THE LIVING WORLD
Unit Six. Animal Life
31. Reproduction and Development
The Fourth Week: Organogenesis
In the fourth week of pregnancy, the body organs begin to form, a process called organogenesis (figure 31.20a; the drawing helps identify the structures in the photo). The eyes form, and the heart begins a rhythmic beating and develops four chambers. At 70 beats per minute, the little heart is destined to beat more than 2.5 billion times during a lifetime of about 70 years. More than 30 pairs of somites are visible by the end of the fourth week, and the arm and leg buds have begun to form. The embryo more than doubles in length during this week, reaching about 5 millimeters.
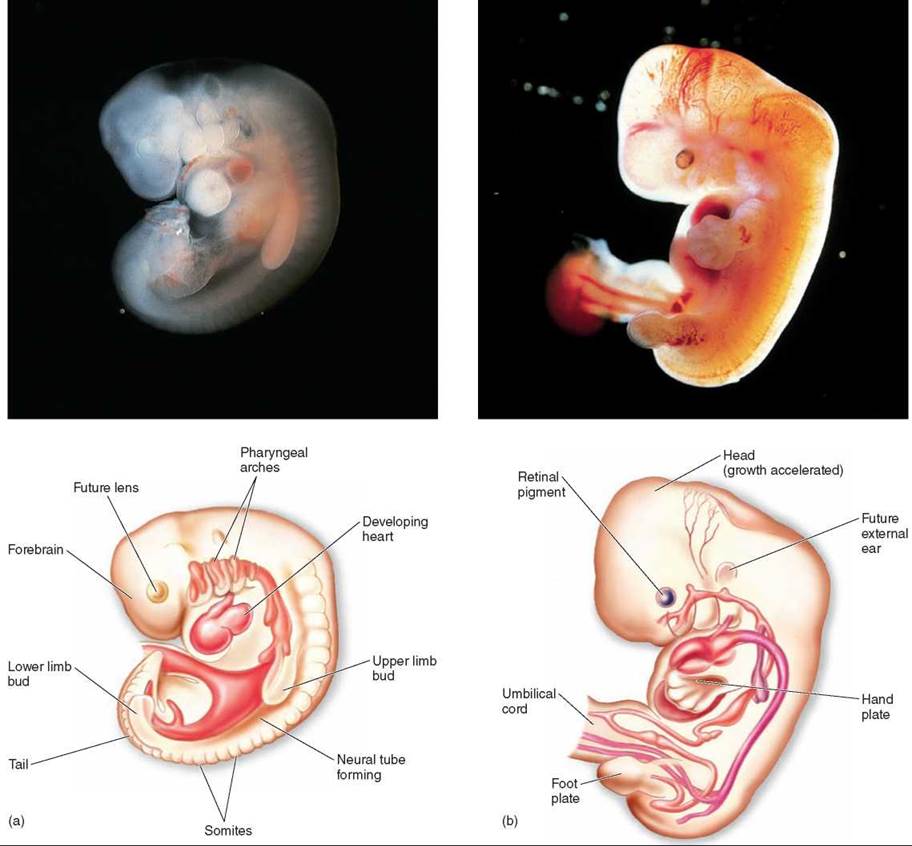
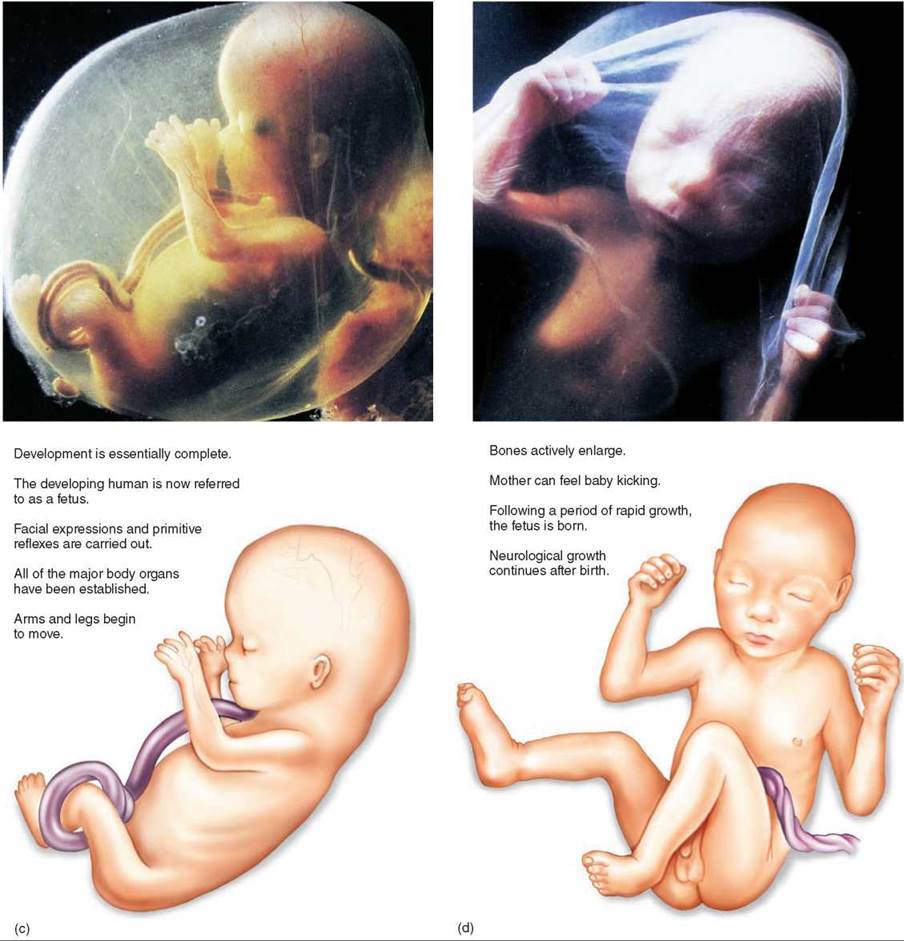
Figure 31.20. The developing human.
(a) Four weeks; (b) seven weeks; (c) three months; and (d) four months.
By the end of the fourth week, the developmental scenario is far advanced, although most women are not yet aware that they are pregnant. This is a crucial time in development because the proper course of events can be interrupted easily. For example, alcohol use by pregnant women during the first months of pregnancy is one of the leading causes of birth defects, producing fetal alcohol syndrome, in which the baby is born with a deformed face and often severe mental retardation. One in 250 newborns in the United States is affected by fetal alcohol syndrome. Also, most spontaneous abortions (miscarriages) occur during this period.
The Second Month: The Embryo Takes Shape
During the second month of pregnancy, great changes in morphology occur as the embryo takes shape (figure 31.20b). The miniature limbs of the embryo assume their adult shapes. The arms, legs, knees, elbows, fingers, and toes can all be seen as well as a short, bony tail. The bones of the embryonic tail, an evolutionary reminder of our past, later fuse to form the coccyx, or tailbone. Within the body cavity, the major internal organs are evident, including the liver and pancreas. By the end of the second month, the embryo has grown to about 25 millimeters in length—it is 1 inch long. It weighs perhaps a gram and is beginning to look distinctly human.
The Third Month: Completion of Development
Development of the embryo is essentially complete except for the lungs and brain. The lungs don’t complete development until the third trimester, and the brain continues to develop even after birth. From this point on, the developing human is referred to as a fetus rather than an embryo. What remains is essentially growth. The nervous system and sense organs develop during the third month. The fetus begins to show facial expressions and carries out primitive reflexes such as the startle reflex and sucking. By the end of the third month, all of the major organs of the body have been established and the arms and legs begin to move (figure 31.20c).
