Classic Human Anatomy in Motion: The Artist's Guide to the Dynamics of Figure Drawing (2015)
Chapter 2
Joints and Joint Movement
To fully understand movement, artists need to become familiar with the mechanics of the joints. While muscles are important because they are responsible for moving the bones, the joints play a vital role in the movement of the human figure—its limitations as well as its capabilities. This chapter focuses on the various joints and their movements.
Basic Joint Types
The are three basic types of joints—fibrous, cartilaginous, and synovial. Of these, the synovial joints are of the greatest interest to artists, but let’s take a brief look at the other two types before turning our attention to the several different categories of synovial joints.
Fibrous Joints
Fibrous joints are held together with fibrous connective tissue. There are three different types of fibrous joints, shown in the drawing at right: suture joints, gomphosis joints, and syndesmosis joints. Suture joints are fused, immovable joints with a zigzag appearance; examples are the suture joints of the cranium. Gomphosis joints (pron., gom-FOH-sis) are immovable joints in which a peglike structure fits into a socket; examples are the gomphosis joints of the teeth, each of which is individually rooted in a tooth socket. Syndesmosis joints (pron., SIN-dez-MOH-sis) are capable of slight movement because the fibrous connective tissue (interosseous membrane) that binds the bones together is slightly longer than that of the other two fibrous joints. Syndesmosis joints are found between the ulna and radius bones of the lower arm and the tibia and fibula bones of the lower leg.
FIBROUS JOINTS—THREE TYPES
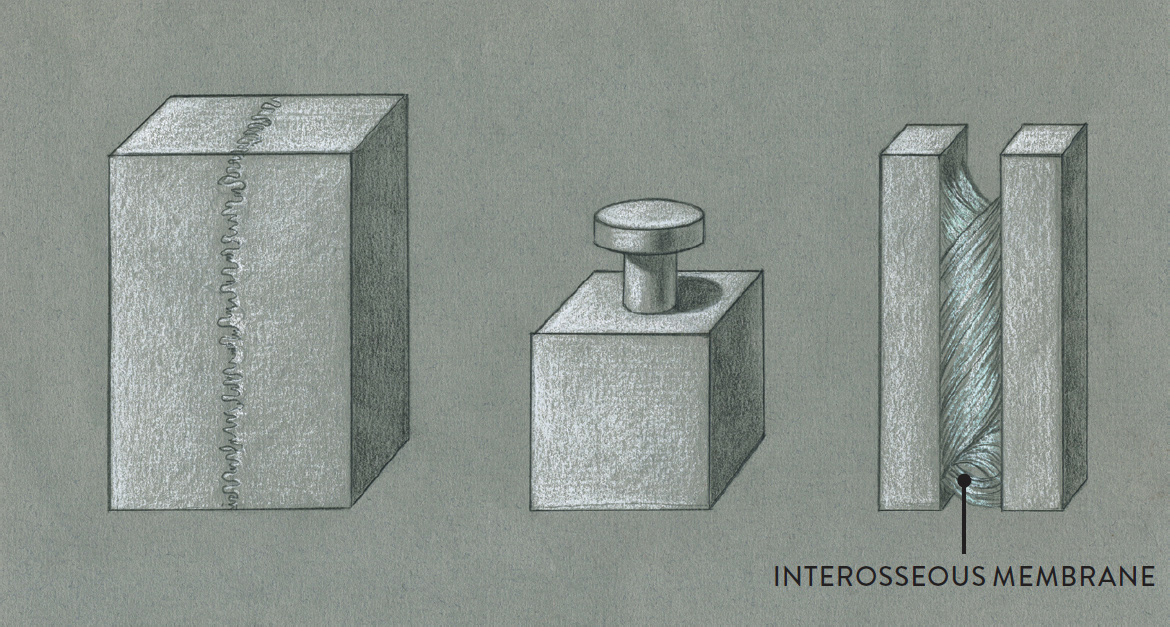
LEFT: Suture joint
CENTER: Gomphosis joint
RIGHT: Syndesmosis joint
Cartilaginous Joints
Cartilaginous joints (pron., KAR-tih-LAAJ-ih-nuss) are connected together with a cartilage-like connective tissue, usually in the form of a fibrocartilaginous disc. There are two different types of cartilaginous joints: synchondrosis joints and symphysis joints. Synchondrosis joints (pron., sin-kon-DROH-sis) are immovable; an example is the joint between the first costal cartilage of a rib and the sternum. Symphysis joints (pron., SIM-fih-sis) are slightly movable and are located on the midline (medial line) of the body. Examples are the joints between the vertebrae (intervertebral disc joints), which have small fibrocartilage pads called intervertebral discs, and the joint between the pubic bones, called the pubic symphysis.
CARTILAGINOUS JOINTS—TWO TYPES
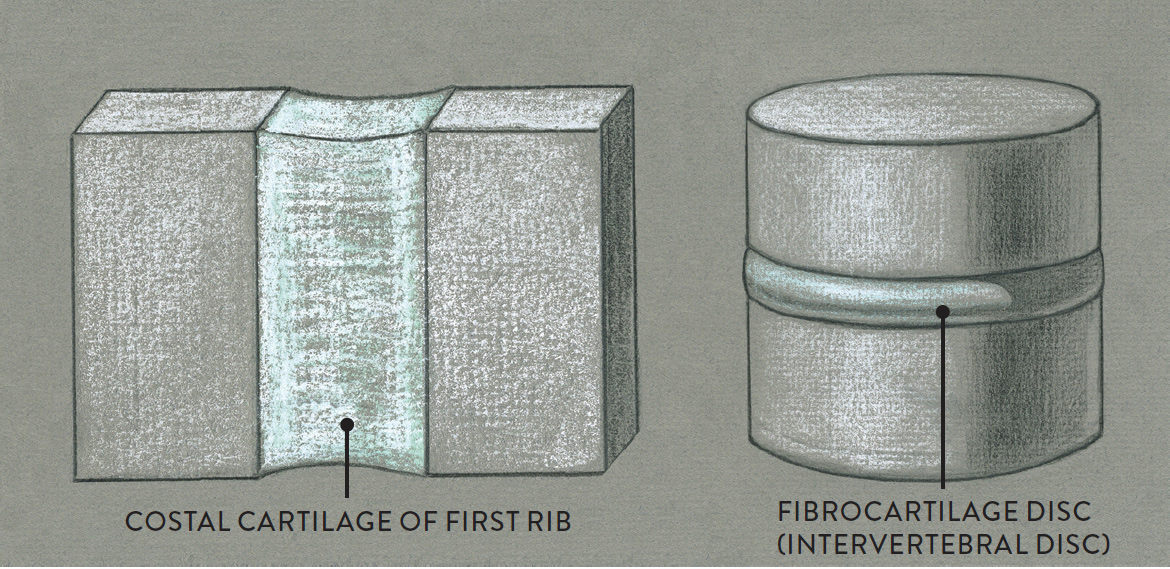
LEFT: Synchondrosis joint
RIGHT: Symphysis joint
Synovial Joints
Also called movable joints, synovial joints (pron., sih-NO-vee-al) are essential for artists to know because of the tremendous variety of movement possibilities they enable. The outer ends of the bones that articulate with each other in synovial joints have a protective coating of articular cartilage to reduce friction and minimize wear and tear during movement. These joints are also encapsulated in an outer layer of fibrous tissue (mainly ligaments) and an inner layer called the synovial membrane. The synovial membrane contains synovial fluid, which functions as a lubricant for the joint. This entire structure is called the joint capsule. Joint capsules are found only at the synovial joints.
Each of the various types of synovial joints—ball-and-socket, hinge, pivot, saddle, gliding/plane, and ellipsoid/condyloid—produces a distinctive kind of movement, as can be seen in the drawings here.
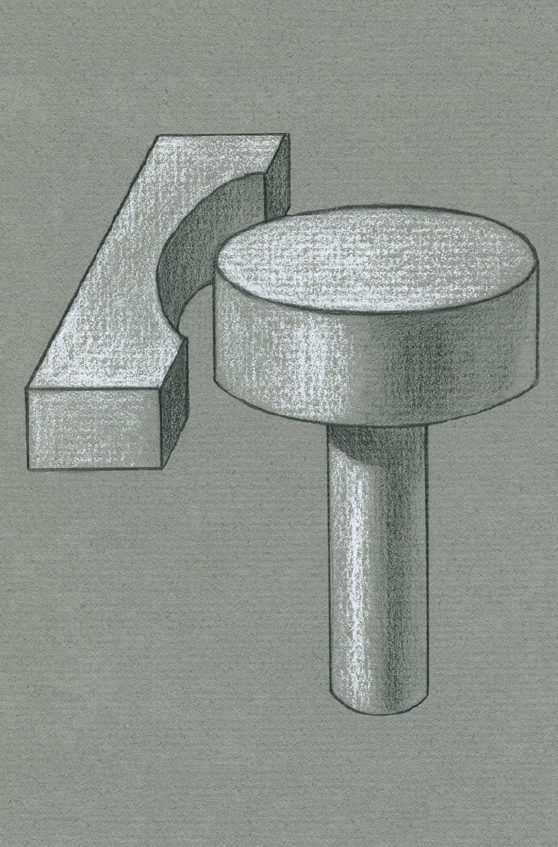
BALL-AND-SOCKET JOINT
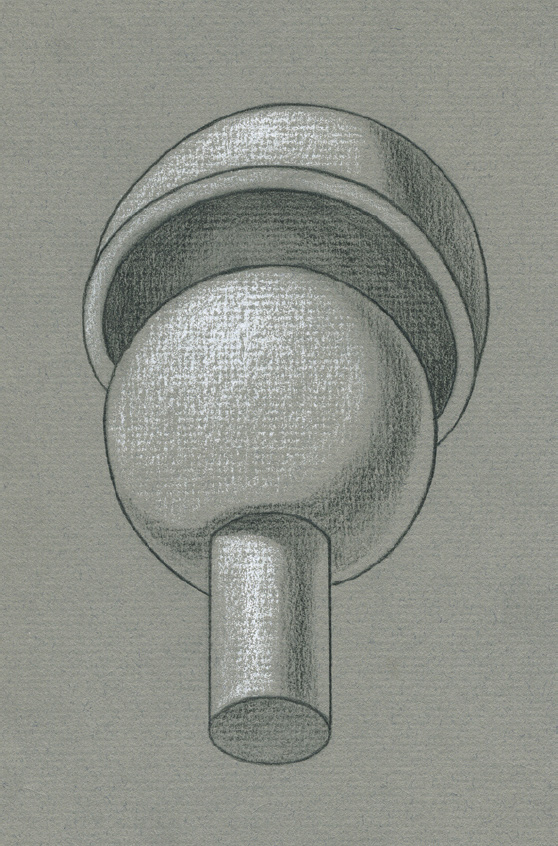
In a ball-and-socket joint, a ball-shaped head on one bone fits into a cuplike socket on another bone.
A ball-and-socket joint is just what the term says: a spherelike structure fitting into a cuplike structure. Examples include the shoulder joint (glenohumeral joint) and hip joint (femoroacetabular joint). Of all the types of synovial joints, ball-and-socket joints have the greatest ability to move bones in many different directions.
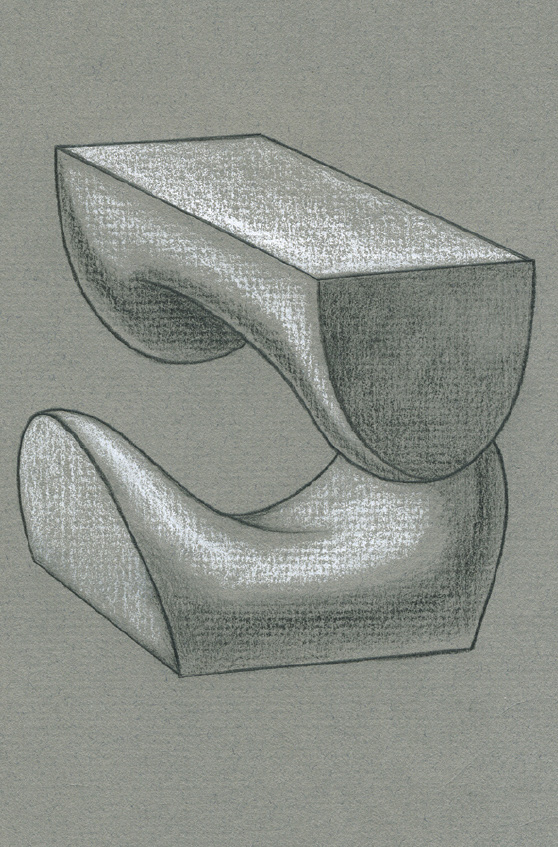
HINGE JOINT
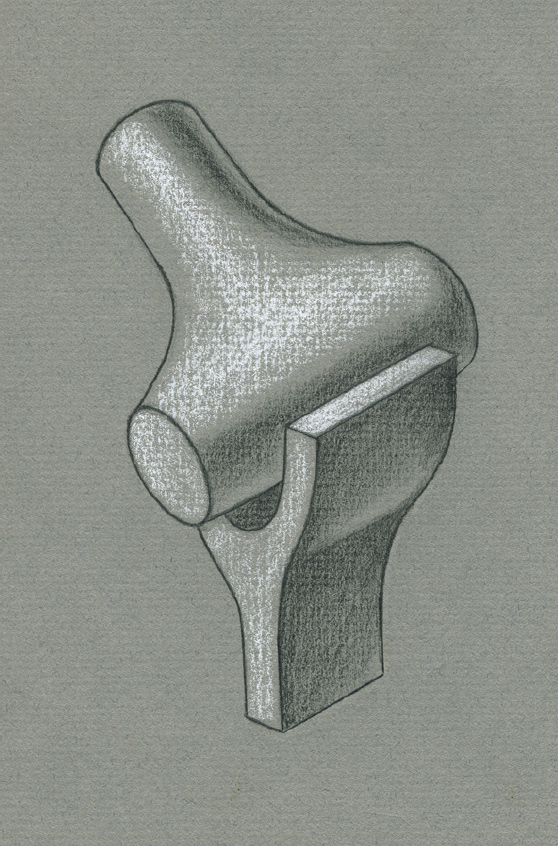
In a hinge joint, a convex surface on one bone fits into a concave surface on another bone.
A hinge joint produces more limited movement, in that it can only move a bone in one direction and then return the bone back to its original position, much like the opening and closing of a door (hence the name). Hinge joints include the lower-jaw joint (temporomandibular joint, or TMJ), elbow joint (humeroulnar joint), knee joint (tibiofemoral joint), ankle joint (talocrural joint), and the finger and toe joints (interphalangeal joints). Some anatomists consider the TMJ and knee joint to be modified hinge joints rather than true hinge joints because subtle subsidiary movements, such as rolling and gliding of the bones, occur within these joints.
PIVOT JOINT
In a pivot joint, the rounded end of one bone rotates within a ringlike structure formed by another bone or a ligament.
A pivot joint has the ability to swivel a bone on its own axis—as when you shake your head “no” or turn your hand from an upward to a downward position. Joints of this type are found at the upper neck (alanto-axial joint), elbow (proximal radioulnar joint), and wrist (distal radioulnar joint).
SADDLE JOINT
In a saddle joint, the two articulating ends of bones are shaped somewhat like saddles, with convex and concave surfaces, and are positioned perpendicularly, one overtop the other.
A saddle joint has slightly more movement than a hinge joint because of its saddlelike concave and convex articulating surfaces. The best-known saddle joint is the carpometacarpal joint at the base of the thumb, which helps move the thumb forward and back as well as across the palm, back to its normal position, and then out to the side. Some anatomists also consider the sternoclavicular (SC) joint between the inner end of the clavicle and the manubrium of the sternum to be a saddle joint.
GLIDING/PLANE JOINT
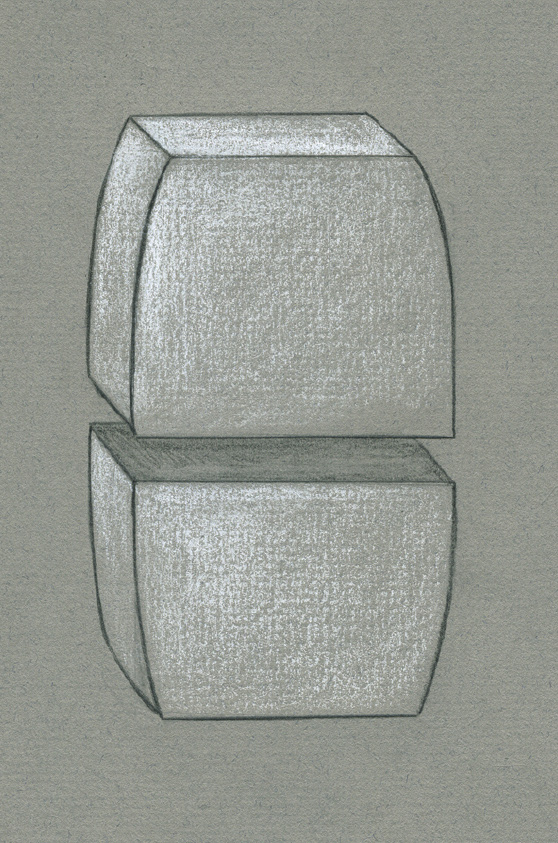
In a gliding joint, two bones with flat or slightly curved surfaces glide across each other.
A gliding joint, or plane joint, has the least movement capability of all the synovial joints. As the name implies, the bones simply glide against each other. Gliding joints include the carpal joints (intercarpal joints), the tarsal joints (intertarsal joints), the carpal and metacarpal joints (CMC joints), and the pelvis joint (sacroiliac joint); they also occur between the ribs and vertebral column (costovertebral joints), the sternum and ribs (sternocostal joints), and the acromion process and clavicle (acromioclavicular joint).
