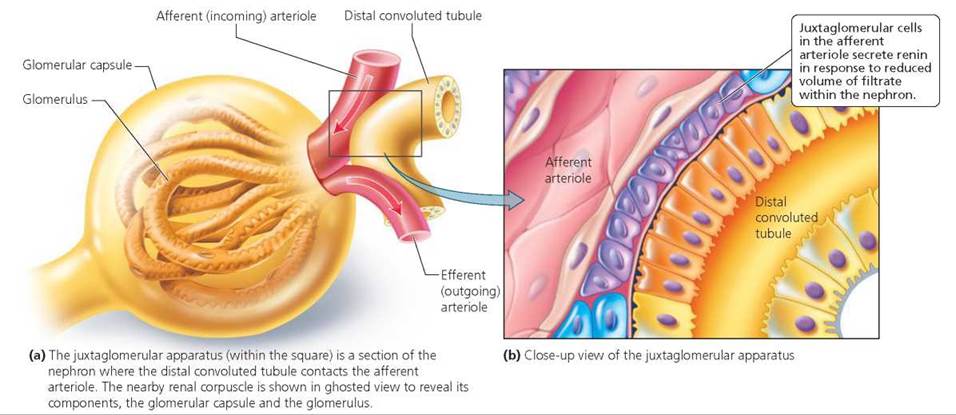
FIGURE 16.10. The juxtaglomerular apparatus
Stop and think
Estrogens are sex hormones that are chemically similar to aldosterone. As a result, the effects of estrogens on the distal convoluted tubules and collecting ducts of the kidneys are similar to those of aldosterone. How might this similarity explain the water retention experienced by many women as their estrogen levels rise during the menstrual cycle?
A final hormone that influences kidney function is atrial natriuretic peptide (ANP), released by cells in the right atrium of the heart. The cells release ANP in response to stretching of the heart caused by increased blood volume and pressure. Atrial natriuretic peptide decreases water and Na+ reabsorption by the kidneys, causing declines in blood volume and pressure and the production of large amounts of dilute urine. ANP also influences kidney function by inhibiting secretion of aldosterone and renin.
Red Blood Cells and Vitamin D
The kidneys have two additional functions that are important to homeostasis but are not directly related to the urinary system. First, the kidneys release erythropoietin, a hormone that travels to the red bone marrow, where it stimulates production of red blood cells. Second, the kidneys have an effect on vitamin D. Vitamin D is a substance provided by certain foods in our diet or produced by the skin in response to sunlight. The kidneys transform vitamin D into its active form, calcitriol, which promotes the absorption and use of calcium and phosphorus by the body.
Dialysis and Transplant Surgery
Renal failure is a decrease or complete cessation of glomerular filtration. In other words, the kidneys stop working. The failure can be acute or chronic. Acute renal failure is an abrupt, complete—or nearly complete—cessation of kidney function. It typically develops over a few hours or days and is characterized by little output of urine. Causes of acute renal failure include nephrons damaged by severe inflammation, certain drugs, and poison. Acute renal failure also may be caused by low blood volume due to profuse bleeding or obstruction of urine flow by kidney stones. Kidney stones are small, hard crystals that form in the kidneys when substances such as calcium or uric acid precipitate out of urine because of higher-than-normal concentrations. Some kidney stones are surgically removed, others are dissolved with drugs, and still others are pulverized with high-energy shock waves, which break the stones into tiny pieces that can be passed painlessly in the urine.
Chronic renal failure is a progressive and often irreversible decline in the rate of glomerular filtration over a period of months or years. Kidney disease may destroy nephrons and cause a progressive decline of this type. Nephrons lost to kidney disease cannot be replaced. Polycystic kidney disease, for example, is an inherited and progressive condition in which fluid-filled cysts and tiny holes form throughout kidney tissue. Few symptoms are apparent at the beginning of chronic renal failure because the remaining nephrons enlarge and take over for those that have been destroyed. With time, however, the loss of nephrons becomes so severe that symptoms of decreased glomerular filtration rate appear. For example, increased levels of nitrogen-containing wastes are found in the blood. By end-stage renal failure, about 90% of the nephrons have been lost, making necessary a kidney transplant or the use of an artificial kidney machine.