The Second Trimester: The Fetus Grows in Earnest
The second trimester is a time of growth. In the fourth (figure 31.20d) and fifth months of pregnancy, the fetus grows to about 175 millimeters in length (almost 7 in long), with a body weight of about 225 grams. Bone formation occurs actively during the fourth month. During the fifth month, the head and body become covered with fine hair. This downy body hair, called lanugo, is another evolutionary relic and is lost later in development. By the end of the fourth month, the mother can feel the baby kicking; by the end of the fifth month, she can hear its rapid heartbeat with a stethoscope.
In the sixth month, growth accelerates. By the end of the sixth month, the baby is over 0.3 meters (1 ft) long and weighs 0.6 kilograms (about 1.5 lb)—and most of its prebirth growth is still to come. At this stage, the fetus cannot yet survive outside the uterus without special medical intervention.
The Third Trimester: The Pace of Growth Accelerates
The third trimester is a period of rapid growth. In the seventh, eighth, and ninth months of pregnancy, the weight of the fetus more than doubles. This increase in bulk is not the only kind of growth that occurs. Most of the major nerve tracts are formed within the brain during this period, as are new brain cells.
All of this growth is fueled by nutrients provided by the mother’s bloodstream, passing into the fetal blood supply within the placenta. The placenta in figure 31.21 contains blood vessels that extend from the umbilical cord into tissues that line the uterus (the decidua basalis in the figure). The mother’s blood bathes this tissue so that nutrients can pass from the mother’s blood into the blood vessels that carry it back to the fetus without the two blood systems ever mixing blood. The undernourishment of the fetus by a malnourished mother can adversely affect this growth and result in severe retardation of the infant. Retardation resulting from fetal malnourishment is a severe problem in many underdeveloped countries, where poverty and hunger are common.
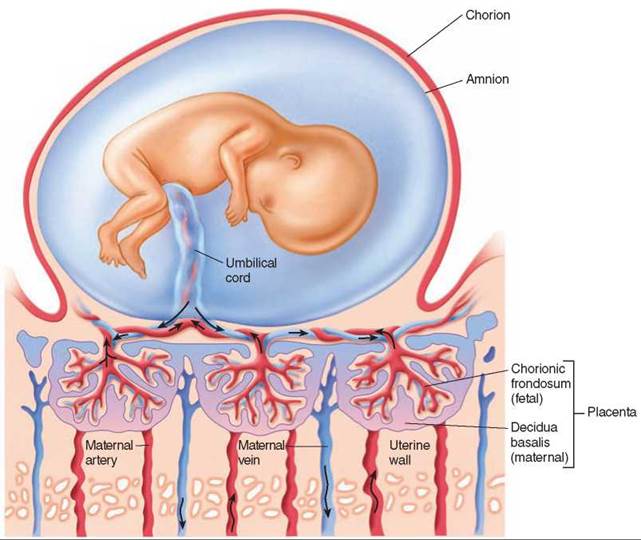
Figure 31.21. Structure of the placenta.
The placenta contains a fetal component, the chorionic frondosum, and a maternal component, the decidua basalis. Oxygen and nutrients enter the fetal blood from the maternal blood by diffusion. Waste substances enter the maternal blood from the fetal blood, also by diffusion.
By the end of the third trimester, the neurological growth of the fetus is far from complete and, in fact, continues long after birth. But by this time the fetus is able to exist on its own. Why doesn’t the fetus continue to develop within the uterus until its neurological development is complete? What’s the rush to get out and be born? Because physical growth is continuing as well, and the fetus is about as large as it can get and still be delivered through the pelvis without damage to mother or child. As any woman who has had a baby can testify, it is a tight fit. Birth takes place as soon as the probability of survival is high.