ELLIPSOID/CONDYLOID JOINT
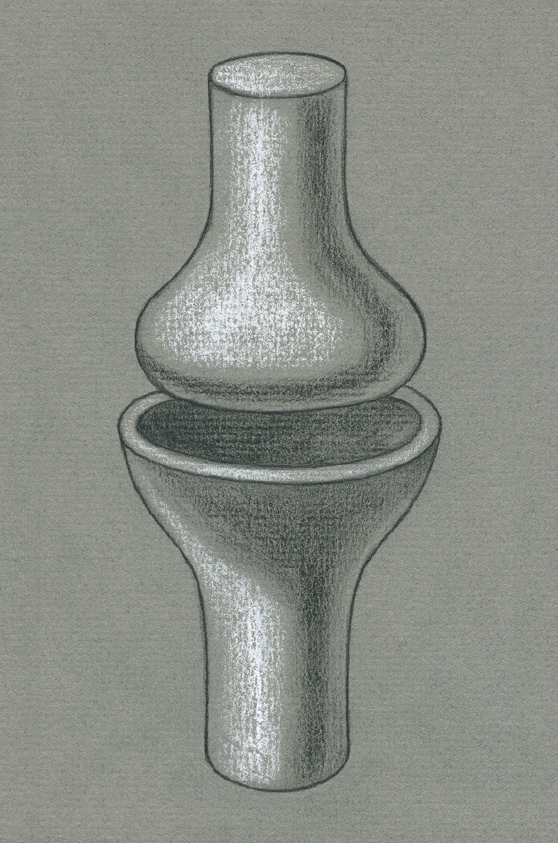
In an ellipsoid joint, the end of one bone, shaped like an elongated oval, fits into the elongated, oval-shaped cavity of another bone.
An ellipsoid joint, or condyloid joint, is similar to a ball-and-socket joint, but the shapes of the head of one bone and the socket of the other bone are more elongated—oval rather than round. Movements produced by ellipsoid joints are therefore slightly more limited than those enabled by ball-and-socket joints. Ellipsoid joints are located at the connection of the head and neck (atlanto-occipital joint), wrist (radiocarpal joint), and knuckles of the hand (metacarpophalangeal joints).
In addition to the joints described previously, there is what is called a functional joint. For example, the articulation between the scapula bone and the posterior portion of the rib cage is not a true joint because the scapula and rib cage are not held together with connective tissues such as ligaments, nor does it have a joint capsule. However, this articulation does function as a joint, hence the term.
Basic Joint Movements
Muscles contract to move bones at the joints. Movements include forward and backward motions, side-to-side motions, and rotational motions of bones or body parts. Each of these movements has a name identifying the direction of the movement. For every basic action there is a reverse action, so the terms are usually paired. For example, the torso can bend forward at the waist in the movement called flexion, then return to its original upright position in the movement called extension. In addition, most movements can be characterized as angular, rotational, circular, or gliding.
An angular movement changes the angle between two bones (increasing or decreasing the joint angle). Angular movements include flexion and extension as well as abduction and adduction.
In a rotational movement, a bone rotates on its own axis without changing its position spatially. These movements include medial and lateral rotation as well as pronation and supination.
In a circular movement (circumduction), a bone or body part produces a movement in a cone-shaped configuration, with the apex of the imaginary cone located at the joint initiating the action. In other words, one end of the bone (within the joint) is somewhat stationary while the other end of the bone moves in a circular fashion.
In gliding movements, one bone glides over another bone to produce a limited action. These movements include protraction and retraction as well as eversion and inversion.
Note that the overall movement of a joint can also include subsidiary movements in which one bone surface slides over, rolls over, or spins around another. A combination of these three types of motions can be found, to a greater or lesser degree, in all synovial-joint movements.
Anatomical Planes
To help classify the different directions of bodily movements, anatomists have formalized a system of three basic anatomical planes in relation to the body standing in the anatomical position—which, again, is the position of a standing figure whose head and palms of the hands are facing forward and whose weight is evenly distributed on both feet. The anatomical planes—called the sagittal, coronal, and transverse planes—are used for reference when identifying the various angular and rotational movements of the joints. Think of these imaginary planes as flat, two-dimensional spatial fields or as sheets of transparent glass slicing through the body perpendicularly to each other. Certain movements can take place only within certain planes.
The sagittal plane divides the body vertically into equal right and left halves. Movements within the sagittal plane are flexion and extension—forward and backward movements of the head, spine, and limbs.
The coronal plane divides the body vertically into equal front (anterior) and back (posterior) portions. Movements within the coronal plane are abduction and adduction (side-to-side movements of the arms and legs), as well as lateral flexion (a side-to-side movement of the head, neck, or torso).
A transverse plane divides the body horizontally into upper (superior) and lower (inferior) portions. Movements within a transverse plane include the rotation of the head, spine, or limbs.
Although, as I say above, certain movements are restricted within the boundaries of one of these planes, many complex actions occur in two or three planes: think of a baseball pitcher moving the whole arm in a circular manner to pitch the ball, or a martial arts master executing a powerful kick.
ANATOMICAL PLANES

Anterior three-quarter view of a figure in the anatomical position
 Sagittal plane
Sagittal plane
Movements in this plane are forward and backward movements of the head, spine, and limbs.
 Coronal plane
Coronal plane
Movements in this plane are side-to-side movements of the head, neck, torso, and limbs.
 Transverse plane
Transverse plane
Movements in this plane are rotations of the head, spine, and limbs.
The Individual Joints of the Skeleton
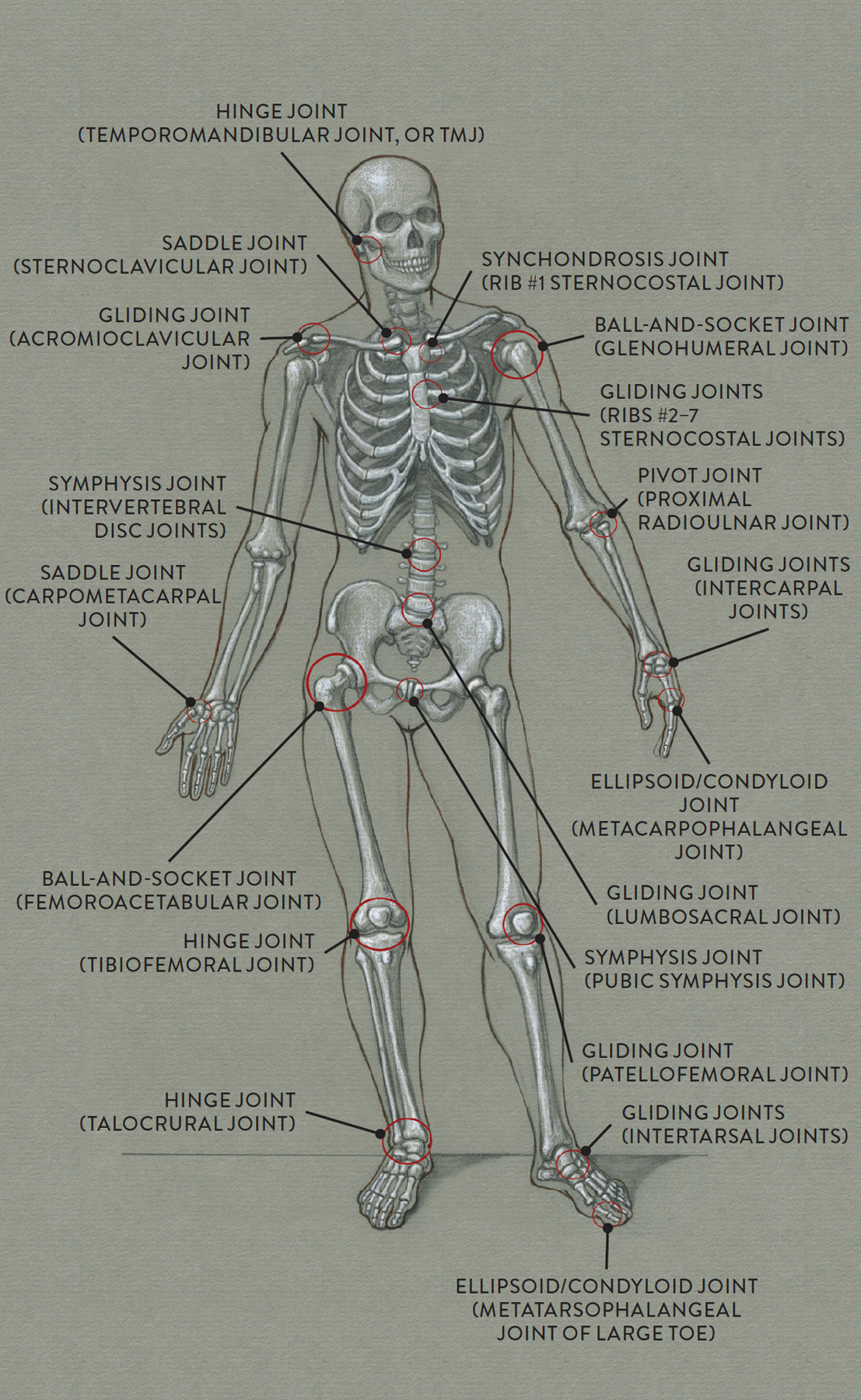
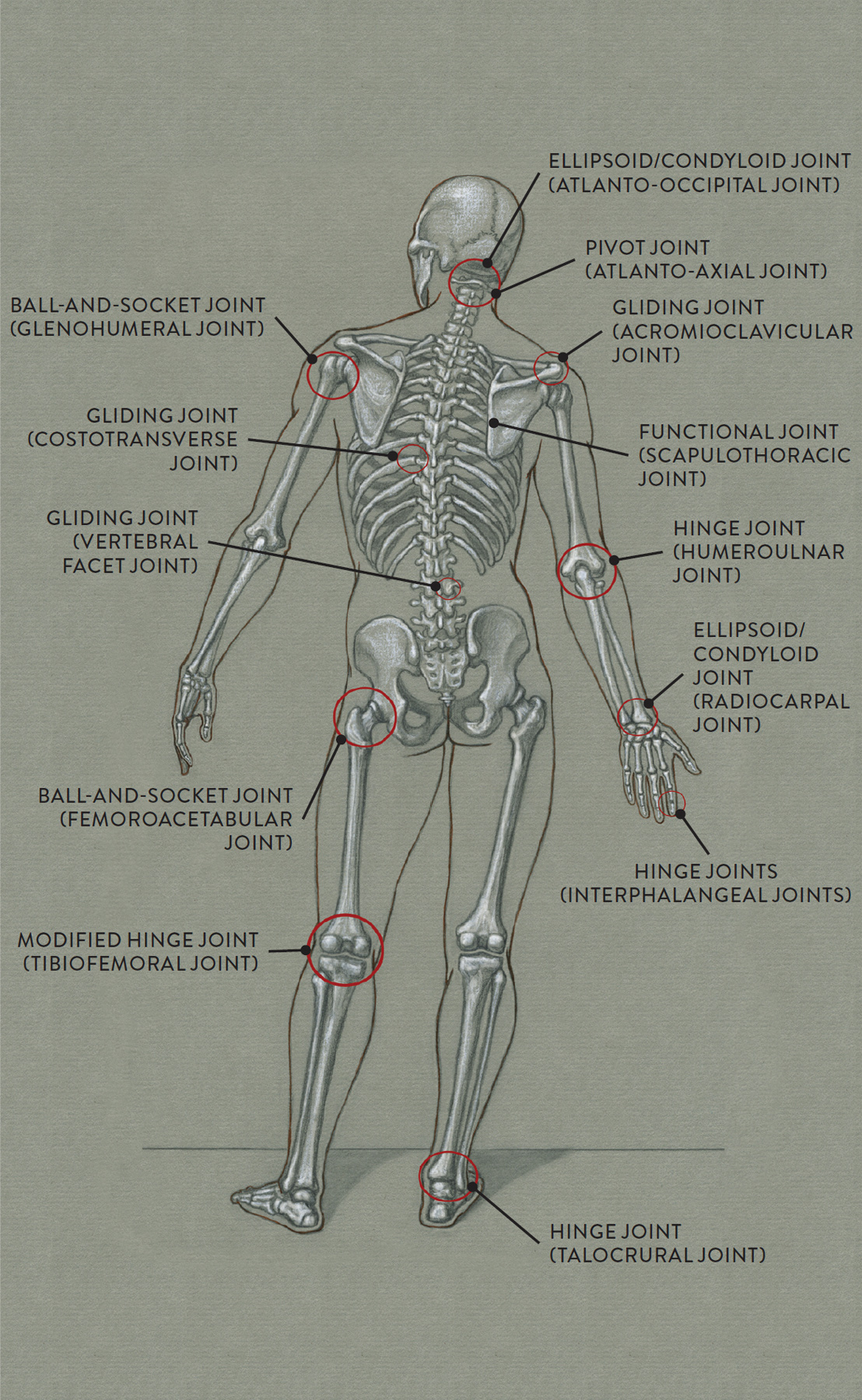
We will now move through the whole skeleton and examine the main joints of each section of the body. The description of the joint will be followed by the kind or kinds of movement it produces. Locations of the most important joints and the category to which each belongs are identified in the following drawings.
LOCATION OF MAIN JOINTS OF SKELETON—ANTERIOR VIEW
LOCATION OF MAIN JOINTS OF SKELETON—POSTERIOR VIEW
Mandible Joint
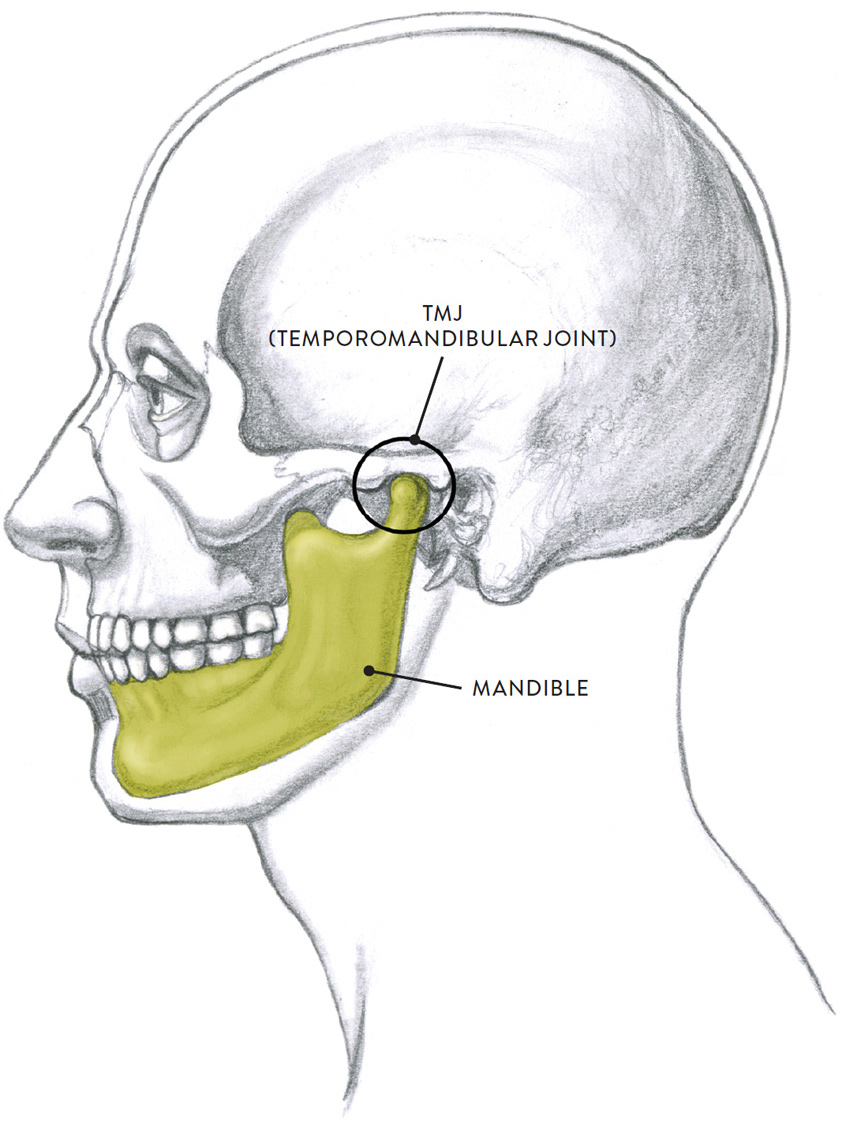
All the joints of the cranium, with one exception, are suture (fused) joints, incapable of any movement. These joints are seen on skulls as zigzagging lines on the dome of the cranium and a few of the facial bones. The only moveable joint of the cranium is the temporomandibular joint, or TMJ.
The TMJ is the articulation between the condylar process (a pronglike structure on the lower jaw) and the condylar fossa (a depression) of the temporal bone of the skull. Located directly in front of the ear, the TMJ cannot be seen on the surface, as it is covered with ligaments, muscles, and soft-tissue forms. The TMJ’s appearance is similar to that of an ellipsoid/condyloid joint, but it is classified as a modified hinge joint.
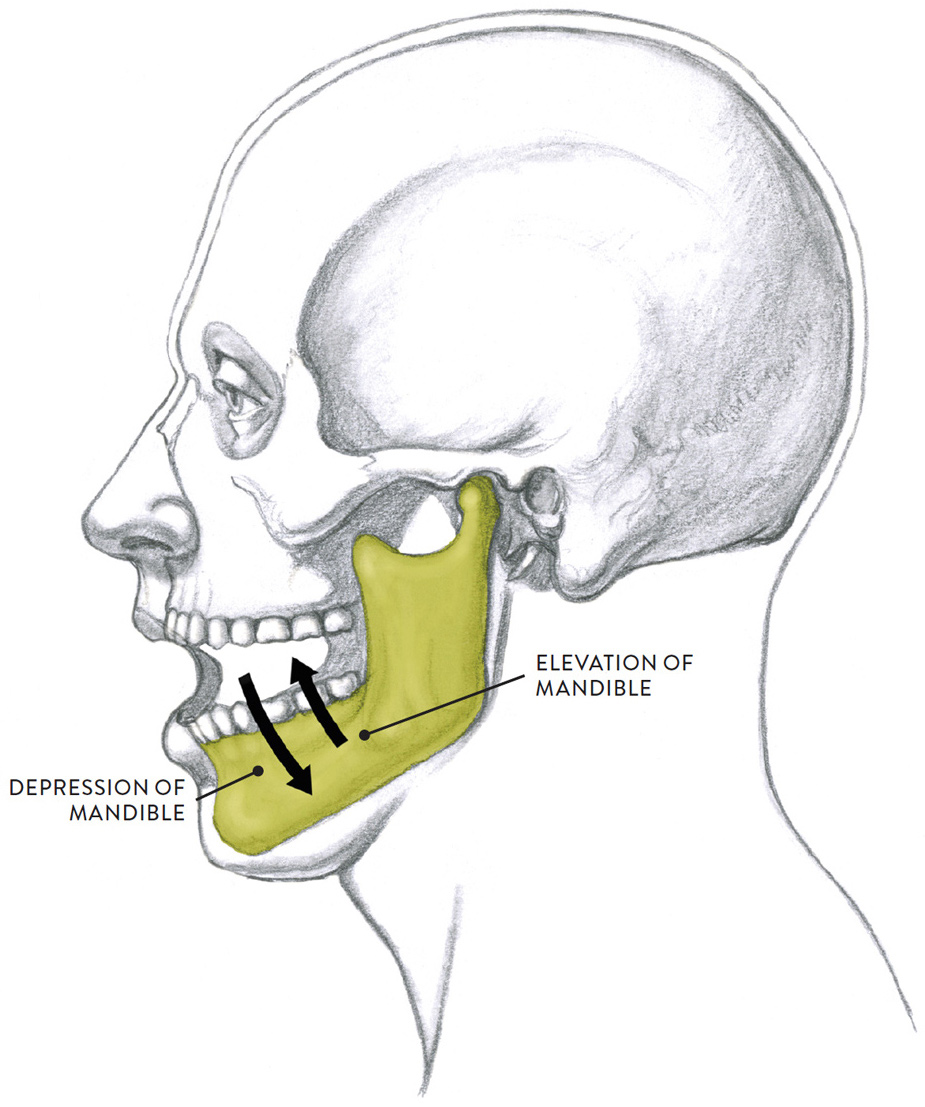
The mandible is capable of three types of movement: depression and elevation (opening and closing of the lower jaw), protraction and retraction (forward and backward movement of the lower jaw), and lateral excursion (the side-to-side movements of the lower jaw, also known as left and right deviation). These jaw movements are utilized mainly for chewing and grinding food, but also in certain vocalizations when the jaw is open.