Renal failure, whether acute or chronic, has many consequences. These include (1) acidosis, a decrease in blood pH caused by the inability of the kidneys to excrete hydrogen ions; (2) anemia, low numbers of red blood cells caused by the failure of damaged kidneys to release erythropoietin; (3) edema, the buildup of fluid in the tissues because of water and salt retention; (4) hypertension, an increase in blood pressure caused by failure of the renin-angiotensin system and salt and water retention; and (5) accumulation of nitrogen-containing wastes in the blood. In short, failure of the kidneys severely disrupts homeostasis. Untreated kidney failure will lead to death within a few days.
Stop and think
Why would inadequate water consumption increase your chances of developing kidney stones?
Dialysis
A common way of coping with failure or severe impairment of the kidneys is hemodialysis, the use of artificial devices to cleanse the blood of wastes and excess fluid. Often this is done with an artificial kidney machine (Figure 16.11). A tube is inserted into an artery of the patient's arm. Blood flows through the tube and into the kidney machine. The machine pumps the blood into a large canister (called the hemodialyzer), where it is filtered and then returned to the patient's body. Within the hemodialyzer, the blood flows through tubing made of a selectively permeable membrane and immersed in a dialysis solution called the dialysate. The selectively permeable membrane of the tubing permits wastes and excess small molecules to move from the blood into the dialysate. At the same time, the membrane prevents passage into the dialysate of blood cells and most proteins because they are too large. Nutrients are sometimes provided in the dialysate for absorption into the blood. The composition of the dialysate is precisely controlled to maintain proper concentration gradients between the dialysate and the blood. Once the blood has completed the circuit through the tubing, it is returned, free of wastes, to a vein in the arm. Patients requiring hemodialysis typically undergo the procedure about three times a week at a dialysis clinic.
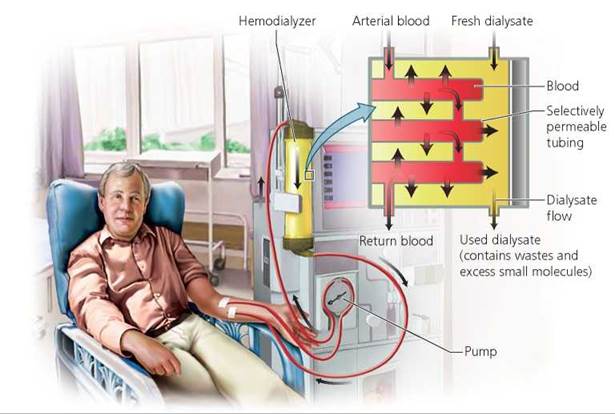
FIGURE 16.11. An artificial kidney machine can be used to cleanse the blood when the kidneys fail.
Another option for removing wastes from the blood is continuous ambulatory peritoneal dialysis (CAPD), a procedure that is normally performed by the patient at home. In this procedure the peritoneum, one of the body's own selectively permeable membranes, is used as the dialyzing membrane. The peritoneum lines the abdominal cavity and covers the internal organs. Dialyzing fluid held in a plastic container suspended over the patient flows down a tube inserted into the abdomen. As the fluid bathes the peritoneum, wastes move from the blood vessels that line the abdomen across the peritoneum and into the solution. The solution is then returned to the plastic container and discarded. Typically, fluid is passed into the abdomen, left for a few hours, and then removed and replaced with new fluid. CAPD requires about three or four fluid changes each day. However, the patient is free to move around between fluid changes while the dialysis proceeds internally, which tends to be less disruptive than traditional hemodialysis.
Because CAPD is performed daily over long periods of time, it is gentler in its waste removal than hemodialysis, resulting in a steadier physical condition in the patient. CAPD is also less costly than hemodialysis. However, CAPD requires that the patient perform several daily changes of dialysis fluid, and each change requires hooking up a new container of dialysate. Thus, CAPD provides more opportunities for bacteria to move down the tube and into the abdomen, where they may cause peritonitis (inflammation of the peritoneum).
In some cases of acute renal failure, dialysis may be needed for a short time, until kidney function returns. Patients with chronic renal failure, however, will need dialysis for the rest of their lives, unless they receive a kidney transplant.
Kidney Transplant Surgery
The ultimate hope for many people whose kidneys fail is to receive a healthy kidney from another person. The kidney was one of the first organs to be successfully transplanted. The availability of dialysis was a crucial part of this success, because dialysis keeps people alive until a suitable donor organ can be found.