Birth
At approximately 40 weeks from the last menstrual cycle, the process of birth begins. Hormonal changes in the mother, in addition to physical and possibly hormonal signals from the fetus, initiate the onset of labor. During labor (and delivery), the cervix gradually dilates (the opening becomes larger), the amnion ruptures causing amniotic fluid to flow out through the vagina (sometimes referred to as the “water breaking”), and uterine contractions become strong and regular, usually resulting in the expulsion of the fetus from the uterus. Hormones called oxytocin and prostaglandins work in a positive feedback mechanism to stimulate and increase uterine contractions. The fetus is usually in a head-down position near the end of pregnancy. In a vaginal birth, the fetus is pushed down through the cervix and out through the vagina (figure 31.22). The umbilical cord is still attached to the baby, and a doctor, nurse, or parent clamps and cuts the cord. The baby transitions from living in a fluid environment to a gaseous one, and many of its organ systems undergo major changes. After the birth of the fetus, continuing uterine contractions expel the placenta and associated membranes, collectively called the “afterbirth.” In some cases, such as when a vaginal delivery would cause harm to the fetus or the mother, the fetus and placenta are surgically removed from the uterus in a procedure called a caesarian section (C-section).
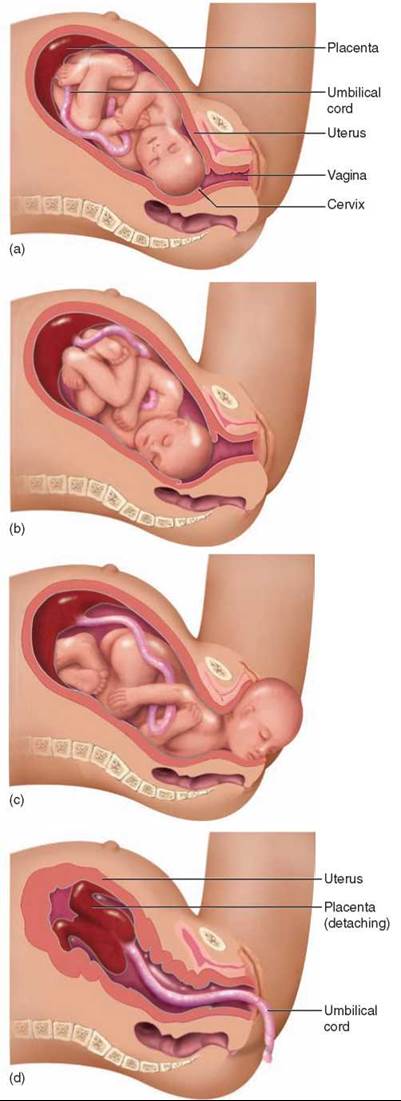
Figure 31.22 Stages of childbirth.
In the mother, hormones during late pregnancy prepare the mammary glands (see section 20.8) for nourishing the baby after birth. For the first couple of days after childbirth, the mammary glands produce a fluid called colostrum, which contains protein and lactose but little fat. Then milk production is stimulated by the anterior pituitary hormone prolactin, usually by the third day after delivery. When the infant suckles at the breast, the posterior pituitary hormone oxytocin is released, initiating milk release, or milk “letdown.”
Postnatal Development
Growth continues rapidly after birth. Babies typically double their birth weight within a few months. Different organs grow at different rates, however, and the body proportions of infants are different than those of adults. The head, for example, is disproportionately large in newborns, but after birth it grows more slowly than the rest of the body. Such a pattern of growth, in which different components grow at different rates, is referred to as allometric growth.
At birth, the developing nervous system of humans is generating new nerve cells at an average rate of more than 250,000 per minute. Then, about six months after birth, this production of new neurons essentially ceases (recent research has shown new neurons continue to be produced into adulthood in a few small regions of the brain). The fact that the human brain continues to grow significantly for the first few years of postnatal life means that adequate nutrition and a safe environment are particularly crucial during this period.
Key Learning Outcome 31.7. Most of the key events in fetal development occur early. Organs begin to form in the fourth week, and by the end of the second month the developing body looks distinctly human. The development of the embryo is essentially complete before the woman may even know she is pregnant. What remains in the second and third trimester is primarily growth.
Biology and Staying Healthy
Why Don't Men Get Breast Cancer?