The next drawing, Depression and Elevation of Mandible at the TMJ (Temporomandibular Joint), shows the hinge-like movement of the jaw. Depression is the lowering of the jaw, opening the mouth wide. Elevation is the movement of returning the jaw back to its normal position. These movements are seen in various facial expressions and in vocalizations in which the jaw is dropped and mouth opened to project the voice when singing or calling out.
DEPRESSION AND ELEVATION OF MANDIBLE AT THE TMJ (TEMPOROMANDIBULAR JOINT)
Modified hinge joint action
Lateral view of cranium
Neutral position of mandible
Lateral view of cranium
Actions of the mandible
Joints of the Vertebral Column, Rib Cage, and Pelvis
This section covers the cervical joints of the neck, the thoracic vertebral joints of the rib cage, the lumbar joints between the rib cage and pelvis, and the lumbosacral joint of the pelvis, as well as several additional joints of the rib cage and pelvis. We will see how the joints of the cervical (neck) vertebrae move the cranium and how the joints of the thoracic and lumbar region help move the rib cage and pelvis in different directions as whole units.
The Joints of the Vertebral Column
Most of the movement in the vertebral column occurs in the neck region (cervical vertebrae) and the small of the back (lumbar vertebrae), with minor movements occurring in the rib cage (thoracic vertebrae). The range of motion of the vertebral column depends on many factors: An individual’s level of fitness can make a difference in the motion capability of his or her vertebral column. Athletically trained people have more flexibility in their spines than people who are sedentary. Other contributing factors include the flexibility or resistance of the muscles and ligaments of the back and the condition of the various vertebral bones and joints. Age plays a factor, with elderly people tending to lose flexibility of the vertebral column due to bone and disc degeneration.
The joints of the vertebrae, shown in the next drawing, include both cartilaginous and synovial joints. Let’s look at the two basic vertebral joint types: intervertebral joints and vertebral facet joints.
JOINTS OF VERTEBRAL COLUMN—LATERAL VIEW
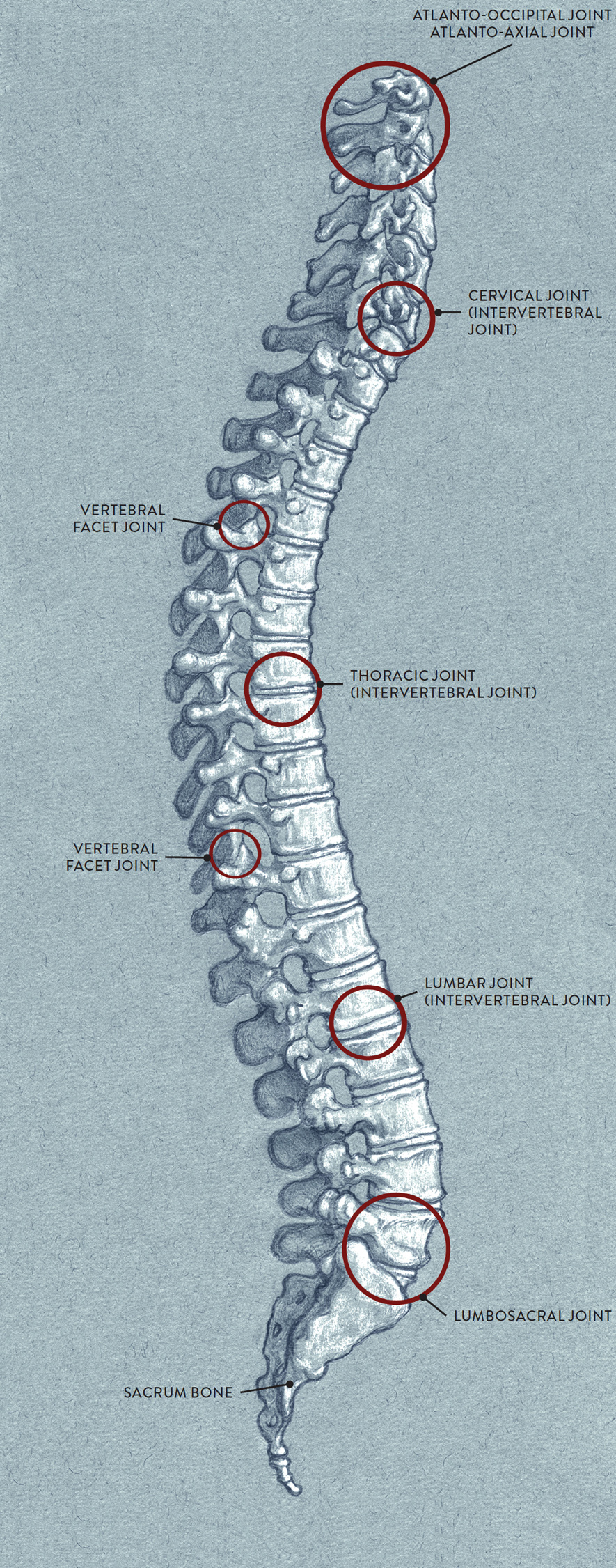
Intervertebral joints (pron., in-ter-VER-teh-brul), also called disc joints, are cartilaginous joints located between the drumlike shapes of the vertebrae. A fibrocartilaginous pad called the intervertebral disc is positioned between every two vertebrae with the exception of C1 and C2. These discs serve as protective cushions, reducing the friction between bones during joint action, and also act as shock absorbers and weight-bearing structures.
Vertebral facet joints are synovial joints located on the vertebral arches. A facet on one vertebral arch articulates with a facet of the adjacent vertebral arch. These joints are considered gliding, or plane, joints.
The cervical, or neck, vertebrae play an important role not only in supporting the weight of the cranium but in allowing the head to move in different directions. The two primary joints of this region are the atlanto-occipital joint and the atlanto-axial joint.
The atlanto-occipital joint (pron., at-LAN-toe ock-SIP-ih-tal), or AOJ, is the joint between the occipital bone of the cranium and the first cervical vertebra (atlas, or C1). It is classified as an ellipsoid/condyloid joint. The main actions at the AOJ are flexion and extension—rocking the head back and forth, as when nodding “yes.” Other actions include lateral flexion and circumduction of the head and neck.
The atlanto-axial joint (pron., at-LAN-toe AXE-see-al), or AAJ, is the joint between the first cervical vertebra (atlas, or C1) and second cervical vertebra (axis, or C2). The articulation occurs between the odontoid process (or dens), a small bony projection on the axis vertebra, and the inner surface of the atlas vertebra. The atlanto-axial joint, classified as a pivot joint, allows rotational movement of the head and neck, as when the head swivels to the right and left in shaking the head “no.” The drawing below shows the atlanto-occiptal and atlanto-axial joints.
ATLANTO-OCCIPITAL AND ATLANTO-AXIAL JOINTS
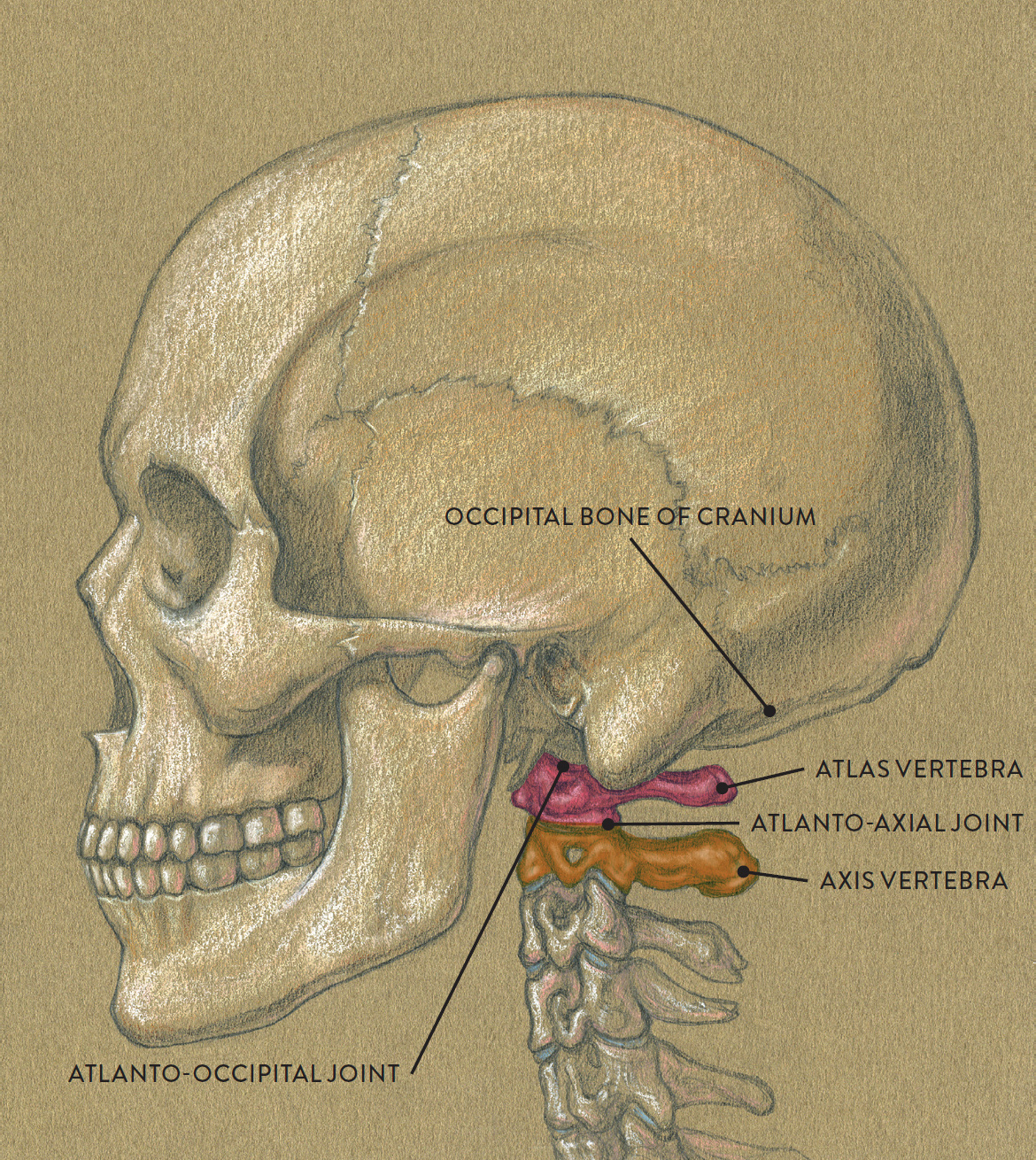
Lateral view of cranium and upper cervical vertebrae
Names of Vertebral Joints
The names of vertebral joints provide clues to their location:
· Occipital pertains to the occipital region of the cranium.
· Atlanto pertains to the first cervical (atlas) vertebra.
· Axial pertains to the second cervical (axis) vertebra.
· Costo pertains to a rib.
· Vertebral pertains to the body of a vertebra.
· Transverse pertains to the transverse processes of a vertebra.
· Lumbo pertains to the lumbar vertebrae.
· Sacral pertains to the sacrum bone.
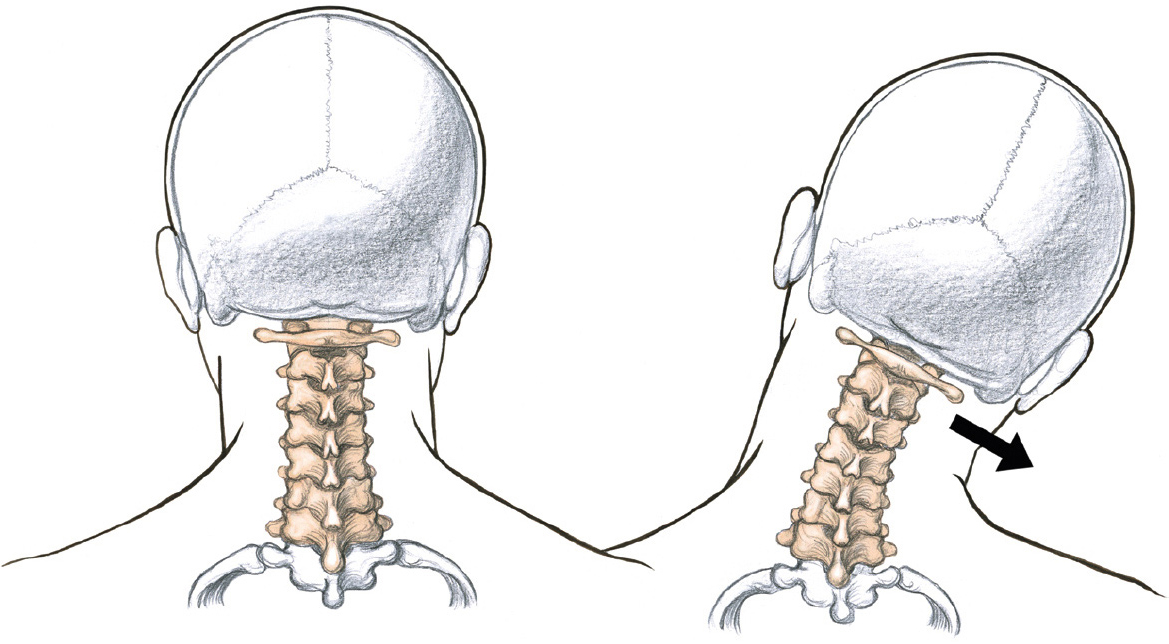
Now let’s look at how the whole neck participates in moving the head. Movements of the neck and head include flexion and extension (bending the head and neck forward and back), lateral flexion (bending the head and neck to the side), and rotation (horizontal swiveling of the head and neck). The next drawing, Flexion and Extension of Head and Neck at Cervical Vertebral Joints, shows the head and neck moving in a forward and back direction. Flexion is the action of bending the head forward and downward toward a stationary rib cage, and extension is the return of the head and neck to its normal position. Bending the head back with the chin lifting upward is sometimes called hyperextension—that is, extending the body part beyond the normal limit.
FLEXION AND EXTENSION OF HEAD AND NECK AT CERVICAL VERTEBRAL JOINTS
Gliding joint action
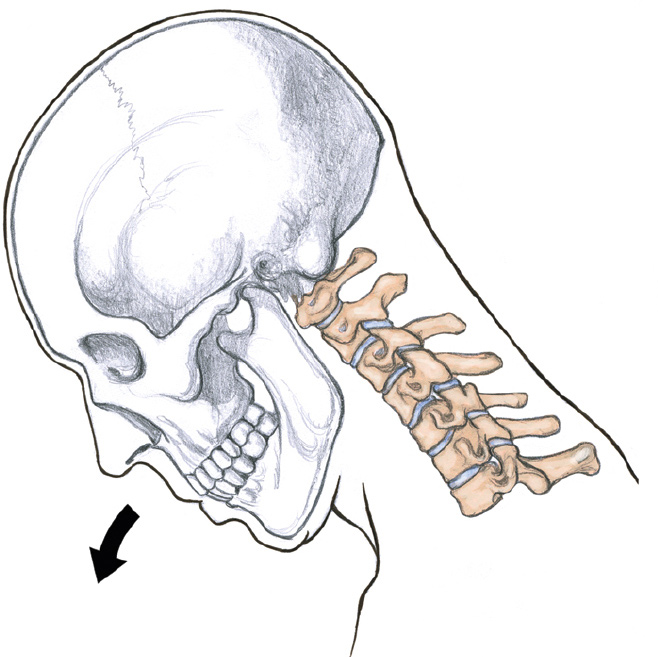
Flexion of head and neck
Head bends forward with chin pulling in.
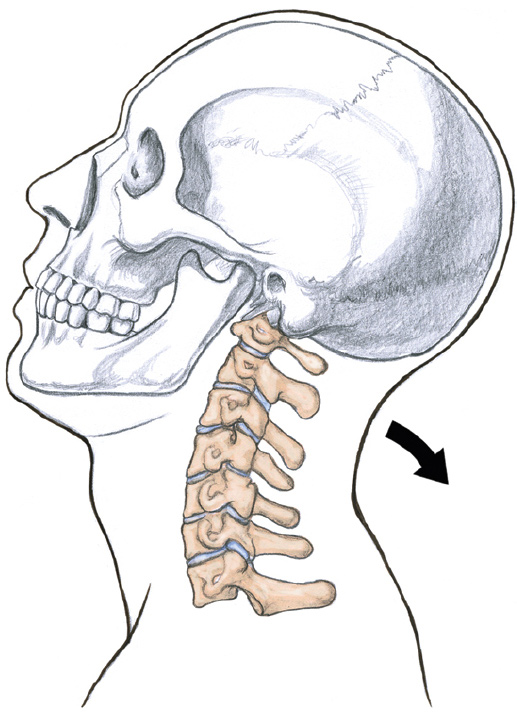
Extension of head and neck
Head bends back with chin pulling up.