What makes a suitable donor organ? The main obstacle to successful acceptance of a transplanted organ is the rejection of foreign tissue by the patient's own immune system (see Chapter 13). The most suitable kidney would come from a patient's identical twin. In fact, the first successful transplant occurred in 1954 between identical twins. A kidney from a close relative, such as a parent or sibling, would be the next best choice. Removal of a healthy kidney is a safe operation, and a healthy donor who gives a kidney away can get along fine with the remaining kidney (of course, all surgeries involve risks, and in the United States about 3 in 10,000 people die from kidney donation). About 90% of kidneys donated by close relatives are still functioning 2 years after transplantation. However, most donated kidneys come from individuals who are unrelated to the patient but who agreed before their death (usually a sudden death in an accident) to donate their organs. About 75% of kidneys donated from unrelated individuals, matched as closely as possible to the patient's tissue and blood type, are still functioning 2 years after transplantation. Even if a transplant fails after a few years, successful second and third transplants may extend a patient's life.
In most situations, the kidneys of the patient needing a transplant are not removed, because survival after surgery is higher when the recipient's own kidneys are left in place. The donor kidney is simply transplanted into a protected area within the pelvis (Figure 16.12). The ureter of the donated kidney is attached to the recipient's bladder, and blood vessels of the donated kidney are attached to the recipient's vessels. The recipient's own kidneys would be removed if they were infected or if they were causing problems such as high blood pressure.
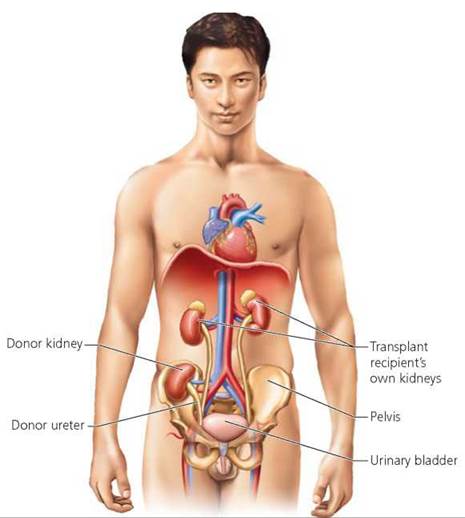
FIGURE 16.12. During a kidney transplant, the donor organ is located in a safe region within the pelvis and its ureter is attached to the recipient’s bladder. Blood vessels from the transplanted kidney are attached to the recipient’s vessels. Typically, the recipient’s own kidneys are left in place.
The high success rate of kidney transplants is linked to the use of drugs that suppress the recipient's immune system. Typically, transplant recipients must take two or more of these medications for the rest of their lives. Recently, a team of researchers developed a way to perform kidney transplants without the recipients' needing to permanently remain on immune-suppressing drugs. The suppressing drugs were given to recipients after transplant surgery. Then, the recipients received several radiation treatments, which were directed at reducing the number of cells in their immune system capable of attacking the new organ. Finally, the recipients received blood stem cells from the person who donated the transplanted kidney. These new stem cells moved to the recipient's bone marrow and generated new blood cells and immune cells. In essence, each recipient now had a hybrid immune system—a mix of his or her own cells and those of the donor. The hybrid immune systems did not recognize the transplanted kidneys as foreign, and recipients were gradually weaned off the immune- suppressing medications.
Despite major advances in kidney transplantation, there still is room for improvement. For example, donor kidneys can be kept alive and healthy for only about 48 to 72 hours (Figure 16.13). This short window of opportunity necessitates rapid location of a recipient, shipment of the donor kidney, and transplantation. Perhaps most important, kidneys available for transplantation are always in short supply. The constant shortage of donor organs has led some people to suggest that we need a new approach to organ donation. The shortage also has led to the illegal sale of kidneys in some countries. See the Ethical Issue essay, Kidney Donation and Trafficking.
FIGURE 16.13. Before transplantation, donor kidneys must be kept in a cool salt solution under sterile conditions. Even under such conditions, kidneys will deteriorate after about 2 or 3 days.