In 2007, an estimated 240,510 new cases of breast cancer were expected among women in the United States and 2,030 new cases among men—over 99% of the new breast cancer victims were women. Similarly, of 40,460 breast cancer deaths anticipated that year, all but 450 of them were women. It is impossible not to wonder why so few men? An obvious answer would be that men don't have breasts, but men do have breast tissue, it just isn't as developed as a woman's. So why so few men?
While 5% of breast cancers are due to inherited genetic mutations (BRCA1 and BRCA2), the cause of 95%—the overwhelming majority—remains a mystery. Hormone differences seem the most promising place to start, as the female sex hormone estrogen controls breast development in women; men, by contrast, lack physiologically significant amounts of estrogen. A logical suggestion is that in breast cancer patients, the effect of estrogen on breast cells is being altered by exposure to a so-called endocrine disrupter. Endocrine disrupters are man-made chemicals that mimic hormones. By sheer chance, their molecules are perfectly shaped to fit particular hormone receptors. In this case, the culprit would be a chemical mimic of estrogen that promotes cancerous growth in breast cells.
One candidate is bisphenol A (BPA), a molecule that is structurally similar to estrogen, with carbon rings at each end tipped with OH groups. Used to form the plastic packaging of many foods and drinks, as well as the clear plastic liners of metal food and beverage cans, BPA is a chemical to which all of us are exposed daily. Six billion pounds are produced worldwide each year.
It has been known since 1938 that BPA promotes excess estrogen production in rats. Alarmingly, in 1993 BPA was shown to have the same effects on human breast cancer cells growing in culture. What was alarming was that the effect could be measured at concentrations as low as 2 parts per billion, not much above the levels to which we humans are routinely exposed.
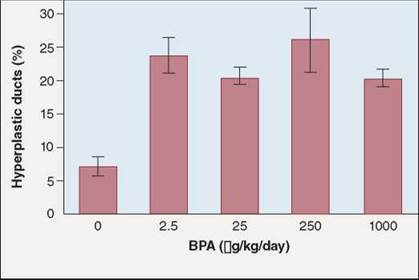
Does BPA in fact induce breast cancer? To test this possibility, Dr. Ana Soto of Tufts University School of Medicine and her research team in 2006 tested its effects on rats, which get breast cancer in much the same way as humans do. They exposed pregnant female rats to a range of BPA concentrations, and after 50 days sacrificed them for examination of their breast tissue. The researchers looked in particular for aberrant cell growth patterns in breast tissue called ductal hyperplasias, which in both rats and people are considered to be the precursors of breast cancer. BPA was administered to four groups of rats. Some received low doses not unlike what humans are exposed to, while others received much higher doses. In a fifth group, which served as a control, no BPA was administered.
The histogram above shows what the researchers found. Amounts of BPA administered to the rats are reported in micrograms of BPA per kilogram of body weight per day. The incidence of breast cancer detected is presented as the percent of examined breast tissue ducts which were hyperplastic (that is, precancerous). Vertical black lines (called error bars) represent 5% confidence intervals (a measure of scatter among the data—95% of replicate experiments would be expected to fall within the ranges of the error bars).
What are we to make of the data the researchers obtained? Did any of the four doses of BPA they administered result in a percent of hyperplastic ducts significantly higher than that seen in the BPA control group? (Hint: If their error bars overlap with the control's, the difference is not significant.) The answer—yes, all four doses are significant. Do higher doses of BPA increase the incidence of hyperplastic ducts? Do the error bars of the four doses fail to overlap? No, all doses yielded similar results. It is difficult to avoid the conclusion that exposure to even low levels of bisphenol A induces ductal hyperplasias in laboratory rats.
These results suggest the rather alarming conclusion that BPA, a chemical to which we are all exposed every day, may cause breast cancer. The study is small, and a rat is not a human, but the possibility that BPA is a carcinogen certainly merits further investigation. Most government-funded breast cancer research has focused on the search for more effective breast cancer treatments; far less money is spent on searching for the causes of breast cancer. The most encouraging aspect of this study is its suggestion that such a search, if it became a priority, might prove fruitful.