In the drawing Lateral Flexion of Head and Neck at Cervical Vertebral Joints, we see the head and neck moving sideways. Lateral flexion is the bending of the head toward either the right or left shoulder. This action causes one side of the neck to stretch while the other side contracts.
LATERAL FLEXION OF HEAD AND NECK AT CERVICAL VERTEBRAL JOINTS
Gliding joint action
Head and neck tilt toward right shoulder. (Head can also tilt toward the left shoulder, in left lateral flexion.)
LEFT: Neutral position of head and neck
RIGHT: Right lateral flexion
Finally, in the drawing Rotation of Head and Neck at Cervical Vertebral Joints, shown next, we see how the head and neck swivel or turn. When the rib cage is stationary, the head and neck can rotate either to the right or to the left. There is, however a limitation in the rotational movement because of the configuration of the cervical vertebrae and the ligaments attaching to them. Ordinarily, the chin cannot move past the shoulder line; however, if the head tilts dramatically back and rotates, then the chin can move slightly past the shoulder.
ROTATION OF HEAD AND NECK AT CERVICAL VERTEBRAL JOINTS
Pivot and gliding joint action
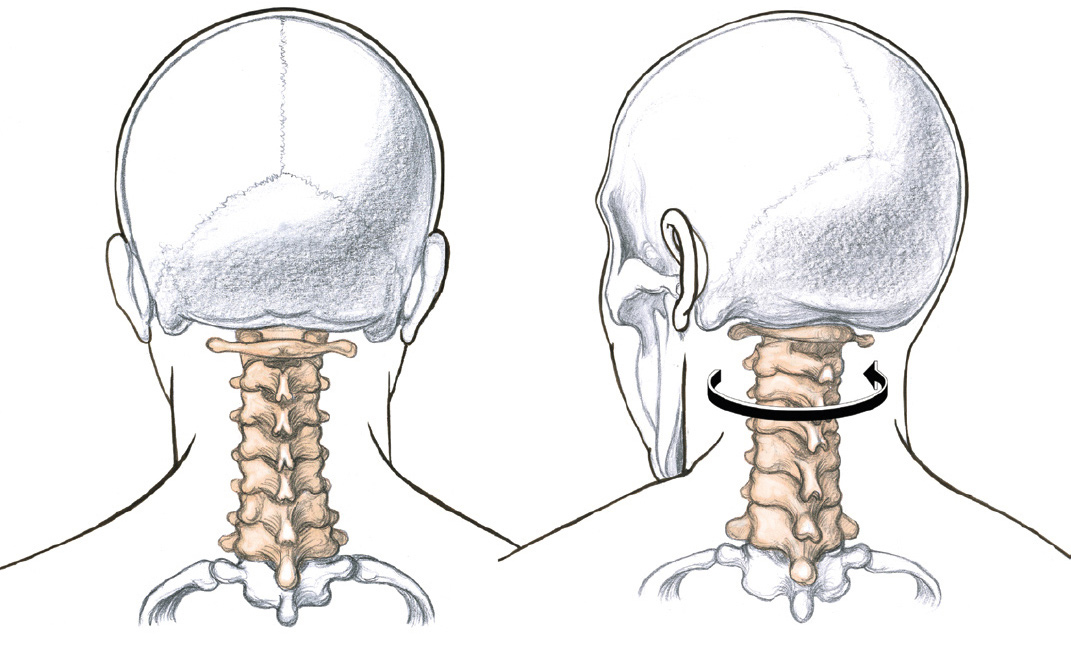
The head and neck can also rotate toward the right (right rotation).
LEFT: Neutral position of head and neck, posterior view
RIGHT: Left position of head and neck, posterior view
The Joints of the Rib Cage
The rib cage consists of twelve pairs of ribs that connect to two primary bony structures: the thoracic vertebrae (positioned in the posterior region of the rib cage), and the sternum (positioned in the anterior region of the rib cage). Note that the three pairs of false ribs do not connect directly to the sternum, and that the two pairs of floating ribs at the bottom of the rib cage do not connect to the sternum at all. Let’s look first at the connections between the ribs and the vertebral column, as shown in the drawing Joints of Rib Cage and Vertebral Column.
JOINTS OF RIB CAGE AND VERTEBRAL COLUMN
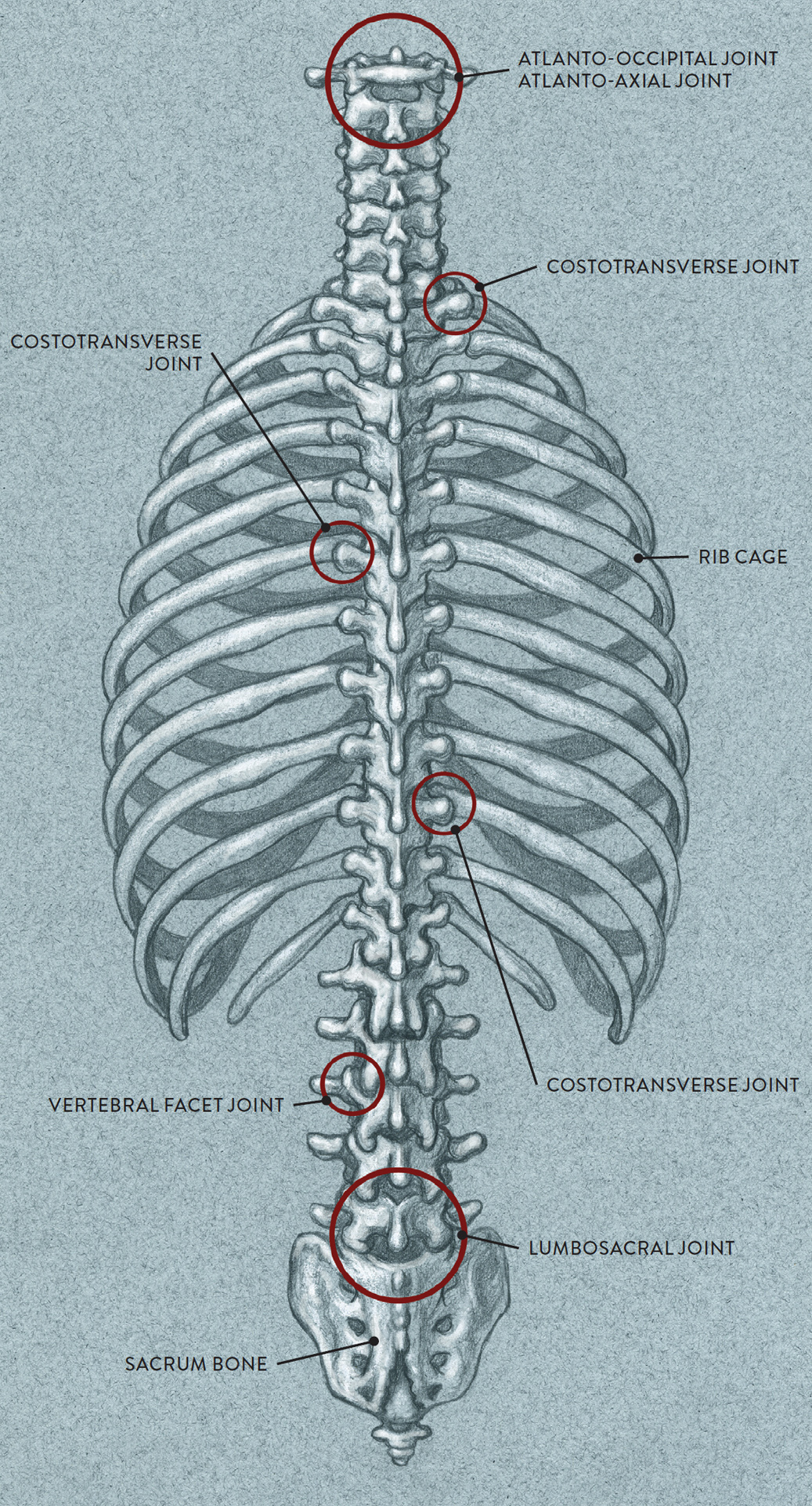
Posterior view
Throughout the vertebral column we see the numerous intervertebral joints and vertebral facet joints, as discussed above. Additional joints occur as the ribs connect into the vertebral column. These are called the costotransverse joints and the costovertebral joints. A costovertebral joint (pron., CO-sto-VER-teh-brul) connects a rib to the drumlike body of a vertebra; this type of joint can be seen in the drawing of the anterior region of the rib cage on this page. A costotransverse (CO-sto-TRANS-verse) joint connects a rib to the transverse process of a vertebra (the horizontal bony protrusion). The term costo means “rib,” and this prefix helps clarify that these particular joints occur only when the ribs attach directly into the thoracic vertebrae.
Names of Rib Cage Joints
The names of rib cage joints provide clues to their locations:
· Costo or costal pertains to the ribs.
· Vertebral pertains to the vertebrae.
· Sterno pertains to the sternum (breastbone).
· Chondral pertains to cartilage.
Now, let’s look at the placement of the joints connecting the ribs to another primary bony structure—the sternum (breastbone), positioned in the anterior portion of the rib cage. As shown in the next drawing Joints of Rib Cage and Sternum, these joints are the sternocostal joints (located between cartilage and sternum), the costochondral joints (between rib and cartilage), and the interchondral joints (between cartilage sections in the thoracic arch). The sternum itself has two separate joints: the manubriosternal joint and the xiphisternal joint.
The joints between the costal cartilages of the first seven ribs and sternum are called the sternocostal joints (pron., STER-no-CO-stol). The articulation of the first rib and the sternum produces no movement because it is a cartilaginous joint. The joints between the sternum and ribs numbers 2 through 7 are gliding/plane joints that produce minimal gliding movements, usually not noticeable on the surface.
JOINTS OF RIB CAGE AND STERNUM
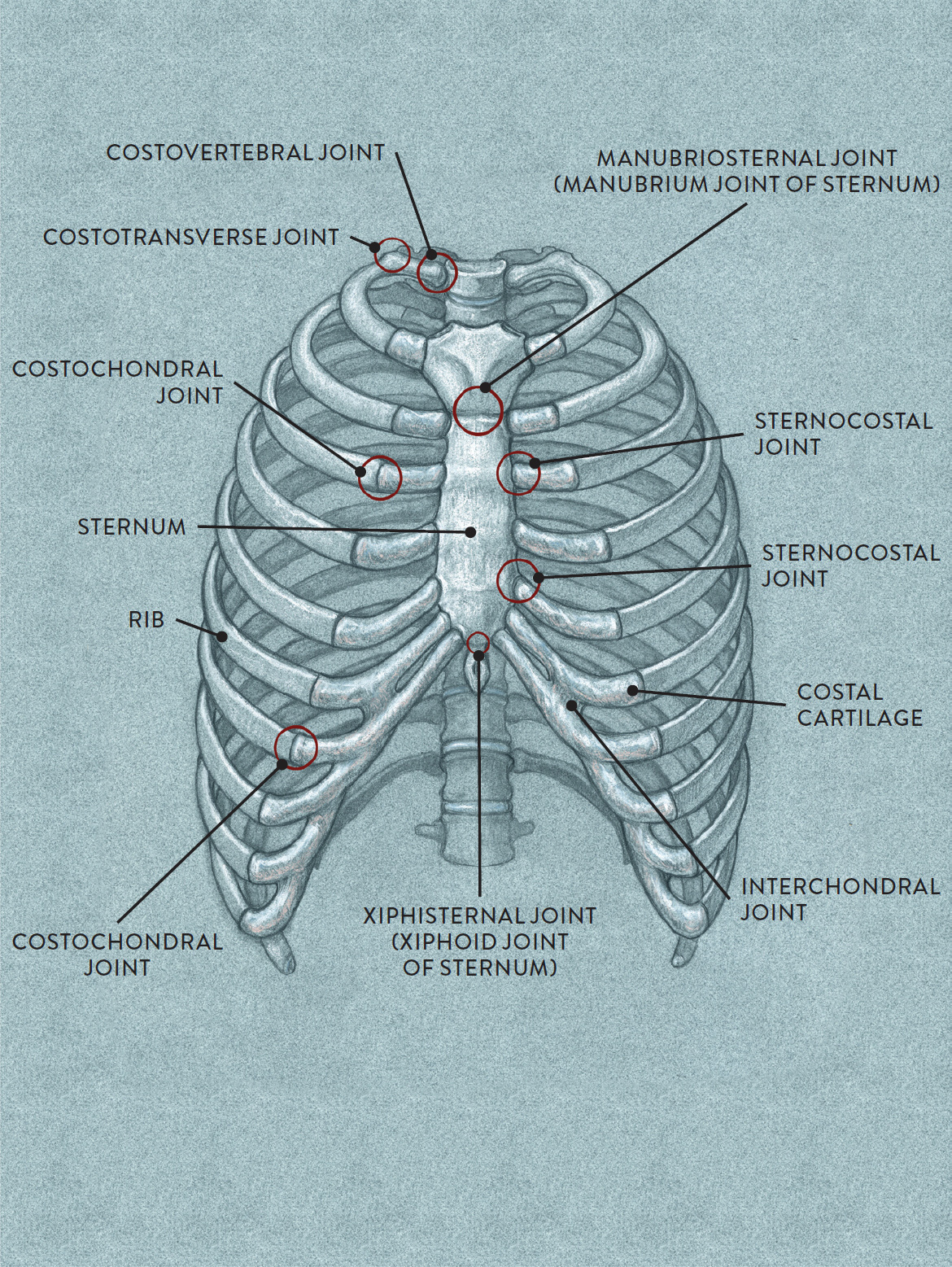
Anterior view
The costochondral joints (pron., co-sto-CON-drul) are between the ribs and the costal cartilage. Since there are no joint capsules, there is very little motion at these joints.
The interchondral joints (pron., in-ter-CON-drul) are small fibrous connections between the costal cartilage in the thoracic arch region. They are considered gliding/plane joints.
The first of the sternum joints is the manubriosternal joint (pron., maa-NEW-bree-oh-STERN-ul), which is between the manubrium of the sternum and the body of the sternum. It is a symphysis type of cartilaginous joint but often fuses together in middle age or later. The other sternum joint, the xiphisternal joint (pron., ZIF-ih-STERN-ul), is between the xiphoid process and the body of the sternum. It is a synchondrosis type of cartilaginous joint but also fuses together in middle age or later.
Movement is minimal at the rib cage joints, activated mainly during breathing. During inhalation the diaphragm contracts and moves downward to allow the lungs to expand, filling with air; the ribs are pulled slightly upward and out, much like levers, to widen the rib cage. In exhalation, the ribs, diaphragm, and lungs return to their normal position. Although these movements are subtle and hard to detect during normal breathing, you can clearly see them when watching the rib cage of an athlete after an exhausting event, such as a sprint.
In the drawing Rib Cage Movement during Respiration, we see the rib cage on the left in the normal state. The middle drawing shows the rib cage immediately after inhalation, when the lungs are filled with air. On the right we see how the rib cage returns back to normal position immediately after exhalation.
RIB CAGE MOVEMENT DURING RESPIRATION
Arrows indicate directional movement within rib cage.
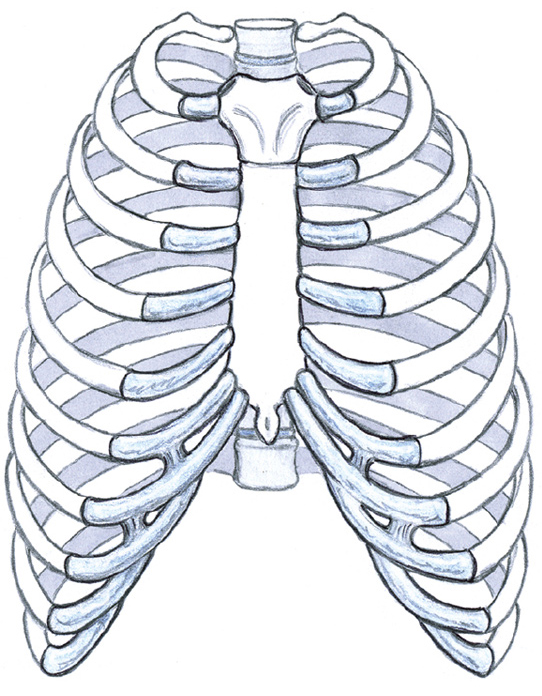
Normal position of rib cage.
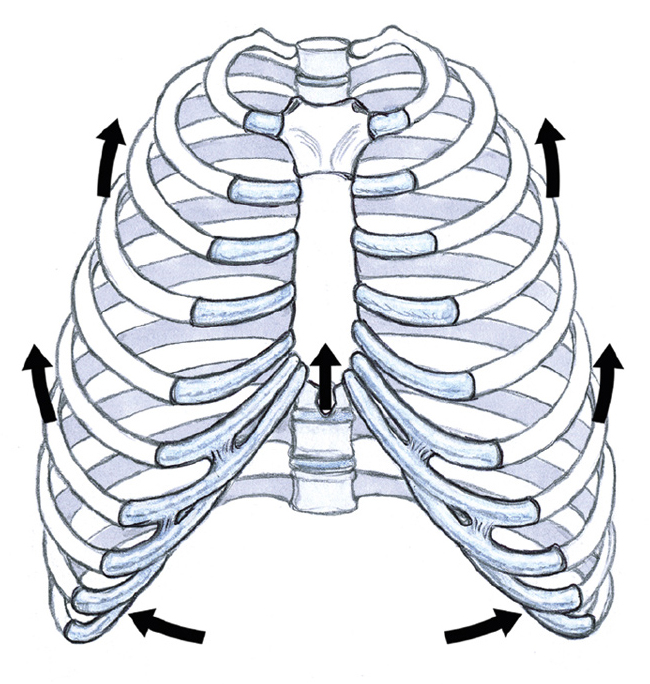
The lungs fill with air.
Inhalation
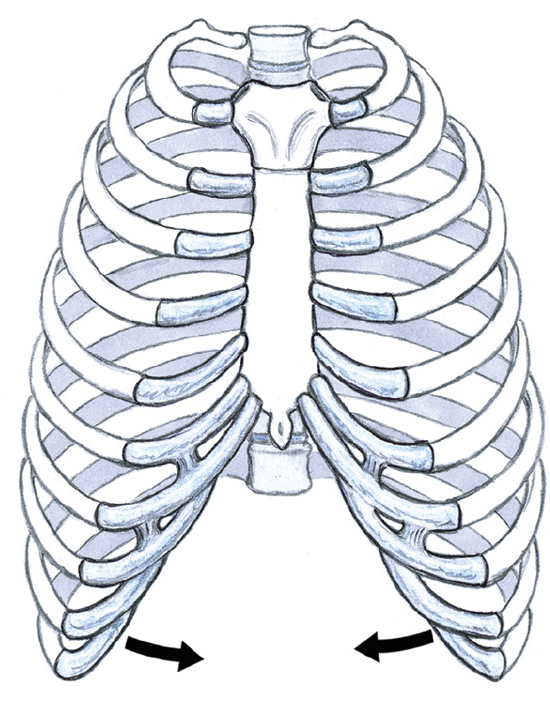
Air is expelled from the lungs, and the position of the rib cage returns to normal.