Ethical Issue
Kidney Donation and Trafficking
Kidneys can be transplanted from living or deceased donors, but in many countries there is a long waiting list for organs. Living kidney donors come from several sources. Many are close relatives of the person needing the transplant. Others, known as Good Samaritans, donate a kidney to someone who is not well known to them. In the United States it is illegal to sell organs, so relatives and Good Samaritans are not paid for their kidneys. In Iran, however, some live donors legally receive monetary compensation. In the Iranian system, a person needing a transplant must first seek a willing donor from among family members. If this fails, then he or she must wait up to six months for a kidney from an appropriate deceased donor. Only if this second option fails can the person apply for a kidney from a list of living donors; people on this list are compensated when they donate one of their kidneys. Iran began this legal compensation system in 1988 and its waiting list for kidneys was eliminated by 1999. About 70% of transplants performed in Iran are compensated; the service is not available to foreign nationals. A final way to obtain a kidney from a living donor is to illegally purchase one. Some patients from developed countries buy kidneys from donors in developing countries. When donors are coerced or deceived into giving up one of their kidneys, it is called kidney trafficking (Figure 16.A). The growing illegal trade in kidneys has prompted calls to consider legal compensation of living donors.

FIGURE 16.A. This man sold his kidney on the illegal organ market.
For deceased organ donation, the United States currently employs the opt-in system in which a person must give permission to use his or her organs after death. If a potential donor is incapable of giving such permission, then medical personnel may consult close relatives. In recent years, those in the United States concerned about organ shortages have suggested changing the law so that people would have to provide written proof that they did not want their organs made available for transplantation after death. In other words, without anything in writing, the revised law would presume that people have no objection to organ donation— this is the opt-out system, also known as presumed consent. Countries such as Spain, Austria, Belgium, and Norway use this system and have larger donor pools. Many healthy people probably have no objections to organ donation, but simply do not think about death and the future use of their organs. On the other hand, some people worry that doctors and nurses might let them die because other people need their organs.
The total number of candidates on the waiting list for organs in the United States is updated minute by minute. At 11:38 a.m. on March 8, 2010, that number totaled 106,162. Most of these candidates—83,698—were waiting for kidneys. Many patients wait months or years for a new kidney; in fact, the average wait time in the United States is 1121 days. Perhaps you have considered carrying an organ donor card that says you wish to donate organs or tissues at the time of your death (Figure 16.B). If you haven't already signed an organ donor card, you might want to reconsider it after you have finished reading this essay: Your kidney could save someone else's life—or perhaps someone else's kidney could save you.

FIGURE 16.B. An organ donor card available through www.organdonor.gov. In addition to carrying this card, it is important to let family members know of your decision to donate your organs or tissues. Your intent to donate also can be indicated on your driver’s license.
Questions to Consider
• Do you support legal compensation of living donors?
• Should the United States change from the opt-in to the opt-out system of deceased organ donation?
Urination
Urination is the process by which the urinary bladder is emptied. This process includes both involuntary and voluntary actions and is summarized in Figure 16.14. The kidneys produce urine around the clock. The urine trickles into the ureters and down to the urinary bladder, where it is temporarily stored. When at least 200 ml (0.42 pt) of urine have accumulated, stretch receptors in the wall of the bladder send impulses along sensory neurons to the lower part of the spinal cord. From there, impulses are sent along motor neurons back to the bladder, where they cause a smooth muscle in the wall of the bladder, called the detrusor muscle, to contract. The impulses also cause the internal urethral sphincter, a thickening of smooth muscle located at the junction of the bladder and urethra, to relax. Upon arrival of sensory impulses in the lower spinal cord, information also travels up to the brain and initiates a desire to urinate. If the circumstances are appropriate, the brain permits voluntary relaxation of the external urethral sphincter, a small band of skeletal muscle farther down the urethra. When the external sphincter relaxes, urine exits the body. If the circumstances are not appropriate for urination, the brain does not permit the external sphincter to relax, and the bladder continues to store the urine until a better time. With normal functioning, urine will exit the body later, when the person consciously allows the external sphincter to relax.
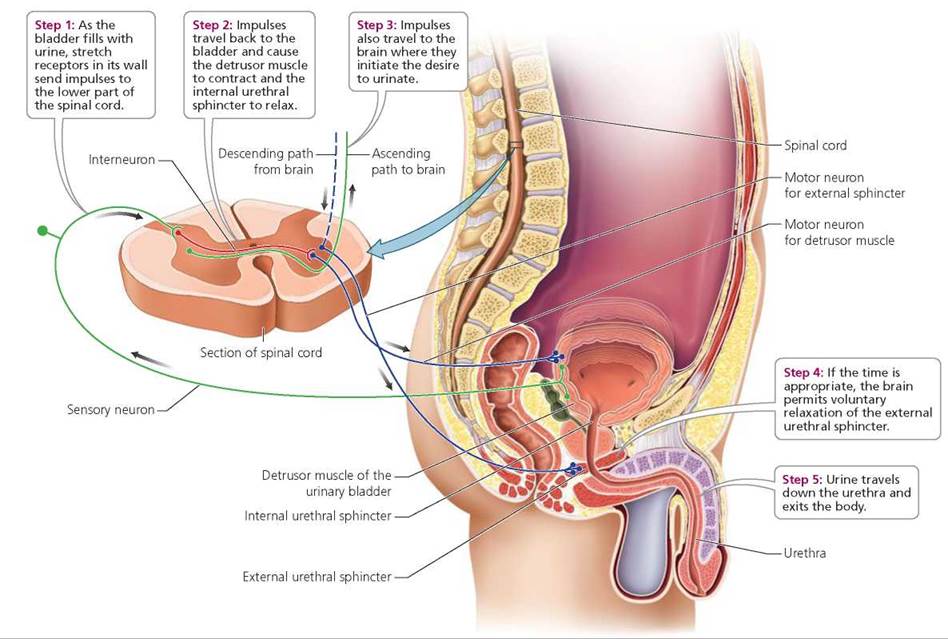
FIGURE 16.14. The steps involved in urination
Thus, although urination is a reflex—a relatively rapid response to a stimulus that is mediated by the nervous system— it can nevertheless be started and stopped voluntarily because of the conscious control exerted by the brain over the external urethral sphincter. However, not everyone can control his or her external urethral sphincter. Lack of voluntary control over urination is called urinary incontinence. Incontinence is the norm for infants and children younger than 2 or 3 years of age, because nervous connections to the external urethral sphincter are incompletely developed. As a result, infants and young children void whenever their bladder fills with enough urine to activate its stretch receptors (Figure 16.15). Toilet training occurs when toddlers learn to bring urination under conscious control. This step is made possible by the development of complete neural connections to the external sphincter.
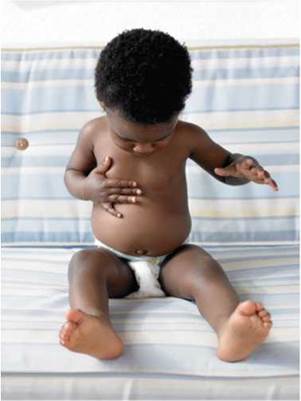
FIGURE 16.15. Conscious control over urination is usually acquired by the age of 3, when neural connections to the external urethral sphincter are fully developed. Before that age, urination occurs as an involuntary reflex.
Damage to the external sphincter may cause incontinence in adults. In men, such damage may occur during surgery on the prostate gland. The prostate gland surrounds the male urethra just below the urinary bladder and contributes substances to semen (see Chapter 17). Incontinence also may occur because of bladder muscles that contract before the bladder is full. This condition is often described as an overactive or spastic bladder. Infection of the urinary system (see the next discussion) can also cause incontinence, in any age group.
Mild incontinence, especially the kind called stress incontinence, is common in adults. Stress incontinence is characterized by the escape of small amounts of urine when sudden increases in abdominal pressure force urine past the external sphincter. Laughing, sneezing, or coughing may cause these sudden increases in pressure.
Urinary retention is the failure to expel urine from the bladder to a normal degree. This condition may result from a lack of the sensation that one must urinate, as might occur temporarily after general anesthesia. It may also result from contraction or obstruction of the urethra. For example, enlargement of the prostate gland in men may obstruct the urethra. Immediate treatment for retention usually involves the use of a tube called a urinary catheter to drain urine from the bladder.
Stop and think
Stress incontinence is more common in women, particularly late in pregnancy and after childbirth. In late pregnancy, the enlarging uterus puts pressure on the bladder. What might explain stress incontinence after childbirth?