Exhalation
Movements of the Vertebral Column with the Rib Cage
Because the ribs connect into the thoracic vertebrae, restricting movement, the thoracic joints are not as flexible as the cervical or lumbar joints. Whenever there is movement of the vertebral column, the rib cage generally moves as a single unit, in a forward or backward direction (flexion and extension), bending sideways (lateral flexion), or twisting or swiveling (rotation).
In the drawing Flexion and Extension of Rib Cage at the Vertebral Joints, we see how the rib cage moves in a forward and back direction. Flexion is the movement of bending the torso (rib cage and vertebral column) forward from a stationary pelvis. Extension is returning the torso to its normal position or bending the torso back, which is sometimes called hyperextension.
FLEXION AND EXTENSION OF RIB CAGE AT THE VERTEBRAL JOINTS
Gliding joint action
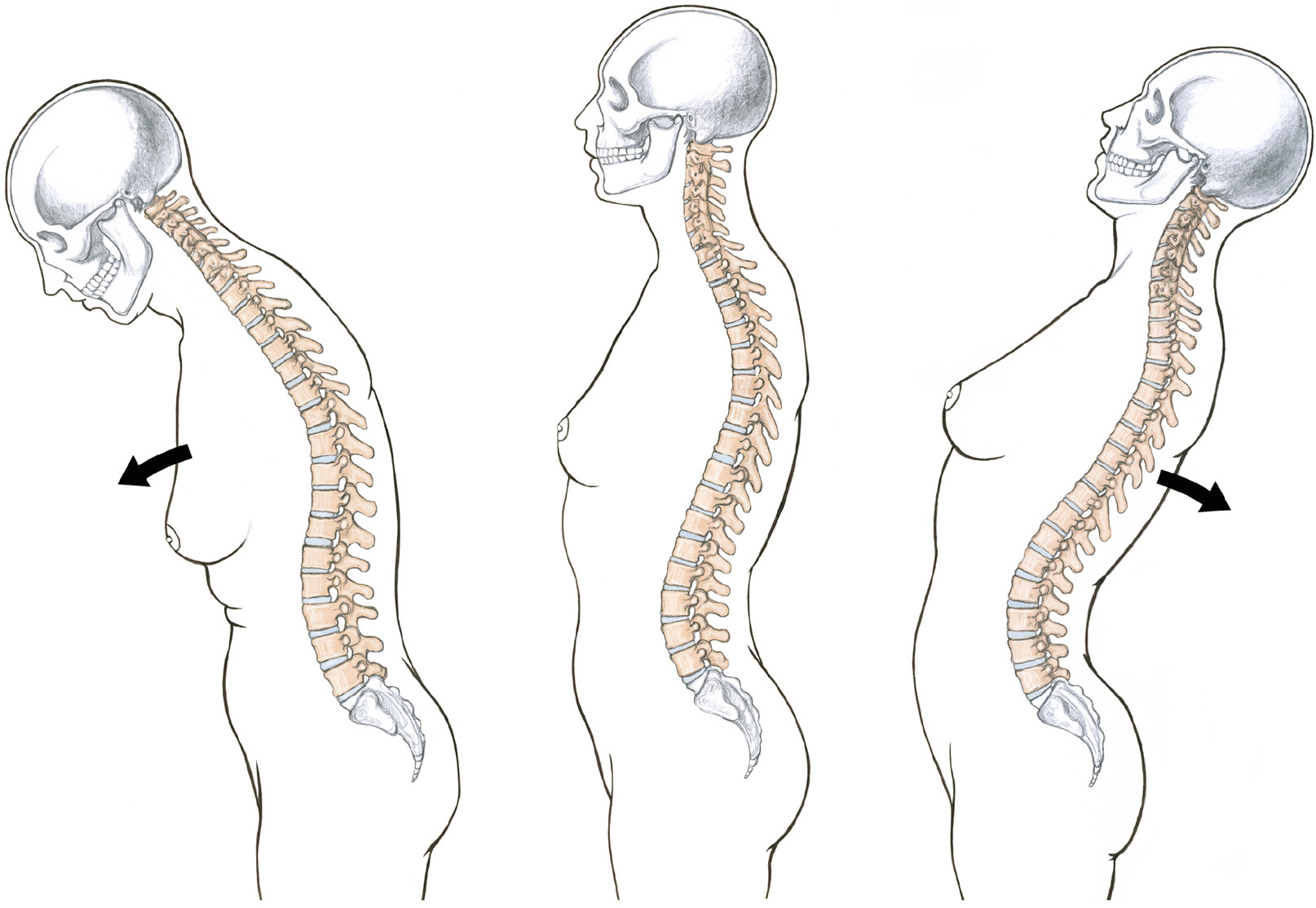
LEFT: Flexion of torso and vertebral column
CENTER: Neutral position of vertebral column, lateral view
RIGHT: Extension of torso and vertebral column
In the following drawing, Lateral Flexion of the Rib Cage at the Vertebral Joints, we see the torso bending in a side direction, called lateral flexion, from a stationary pelvis. The torso can, of course, bend toward either the right or left.
LATERAL FLEXION OF THE RIB CAGE AT THE VERTEBRAL JOINTS
Gliding joint action
Posterior view
The vertebral column is in neutral position.
LATERAL FLEXION OF THE RIB CAGE AT THE VERTEBRAL JOINTS (CONTINUED)
Gliding joint action
Posterior view
The figure leans toward the right from a stationary pelvis. (Movement can also be of the figure leaning toward the left.)
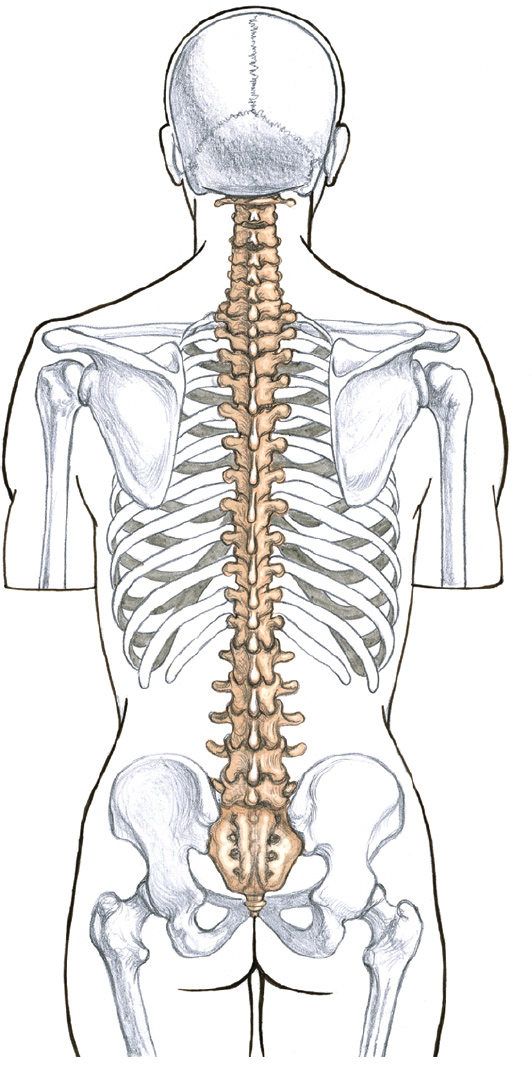
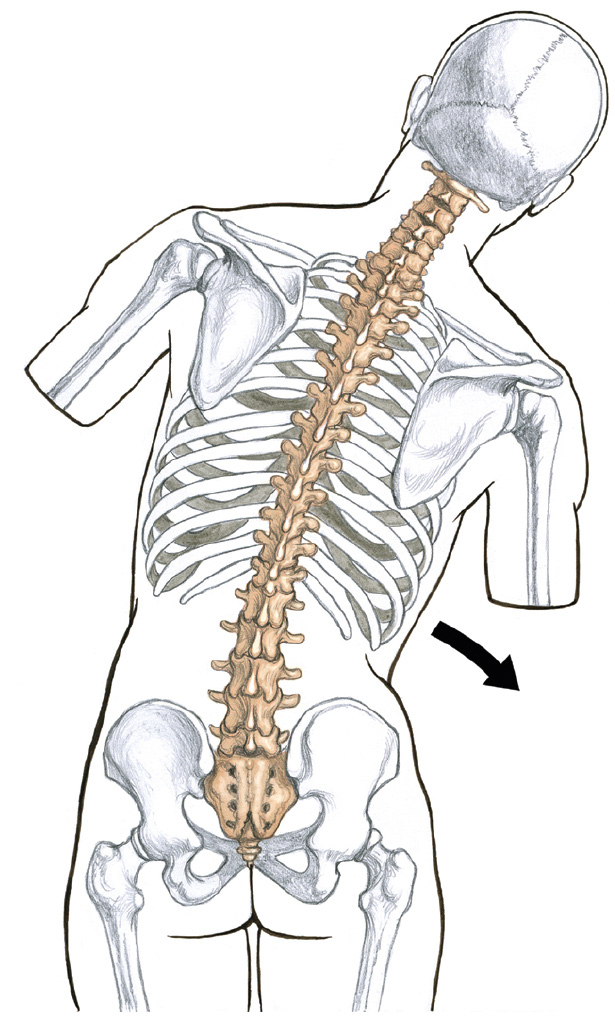
The drawing Rotation of the Rib Cage at the Vertebral Joints, shows how the rib cage can turn on the axis of the vertebral column, rotating the torso (cranium, rib cage, and vertebral column) toward either the right or left (right rotation, left rotation) from a stationary pelvis.
ROTATION OF THE RIB CAGE AT THE VERTEBRAL JOINTS
Pivotal and gliding joint action
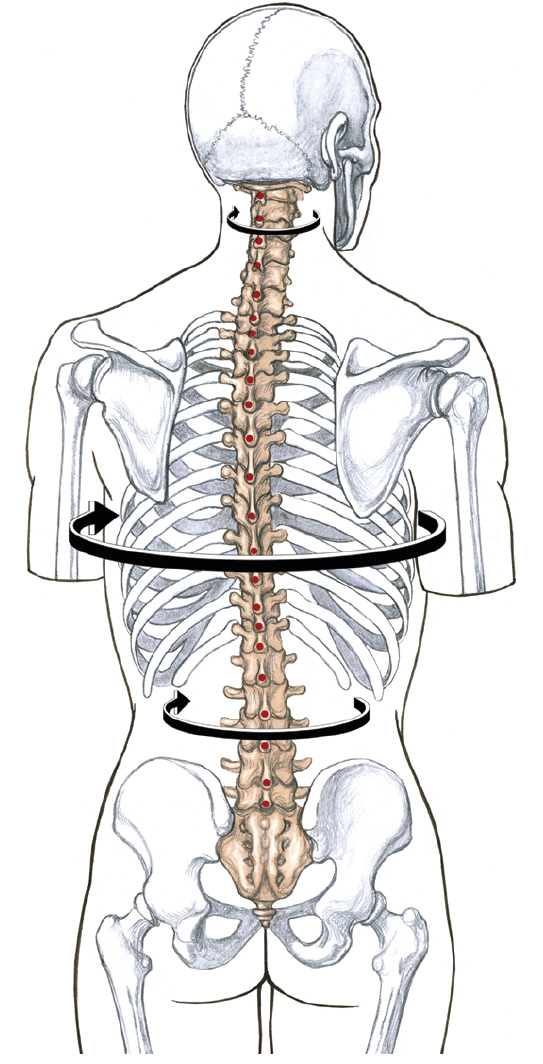
Posterior view
The torso, head, and neck are shown rotating toward the right. The torso, neck, and head can also rotate toward the left. Vertebral column in neutral position shown here.
RED DOTS
Positions of the spinous processes of the vertebral column
BLACK ARROWS
Pivotal movements of the head, neck, and rib cage from the vertebral column
The Joints of the Pelvis
As we move down the vertebral column beyond the rib cage, we encounter the lumbar vertebrae. These large forms help support the weight of the head, neck, and rib cage. The lumbar joints help move the rib cage when the pelvis is more or less stationary, but they also assist in moving the pelvis to various positions.
The joint between the last lumbar vertebra (L5) and the sacrum is called the lumbosacral joint (pron., LUM-bo-SAY-krul). This gliding/plane joint, along with the assistance of the other lumbar joints and the hip joint, allows the pelvis to move in slightly different directions as a whole unit.
JOINTS OF THE PELVIS
Anterior three-quarter view of pelvis
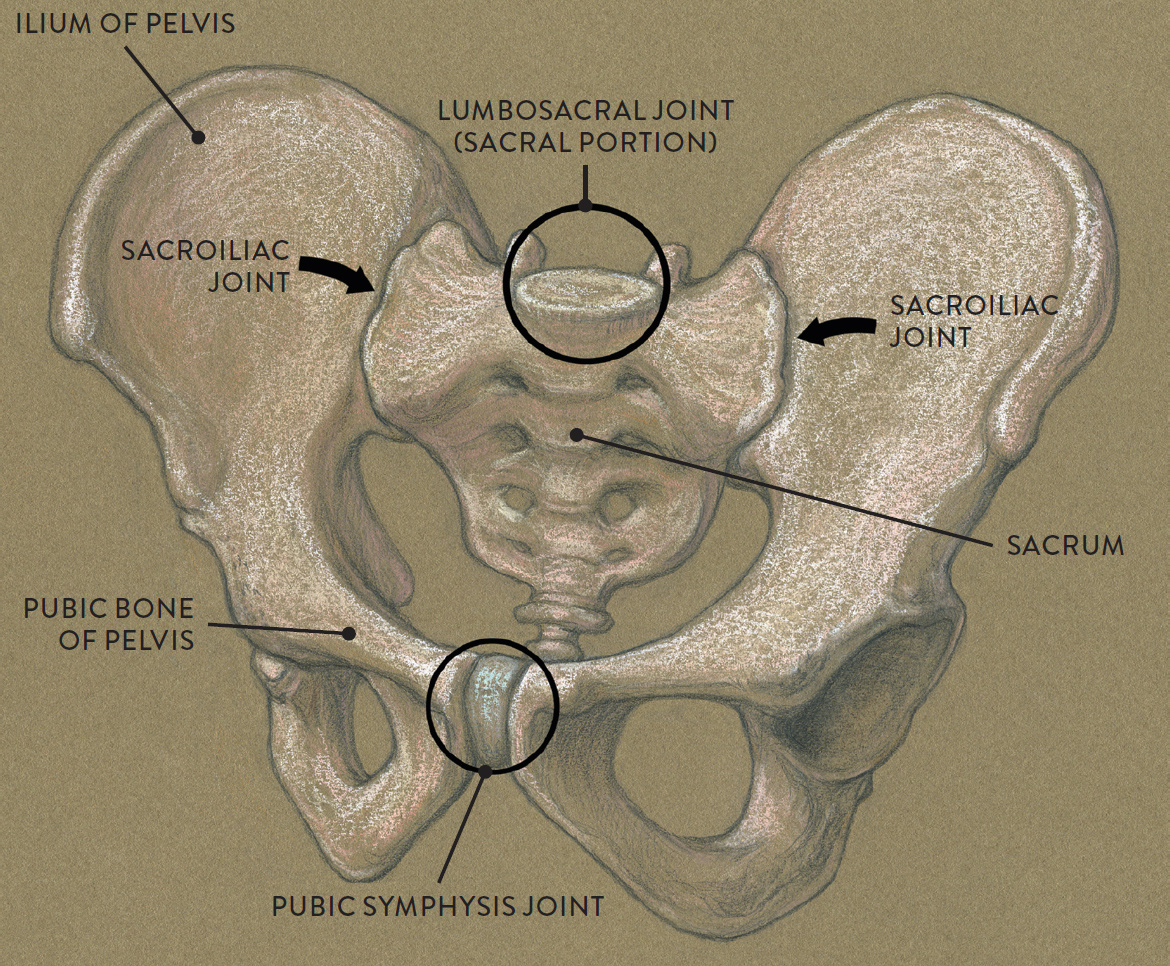
The pelvis contains two other types of joints—the two sacroiliac joints (pron., SAY-kro-IL-ee-ak; located between the sacrum and ilium) and the pubic symphysis joint (pron., PYOO-bic SIM-fih-sis; located between the two pubic bones). The sacroiliac and pubic symphysis joints are capable of small, limited gliding motions (interpelvic motions), too subtle to detect on the surface. Artists should think of the pelvis as a single structure that moves as a unit and not as individual bones shifting up or down.
Movements of the whole pelvis as a single unit include anterior and posterior pelvis tilts (tilting forward and backward), lateral flexion (bending of the pelvis to the side), and rotation of the whole pelvis toward either the right or left. The lumbar joints and hip joint (femoroacetabular joint) participate in these movements.