Urinary Tract Infections
Presence of microorganisms in the organs of the urinary system can cause a urinary tract infection (UTI). Most bacteria enter the urinary system by moving up the urethra from outside the body. Bacteria called Escherichia coli normally inhabit the colon and can cause UTIs if they enter the urethra. Sometimes, microorganisms called Chlamydia and Mycoplasma cause UTIs. In contrast to E. coli, these bacteria are sexually transmitted (see Chapter 17a). Some bacteria arrive at the kidneys by way of the bloodstream.
The urethras of males and females differ in length, as shown in Figure 16.16. The urethra in females is 3 to 4 cm (1.5 in.) long and lies in front of the vagina. The urethra in males is about 20 cm (8 in.) long and opens to the outside at the tip of the penis. Urinary tract infections are more common in females than in males, perhaps because of their shorter urethras. In females, the bacteria need to travel only a short distance from the external urethral orifice (opening) through the urethra to the bladder. In addition, the external urethral orifice is closer to the anus in females than it is in males. Thus, improper wiping after defecation can easily carry fecal bacteria to the female urethra. (Proper wiping is front to back.) Bacteria also may enter the urethra during sexual intercourse. Women are advised to urinate soon after sex to flush bacteria from the lower urinary tract.
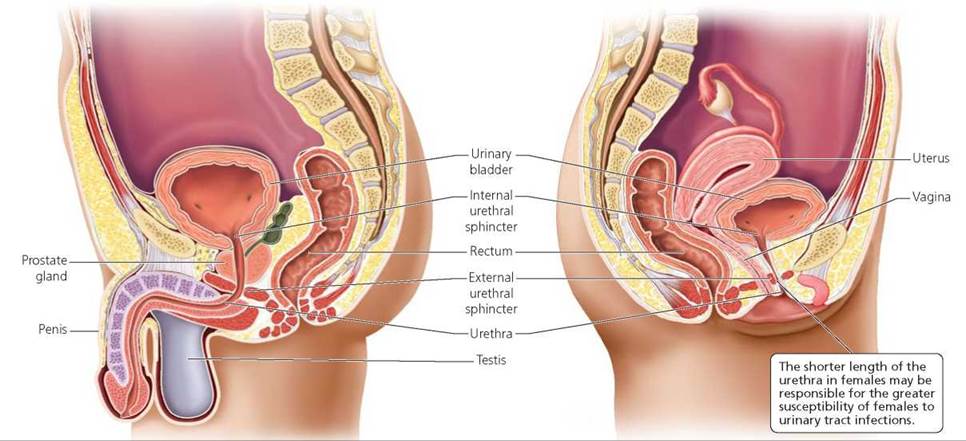
FIGURE 16.16. The urinary bladder and urethra in a male (left) and a female (right)
Symptoms of urinary tract infections include fever, blood in the urine, and painful and frequent urination. Bed wetting may be a symptom in young children. In addition, there may be lower abdominal pain (if the bladder is involved) or back pain (if the kidneys are involved). Physicians usually diagnose such infections by having the urine checked for bacteria and blood cells. People who have recurrent UTIs may wish to purchase nonprescription dipsticks to check for infection. The dipstick is held in the stream of the first morning urine and changes color when it detects nitrite, a compound made by the bacteria. These dipsticks can detect about 90% of UTIs.
Urinary tract infections are treated with antibiotics. Infections of the lower urinary tract (the urethra and bladder) should be treated immediately and the prescribed antibiotics taken for their full term. These steps are critical to prevent the spread of infection to the kidneys, where very serious damage can occur.
Looking ahead
In Chapter 16 we learned that the urethra is a component of the urinary system—it is the tube, in males and females, that transports urine from the urinary bladder to outside the body. In Chapter 17 we discover that the urethra also is considered part of the male reproductive system because it separately transports semen, the fluid containing sperm and secretions from accessory glands.
Highlighting the Concepts
Eliminating Waste (pp. 312-313)
• Several organs from different body systems remove waste from our bodies. Lungs and skin eliminate carbon dioxide, heat, and water. The skin also excretes salt and small amounts of urea and uric acid. Organs of the digestive system eliminate solid wastes (feces), and those of the urinary system excrete nitrogen-containing wastes, water, carbon dioxide, inorganic salts, and hydrogen ions.
Components of the Urinary System (pp. 313-314)
• Two kidneys, two ureters, the urinary bladder, and the urethra make up the urinary system. The main function of this system is to regulate the volume, pressure, and composition of the blood. The kidneys filter excess materials and wastes from the blood and produce urine. Urine travels down the ureters to the urinary bladder, where it is stored until excreted from the body through the urethra. The male urethra transports reproductive fluid in addition to urine (but not at the same time). The female urethra transports only urine.
Kidneys and Homeostasis (pp. 314-323)
• The kidneys are located just above the waist against the back wall of the abdominal cavity. Each kidney has an outer portion (the renal cortex), an inner region (the renal medulla), and an inner chamber (the renal pelvis).
• Properly functioning kidneys are critical to maintaining homeostasis. These organs filter wastes and excess materials from the blood, help regulate blood pH, and maintain fluid balance by regulating the volume and composition of blood and urine.
• Nephrons are tiny tubules responsible for the formation of urine. There are two basic parts to a nephron: (1) the renal corpuscle, which consists of a tuft of capillaries called the glomerulus and a surrounding cuplike structure called the glomerular capsule; and (2) the renal tubule. The renal tubule has three sections: the proximal convoluted tubule, the loop of the nephron, and the distal convoluted tubule. The distal convoluted tubules of several nephrons empty into a single collecting duct. Urine in collecting ducts moves into a large chamber within the kidneys called the renal pelvis. From the renal pelvis, urine leaves the kidneys by traveling down the ureters to the urinary bladder.
• Glomerular filtration is the process by which only certain substances are allowed to pass out of the blood and into the nephron. High pressure within glomerular capillaries forces water and small solutes in the blood across a filter into the space within the glomerular capsule. Large proteins and blood cells normally cannot cross the filter.
• From the glomerular capsule, the filtrate—consisting of water, ions, and small molecules filtered from the blood—moves into the renal tubule of the nephron. As it passes through the renal tubule, about 99% of it is returned to the blood in a process known as tubular reabsorption. Almost all the water, ions, and nutrients in the filtrate are returned to the blood. Wastes are either partially reabsorbed or not reabsorbed at all. Most reabsorption occurs in the proximal convoluted tubule.
• During tubular secretion, drugs and any wastes or excess essential ions that may have escaped glomerular filtration are removed from the blood in the capillaries surrounding nephrons and added to the filtered fluid that will become urine. This process occurs primarily along the proximal and distal convoluted tubules and collecting ducts.
• The kidneys work with the lungs and buffer systems to regulate pH. Specifically, tubular reabsorption returns bicarbonate to the blood (for use in buffering), and tubular secretion removes excess hydrogen ions from the blood.
• Most nephrons have short loops that are restricted almost entirely to the renal cortex. About 20% of the nephrons have long loops that extend deep into the renal medulla. These nephrons are responsible for the extreme water-conserving ability of the kidneys because they maintain high solute concentrations in the interstitial fluid within the kidneys. Maintenance of this gradient between the interstitial fluid and the filtrate enables large amounts of water to move out of collecting ducts by osmosis for conservation by the body, and leads to the production of concentrated urine.
• Several hormones influence kidney function. Antidiuretic hormone (ADH) is produced by the hypothalamus and released by the posterior lobe of the pituitary gland. ADH increases water reabsorption in the collecting ducts of nephrons. Aldosterone is secreted by the adrenal cortex. Aldosterone increases sodium reabsorption by the distal convoluted tubules and collecting ducts. Because water follows sodium, aldosterone increases water reabsorption by nephrons. Atrial natriuretic peptide (ANP) is a hormone released by cells of the right atrium of the heart. ANP causes decreased water and sodium reabsorption by the kidneys, which causes a decrease in blood pressure and volume.
• The kidneys release the hormone erythropoietin, which is necessary for red blood cell production. The kidneys also convert vitamin D into its active form that promotes the body's absorption of calcium and phosphorus.
Dialysis and Transplant Surgery (pp. 323-326)
• Renal failure is a decrease or complete cessation of glomerular filtration. Failure of the kidneys severely disrupts homeostasis. Conditions such as acidosis, anemia, edema, hypertension, and a toxic buildup of nitrogen-containing wastes in the blood may result when the kidneys stop working.
• Treatments for renal failure include hemodialysis (using artificial devices to cleanse the blood), continuous ambulatory peritoneal dialysis (using the patient's own peritoneum as the dialyzing membrane), and kidney transplantation.