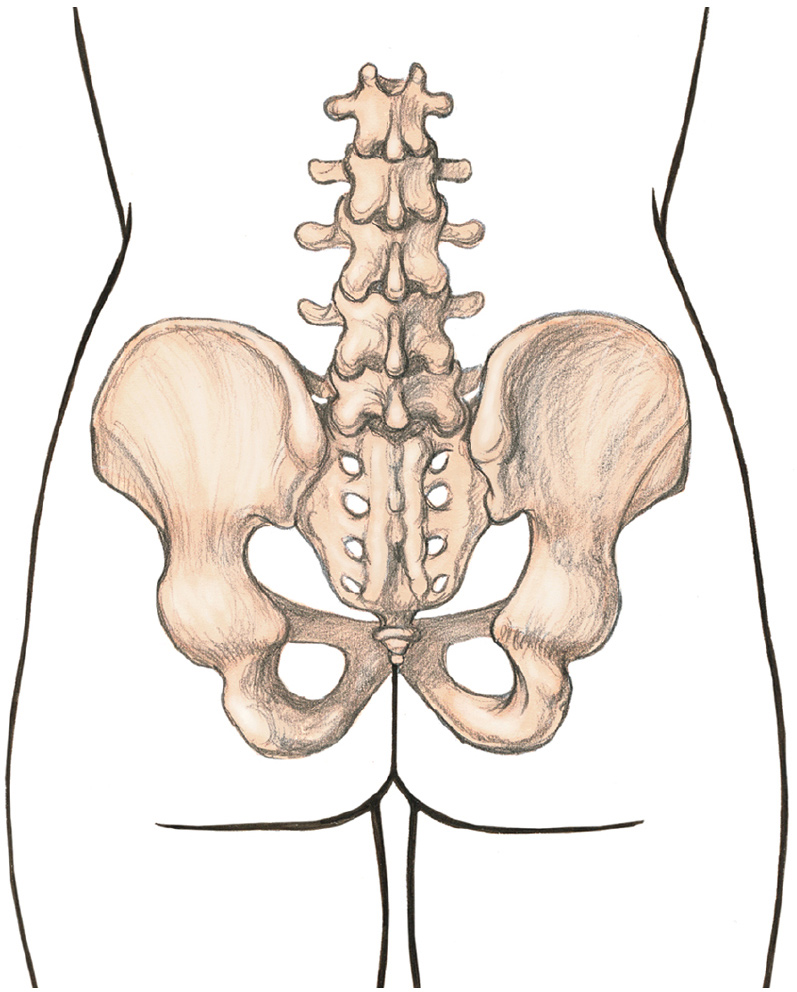
The drawing Anterior and Posterior Pelvic Tilts, shows the pelvis tilting in forward and backward directions. Anterior pelvic tilt (APT) is the tilting of the upper part of the pelvis in a forward and downward direction. The buttocks are lifted upward during this movement, and the vertebral column is usually arched. Posterior pelvic tilt (PPT) is the tilting of the upper part of the pelvis backward. The buttocks are tucked in during this movement.
ANTERIOR AND POSTERIOR PELVIC TILTS
Gliding joint action
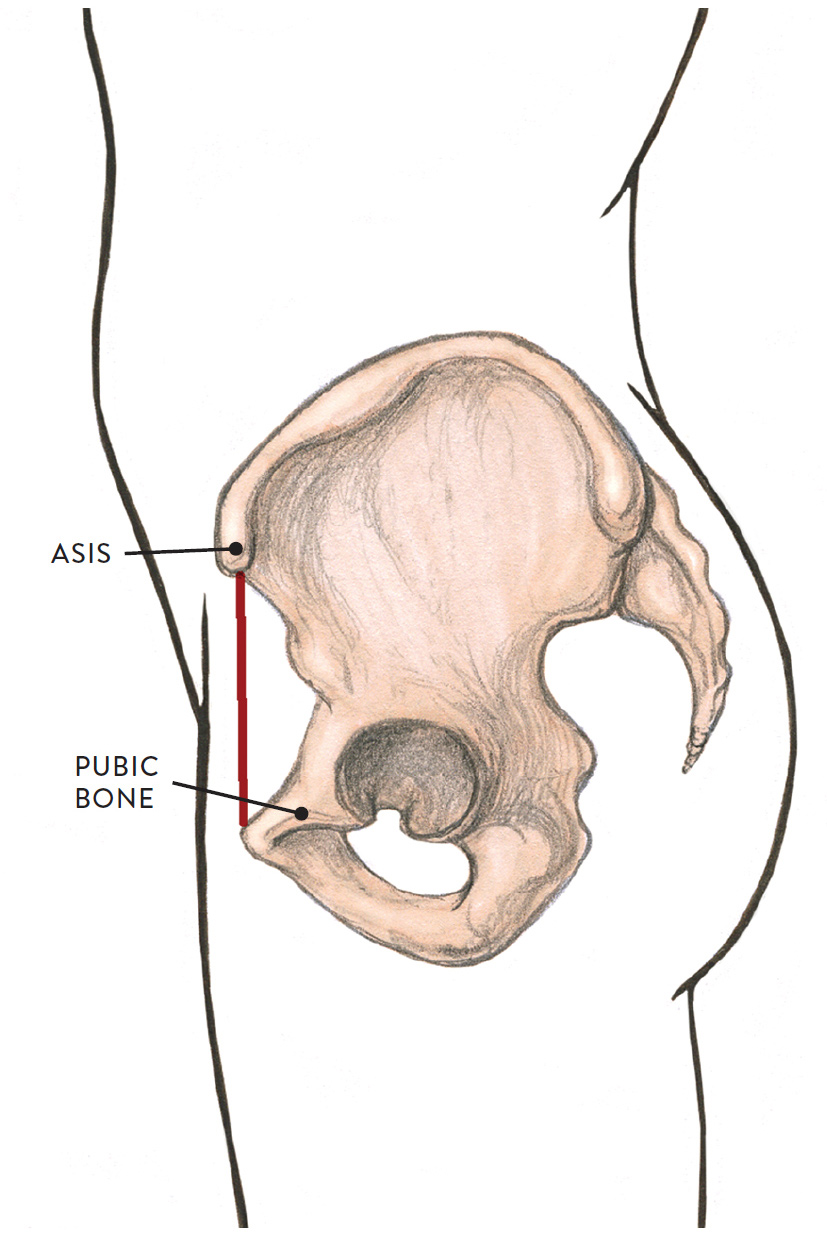
Neutral position of pelvis, lateral view
From a lateral view, the ASIS appears to be positioned somewhat vertically over the pubic bone.
ANTERIOR AND POSTERIOR PELVIC TILTS (CONTINUED)
Gliding joint action
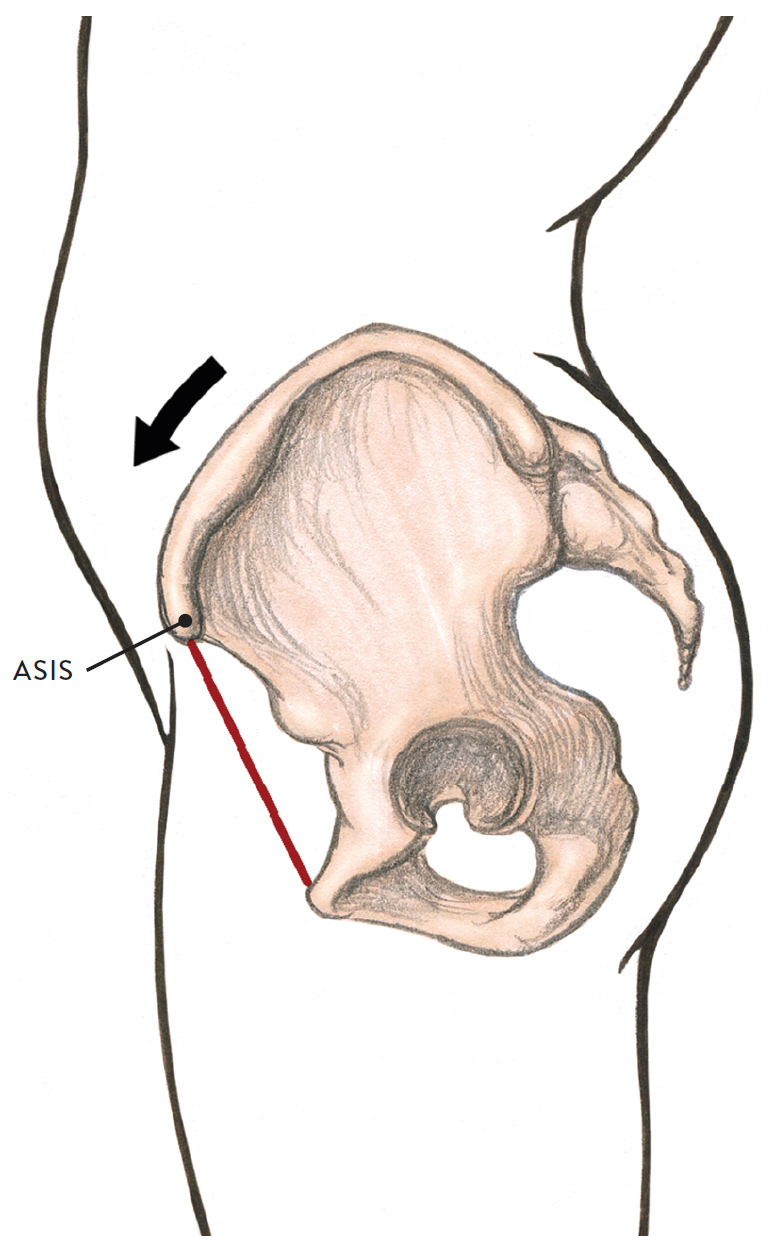
Anterior pelvic tilt (APT), lateral view
The upper part of the pelvis tilts in a forward and downward direction. Each ASIS is in a lower position than when the pelvis is in neutral position.
ANTERIOR AND POSTERIOR PELVIC TILTS (CONTINUED)
Gliding joint action
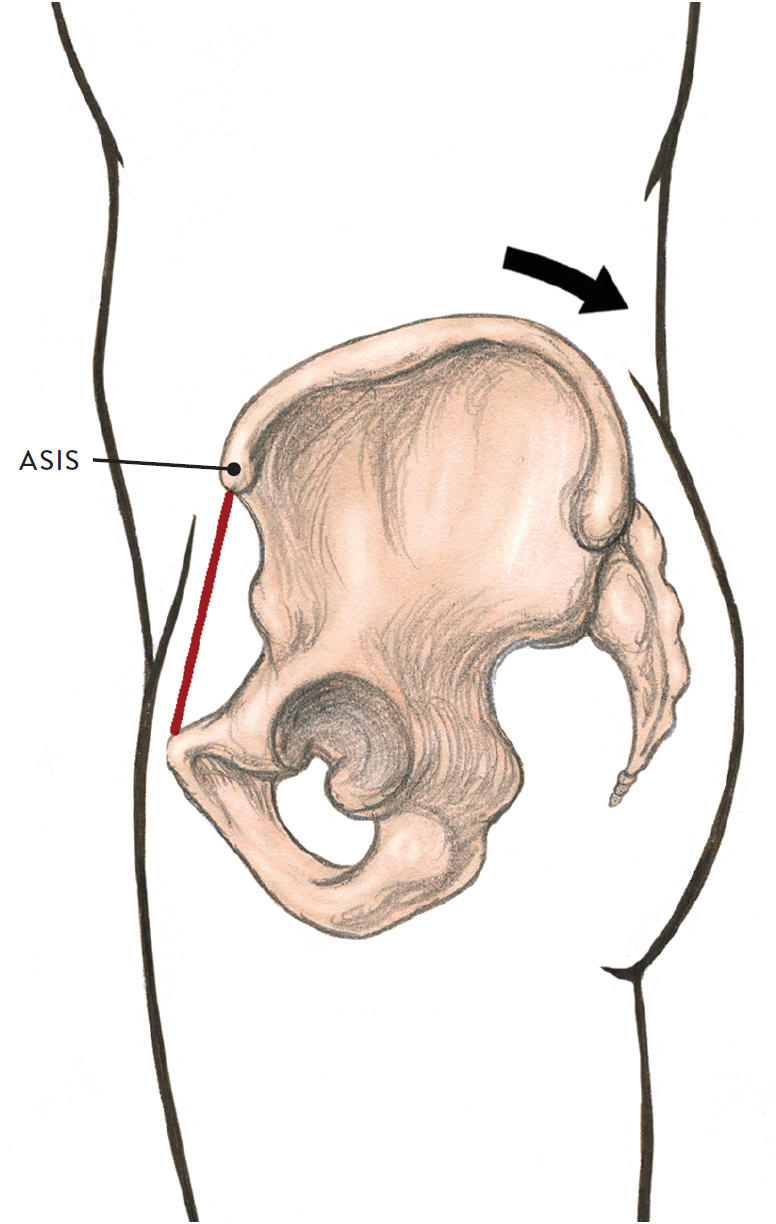
Posterior pelvic tilt (PPT), lateral view
The upper part of the pelvis tilts back. Eash ASIS is in a higher position than when the pelvis is in neutral position.
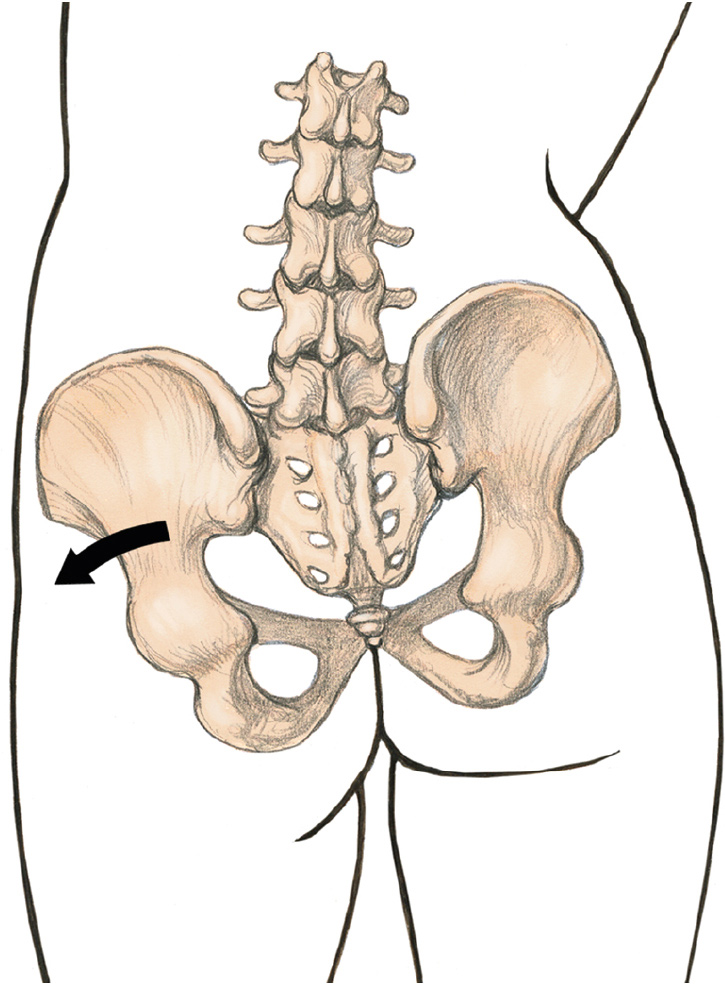
In the drawing Lateral Flexion of Pelvis at the Lumbosacral Joint, we see the pelvis tilting sideways. Lateral flexion is tilting the whole pelvis sideways, either toward the right (right lateral flexion) or left (left lateral flexion).
LATERAL FLEXION OF PELVIS AT THE LUMBOSACRAL JOINT
Gliding joint action
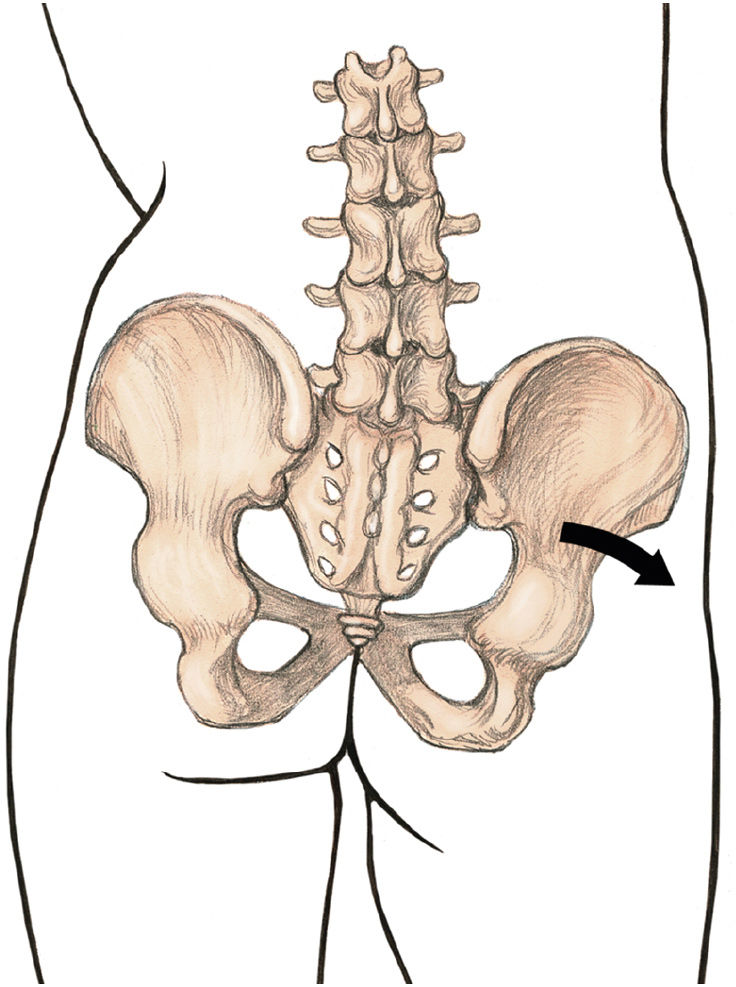
Right lateral flexion, posterior view
Pelvis tilts toward the right side.
LATERAL FLEXION OF PELVIS AT THE LUMBOSACRAL JOINT (CONTINUED)
Gliding joint action
Neutral position of pelvis, posterior view
LATERAL FLEXION OF PELVIS AT THE LUMBOSACRAL JOINT (CONTINUED)
Gliding joint action
Left lateral flexion, posterior view
Pelvis tilts toward the left side.
The drawing Rotation of Pelvis at the Lumbosacral Joint and Lumbar Vertebrae Joints, shows the action of swiveling the hips as the pelvis rotates toward the right and left.