Urination (pp. 326-328)
• Urination, the process by which the urinary bladder is emptied, entails both involuntary and voluntary actions. Moderate filling of the bladder stimulates stretch receptors in its wall that send impulses along sensory neurons to the lower spinal cord. From the spinal cord, impulses move along motor neurons back to the bladder, where they cause the muscular wall of the bladder to contract. The impulses also cause the internal urethral sphincter, a thickening of smooth muscle at the junction of the bladder and urethra, to relax. These actions push stored urine into the urethra. If conditions are appropriate, the brain then permits voluntary relaxation of the external urethral sphincter, a band of skeletal muscle farther down the urethra, causing urine to exit the body.
Urinary Tract Infections (pp. 328-329)
• Urinary tract infections (UTIs) are more common in females than in males, possibly because bacteria can more readily move from outside the body up the shorter urethra of females to the bladder. Infections may occur in the urethra, bladder, and kidneys, with infections of the kidneys being the most serious.
Reviewing the Concepts
1. Name four nitrogen-containing wastes produced by humans. Describe the processes that generate them, and name the organs primarily responsible for excreting them. pp. 312-313
2. List the components of the urinary system and their functions. pp. 313-314
3. Describe the ways in which kidneys maintain homeostasis. pp. 314-323
4. Explain glomerular filtration, tubular reabsorption, and tubular secretion by nephrons. Where in the nephron does each process occur? pp. 316-318
5. How do nephrons contribute to the regulation of blood pH? p. 318
6. How do the kidneys conserve water, and why is this important? pp. 318-320
7. Identify three hormones that play a significant role in kidney function, and explain how each hormone works to help the kidneys meet the body's needs on a daily basis. pp. 321-323
8. Does the solute concentration in interstitial fluid increase, decrease, or stay the same from the renal cortex to the renal medulla? Please explain. pp. 318-321
9. Describe the process and mechanisms involved in urination. pp. 326-327
10. How do the urethras of males and females differ? What are the clinical implications of these differences? pp. 328-329
11. Glomerular filtration
a. occurs at the renal corpuscle.
b. returns useful substances to the blood.
c. occurs along the renal tubule.
d. is the last step of three in cleansing the blood.
12. Which of the following substances would normally not pass through the glomerular filter?
a. Water
b. Ions
c. Red blood cells
d. Glucose
13. In the nephron, microvilli characterize the
a. proximal convoluted tubule.
b. collecting duct.
c. distal convoluted tubule.
d. glomerulus.
14. Which of the following would raise blood pH?
a. Reabsorption of H+
b. Secretion of HCO3-
c. Secretion of H+
d. Reabsorption of glucose
15. Tubular reabsorption
a. allows only certain substances to pass from the blood into the nephron.
b. returns useful substances from the filtrate to the blood.
c. removes wastes and excess essential ions that escaped filtration from the blood.
d. occurs at the renal corpuscle.
16. _____ is the region of the nephron that monitors the pressure of blood entering the glomerulus, and it ultimately influences the release of aldosterone.
17. _____ is the use of artificial devices to cleanse the blood.
18. The _____ urethral sphincter is made of _____ muscle and is involuntary. The _____ urethral sphincter is made of _____ muscle and allows voluntary control over urination.
Applying the Concepts
1. Rachel has noticed that since she gave birth, a small amount of urine escapes whenever she sneezes. What condition might Rachel have? What would explain this condition?
2. Miguel has noticed that after he drinks beer, his urine output increases. Why does this happen?
3. Li has polycystic disease, an inherited and progressive condition that is destroying her kidneys. What will be the health consequences of her chronic renal failure? What are her options for restoring kidney function? What are the advantages and disadvantages of each option?
4. Varian has proteinuria, a condition in which an abnormal amount of protein is present in his urine. His physician suspects that hypertension caused the proteinuria. Which region of the nephron did hypertension likely damage to produce proteinuria? How might proteinuria be diagnosed?
Becoming Information Literate
Write a paper on some of the major changes that occur in the urinary system across the life span. Include in your paper the general changes to kidney function caused by age-related declines in number of nephrons, rates of glomerular filtration, and sensitivity of nephrons to ADH. Keep a log of the sources (books, journal articles, websites) that you look at during your search for information. Next to each source, indicate whether you found it helpful and accurate.