ROTATION OF PELVIS AT THE LUMBOSACRAL JOINT AND LUMBAR VERTEBRAE JOINTS
Pivotal and gliding joint action
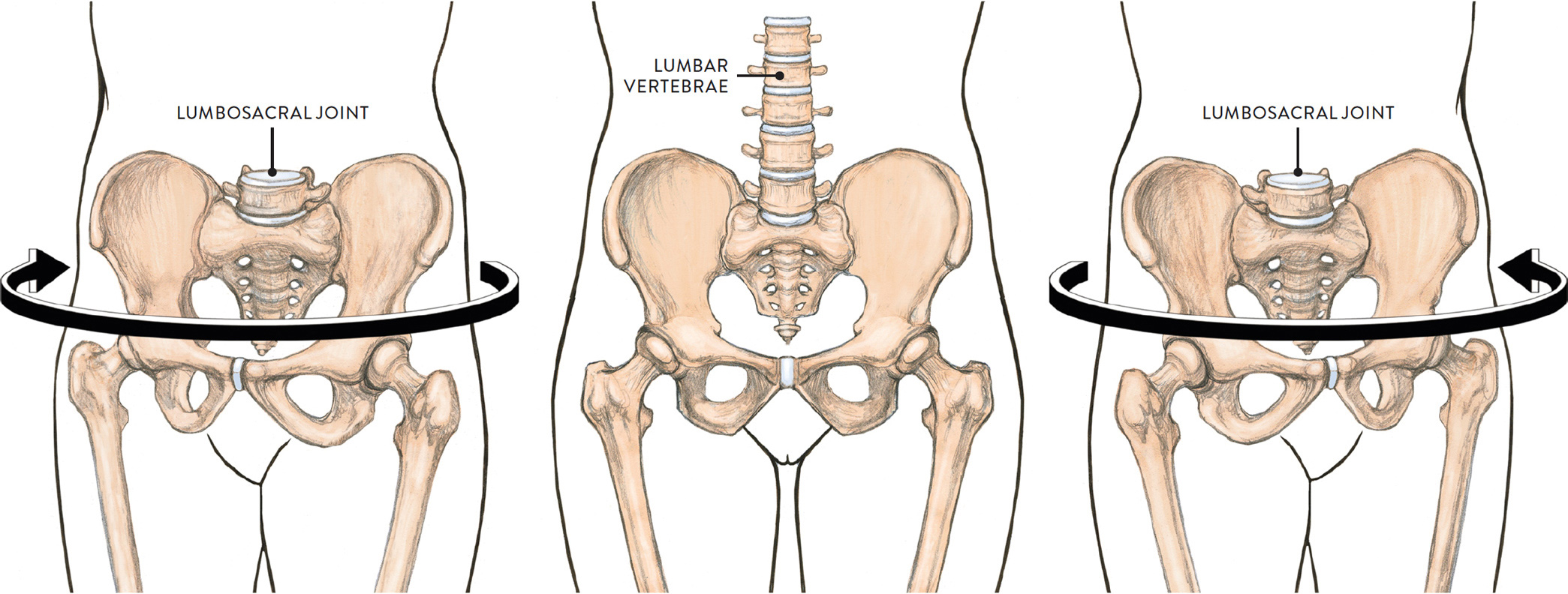
LEFT: Rotation of pelvis toward the right, anterior view
CENTER: Neutral position of pelvis, anterior view
RIGHT: Rotation of pelvis toward left, anterior view
Joints of the Upper Limb and Shoulder Girdle
The main joints of the upper limb are the shoulder joint, elbow joint, wrist joint, and joints of the hand (including finger joints and thumb joints). The drawing shows their locations, identifying the type of each joint.
MAIN JOINTS OF THE UPPER LIMB
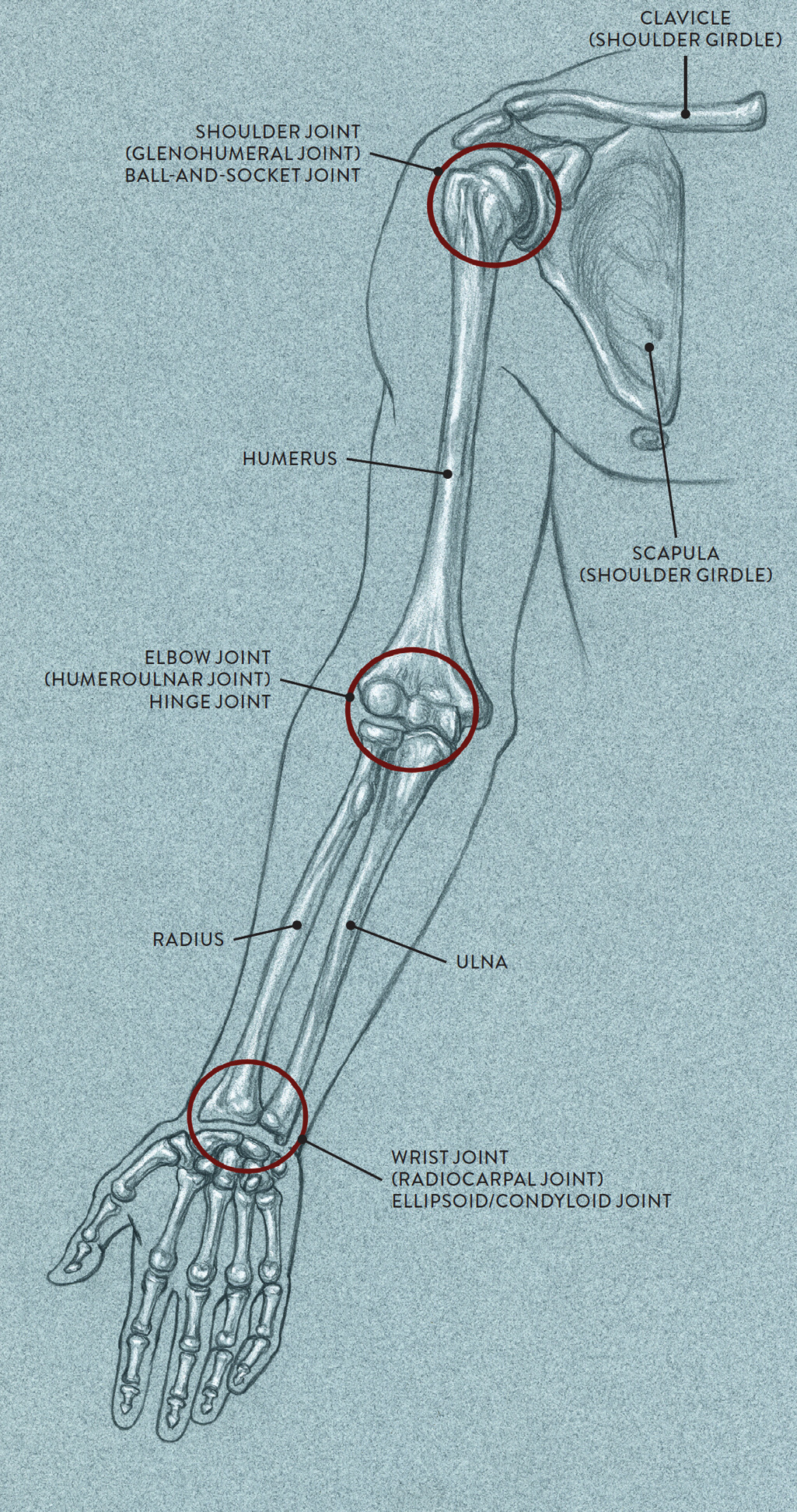
Anterior view of right arm in anatomical position
The shoulder girdle, or pectoral girdle, comprises the clavicles (collarbones) and the scapula bones (shoulder blades) and is the supportive framework to which the upper limbs connect. The shoulder girdle has three main joints: the scapulothoracic joint, sternoclavicular joint, and acromioclavicular joint. These joints and the associated bones are shown in the following drawing.
JOINTS OF THE SHOULDER GIRDLE
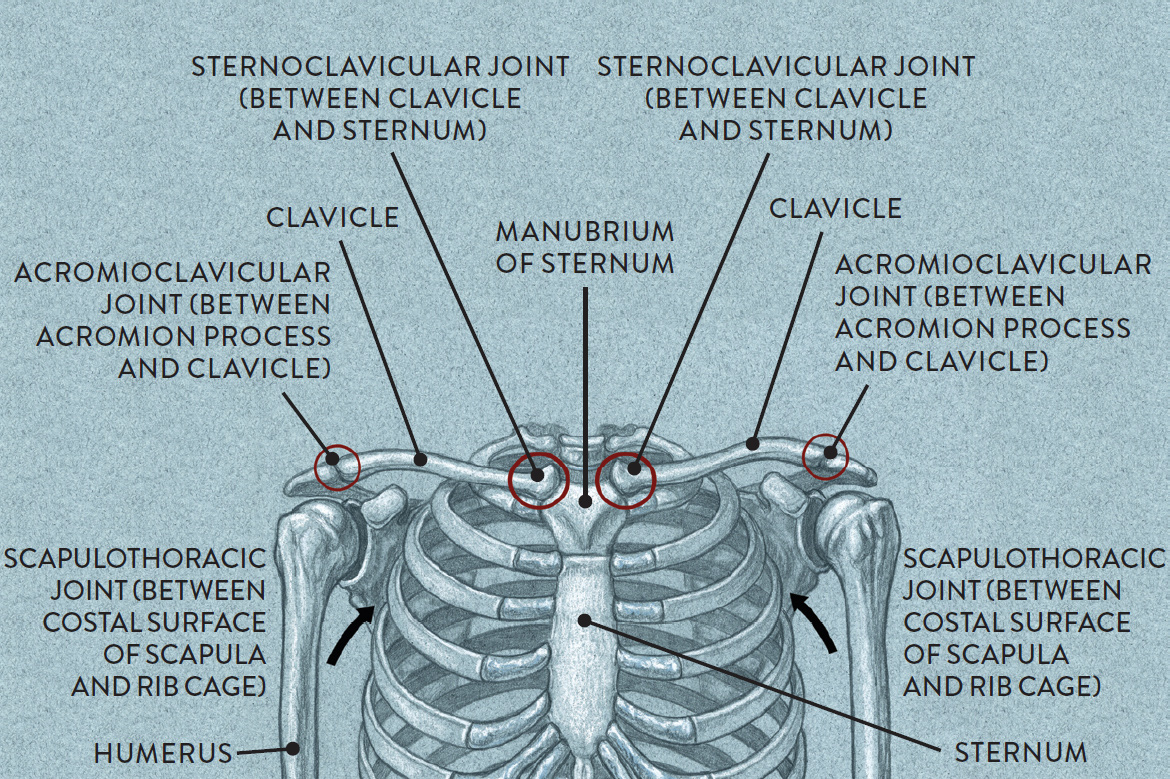
Rib cage and shoulder girdle, anterior view
The scapulothoracic joint (pron., SKAP-pah-low-thoh-RAS-ik) is the articulation between the scapula bone and the posterior portion of the thorax (rib cage). Anatomically, this is not a true joint, but it is considered a functional joint because of the way the scapula moves in relation to the rib cage.
Names of Shoulder-Girdle Joints
The names of shoulder-girdle joints provide clues to their location:
· Scapulo pertains to the scapula bone.
· Thoracic pertains to the thorax, or rib cage.
· Sterno pertains to the sternum.
· Clavicular pertains to the clavicle.
· Acromio pertains to the acromion process of the spine of the scapula.
Movements of the Scapula
It is very beneficial for artists to learn about the scapula bones and how they move. Several muscles attach into these bones, and when the various muscles contract, they move the scapula to slightly different positions on the back. This can noticeably change the topography of the back, with the bulges and valleys of the muscular forms changing from pose to pose. The best way to understand what is occurring on the back is to look for three basic skeletal structures: the rib cage, the vertebral column, and the position of the scapula bones. The presence of the scapula can most easily be detected at the scapula’s medial/vertebral border. You can quickly assess where the scapula bones are by observing the action of the arms, then looking for the medial border, which will enable you to see the approximate location of the scapula bones in that particular pose. From there you can locate the general muscular forms.
In the next drawing, Movements of the Scapula at the Scapulothoracic Joint, we see the many possible positions of the scapula. Since the humerus connects into the scapula, these two bones work as a team in movements of the upper arm. When the humerus moves to different positions, the scapula bone will also move, unless it is intentionally stabilized by certain muscles. The movements of the scapula, shown in the drawing include the following:
· Elevation of the scapula: The shoulders lift upward, as in the action of shrugging the shoulders.
· Depression of scapula: The scapula returns to its normal position or slightly lower, which occurs when lifting a heavy weight, such as a barbell.
· Adduction (or protraction) of the scapula: As the upper arm moves back, the scapula moves back toward the vertebral column. This action can be seen in the military stance of attention or when someone is “jabbing” his or her elbows.
· Abduction (or retraction) of the scapula: As the arm reaches forward, the scapula moves away from the vertebral column. This action can be seen when a person crosses both arms in front of the torso or is hunched over. It can also be seen when someone dynamically thrusts the arms forward when reaching for something.
· Downward rotation of the scapula: The scapula tilts, with the bottom tip (inferior angle) moving slightly inward while the acromion process moves downward. The bottom tip of the scapula can also lift slightly away from the rib cage, creating tension in this region. This action can be seen when someone reaches into a back trouser pocket.
· Upward rotation of the scapula: The scapula tilts, with the bottom tip moving slightly outward and the acromion process tilting upward. This action can be seen when the whole arm is lifted upward.
MOVEMENTS OF THE SCAPULA AT THE SCAPULOTHORACIC JOINT
Posterior view of the torso
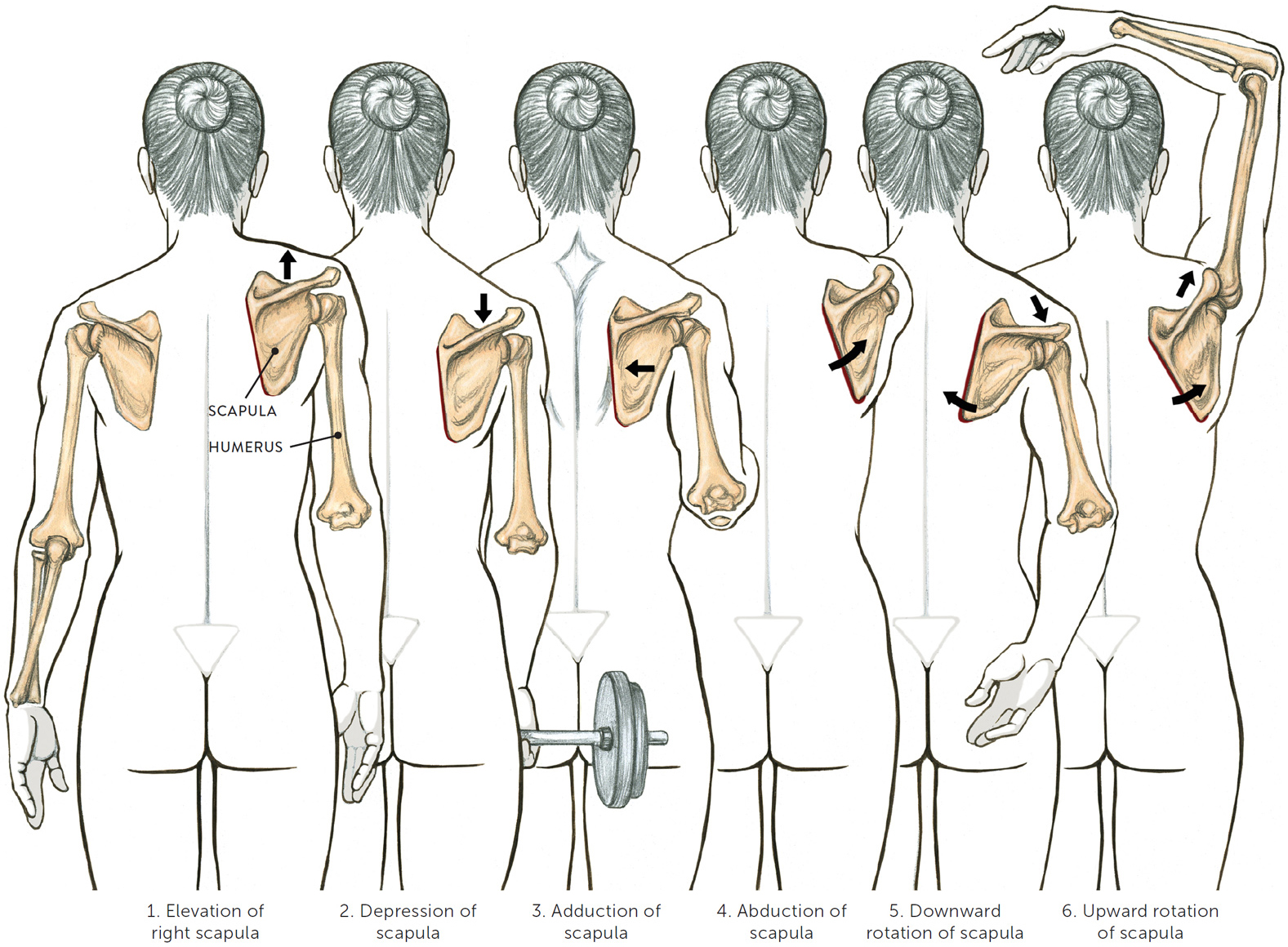
Left scapula and bones of arms are in normal position
ARROWS: Directional movements of the scapula
RED LINES: Medial/vertebral border of the scapula
The Joints of the Clavicle
Each clavicle (collarbone) attaches to two different bones—the sternum and the acromion process of the scapula (the outer end of the spine of the scapula)—thus creating two separate clavicular joints: the sternoclavicular joint and the acromioclavicular joint. The clavicle, scapula, and humerus (which attaches into the scapula) are all interconnected, so if one bone moves, the other bones usually move as well.
The sternoclavicular joint (pron., STER-no-cla-VICK-yoo-lar), or SC joint, is the joint between the inner end of the clavicle and the upper portion (manubrium) of the sternum (breastbone). It is usually classified as a gliding/plane joint, but some experts consider it a saddle joint. Movements at the SC joint are elevation and depression of the clavicle and protraction and retraction of the clavicle.
The acromioclavicular joint (pron., ah-CROW-mee-oh-cla-VICK-yoo-lar), or AC joint, is the joint between the outer end of the clavicle and the acromion process of the scapula. It, too, is a gliding/plane joint. Movements at the AC joint are upward and downward rotation of the clavicles and scapula.
To keep things simple, only the clavicles and the sternum are shown in each of the movements depicted in the drawing Movements of Clavicle at the Sternoclavicular (SC) and Acromioclavicular (AC) Joints, below. Remember, however, that when the clavicle moves, the scapula and humerus move, as well. (Note that downward rotation of the clavicle is not shown in the drawing.)
MOVEMENTS OF CLAVICLE AT THE STERNOCLAVICULAR (SC) AND ACROMIOCLAVICULAR (AC) JOINTS
Gliding joint actions, anterior view of the torso
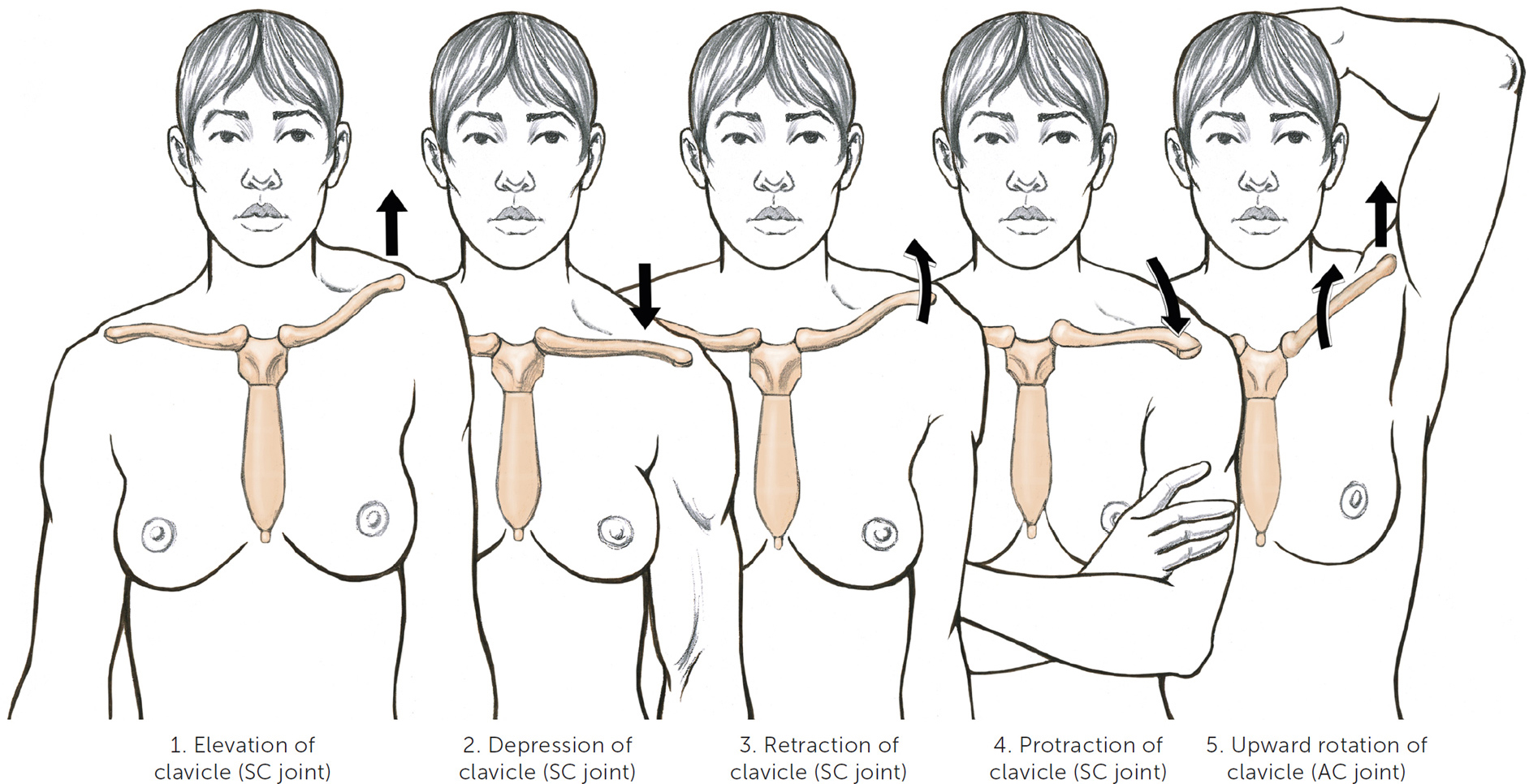
ARROWS: Directional movements of the clavicle
The movements of the clavicle include the following:
· Elevation of the clavicle (at the SC joint): The shoulders are shrugged or one shoulder is lifted higher than the other.
· Depression of the clavicle (at the SC joint): The shoulder returns to its normal position from an elevated position, or the outer end of the clavicle drops even lower, as when a person is holding a heavy weight, such as a barbell.
· Retraction of the clavicle (at the SC joint): The shoulders are thrown back, as in the military stance of attention.
· Protraction of the clavicle (at the SC joint): The shoulders roll forward, as when hunching over or folding the arms in front of the torso.
· Upward rotation of the clavicle (at the AC joint): The upper arm (humerus) is lifted up over the head as in the action of abduction, producing an upward rotation of the scapula that results in the outer end of the clavicle lifting upward and slightly rotating (posterior rotation).
(Note that the clavicle appears to be performing the same upward-tilting action in both the elevation of the clavicle and the upward rotation of the clavicle. The difference is that when the clavicle elevates—as when shrugging the shoulders—the scapula also elevates, with both bones moving in an upward direction, although the inner end of the clavicle at the SC joint remains fixed. In the movement of upward rotation of the clavicle, however, the scapula tilts while the clavicle elevates and rotates.)
The Shoulder Joint
The shoulder joint, known anatomically as the glenohumeral joint (pron., GLEN-o-HYOO-mer-al or GLEE-no-HYOOM-er-al) is the articulation between the head of the humerus (upper arm) and a small, shallow socket on the scapula called the glenoid fossa. This joint, shown in the drawing below, cannot be seen on the surface because it is covered by layers of cartilage, ligaments, and muscles. A ball-and-socket joint, it produces a wide range of movements of the humerus bone, including flexion and extension, abduction and adduction, medial and lateral rotation, and circumduction of the humerus.
SHOULDER (GLENOHUMERAL) JOINT
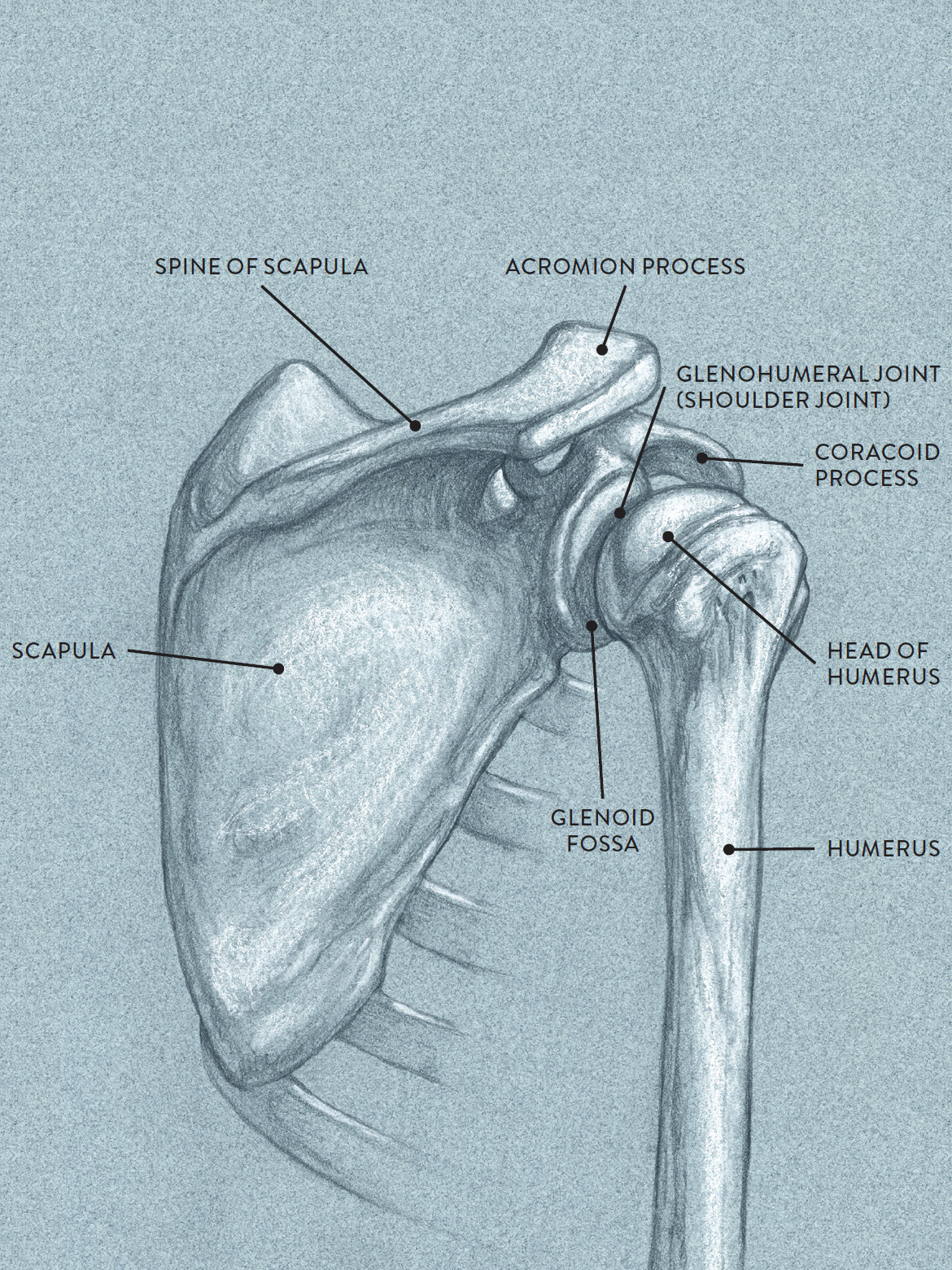
Posterior lateral view of right scapula and humerus bone
The drawing Flexion and Extension of Humerus at Shoulder Joint, shows the humerus performing a forward-and-back movement. Flexion is the action of moving the humerus in a forward direction and can continue until the whole arm is above the head. Extension is the reverse of this action, in which the humerus is returned to its neutral position at the side of the torso. A continuing movement of the humerus toward the back is sometimes referred as hyperextension of the humerus.
FLEXION AND EXTENSION OF HUMERUS AT SHOULDER JOINT
Ball-and-socket joint action
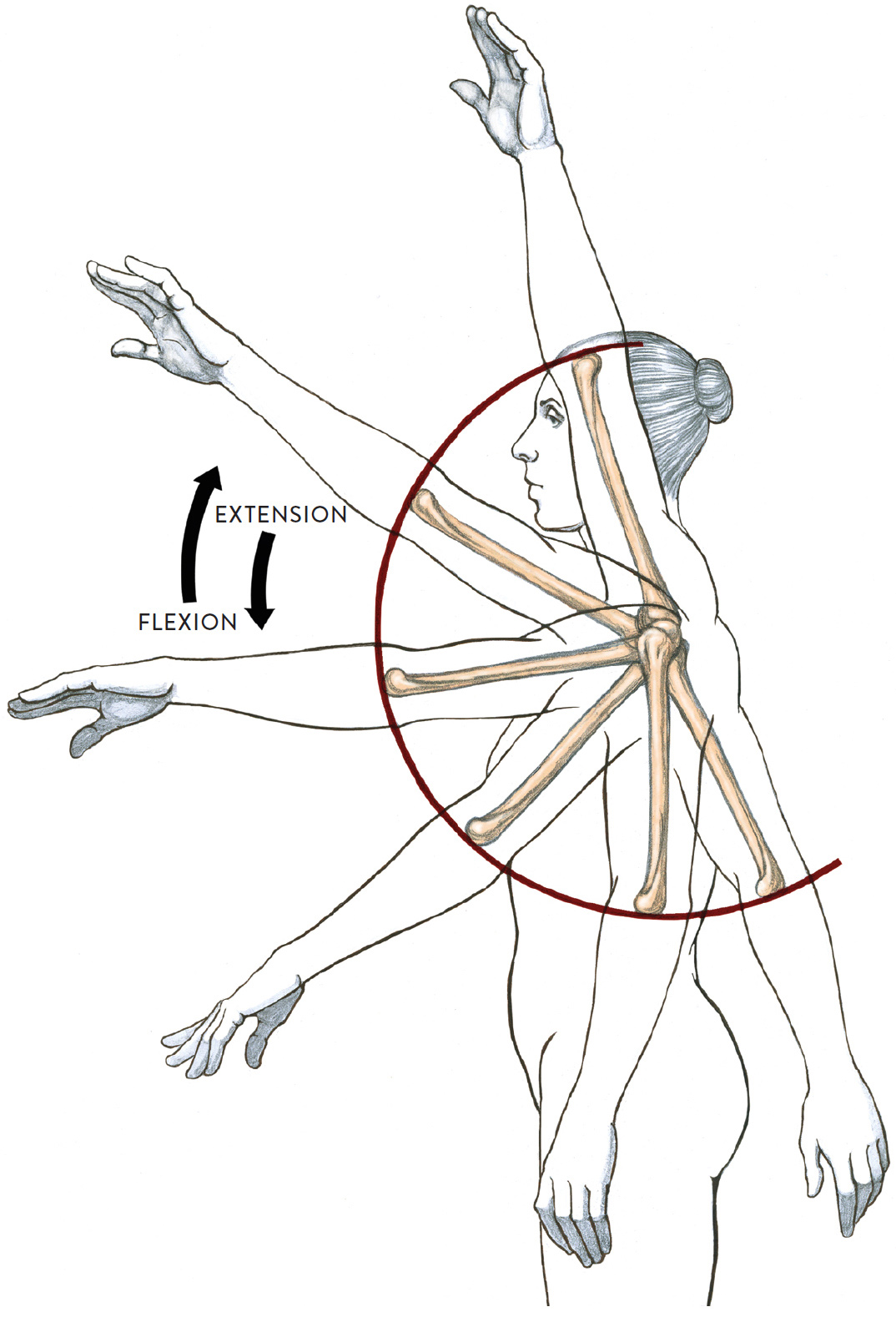
Lateral view of torso and left arm
MAROON HALF-CIRCLE: Arclike directional movement of the humerus bone as it swings upward or downward
In the drawing Abduction and Adduction of Humerus at Shoulder Joint,, we see the humerus moving sideways away from the torso. Abduction is the action of moving the humerus away from the side of the body and can continue upward until the whole arm is above the head. Adduction is the return of the humerus back to the side of the torso. Adduction of the humerus can continue farther, as when the upper arm is moved across the chest.
ABDUCTION AND ADDUCTION OF HUMERUS AT SHOULDER JOINT
Ball-and-socket joint action
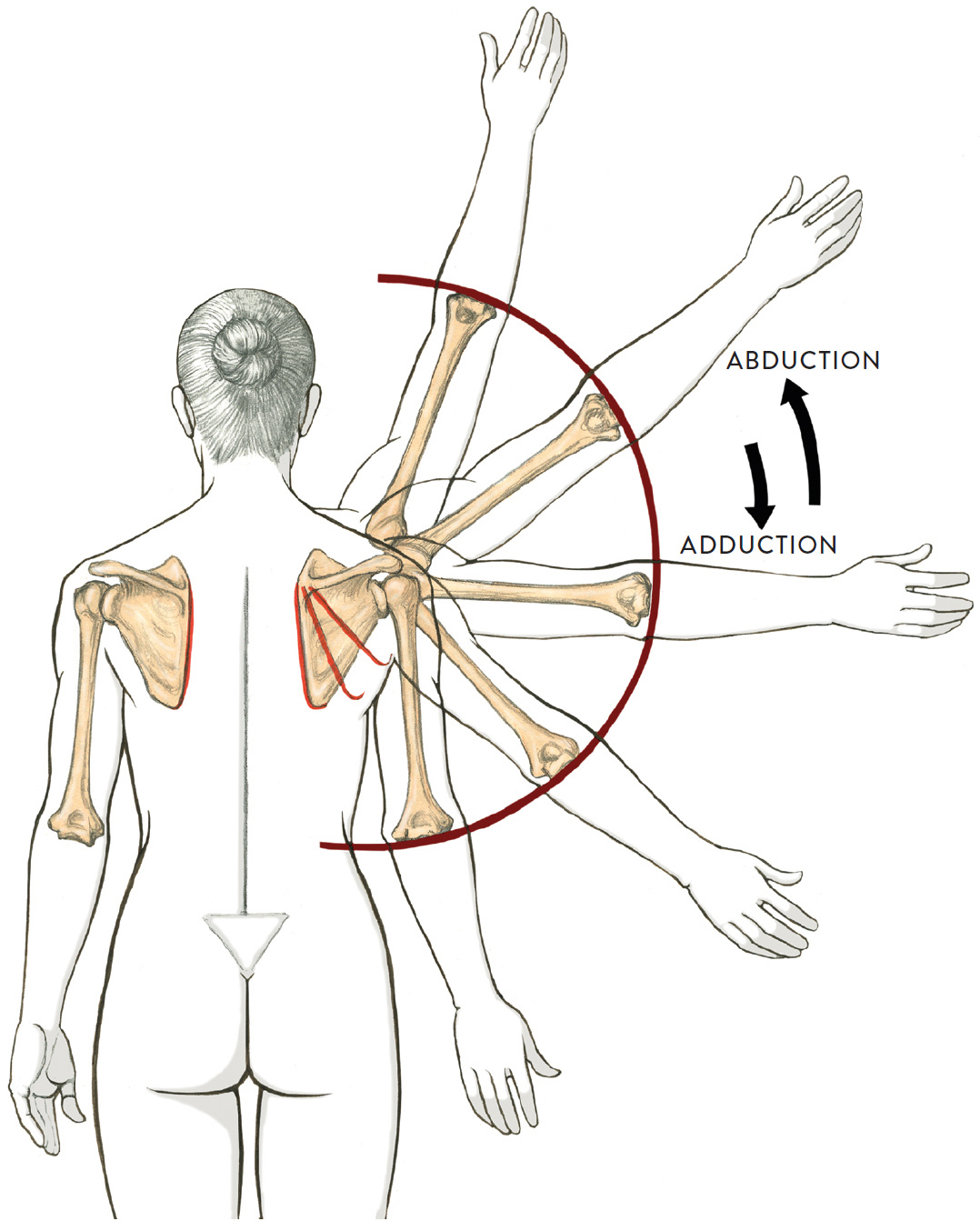
Posterior view
RED LINES: Medial border of the scapula, showing how it changes position as the humerus moves
MAROON HALF-CIRCLE: Arclike directional movement of humerus bone as it swings upward or downward
Next, in the drawing Lateral and Medial Rotation of Humerus at Shoulder Joint, we see the humerus pivoting on its own axis. When the humerus rotates in an outward direction, the action is called lateral rotation because the bone is turning away from the midline of the body. When the humerus rotates in an inward direction, this action is called medial rotation because it is turning toward the midline of the body.
LATERAL AND MEDIAL ROTATION OF HUMERUS AT SHOULDER JOINT
Ball-and-socket joint action
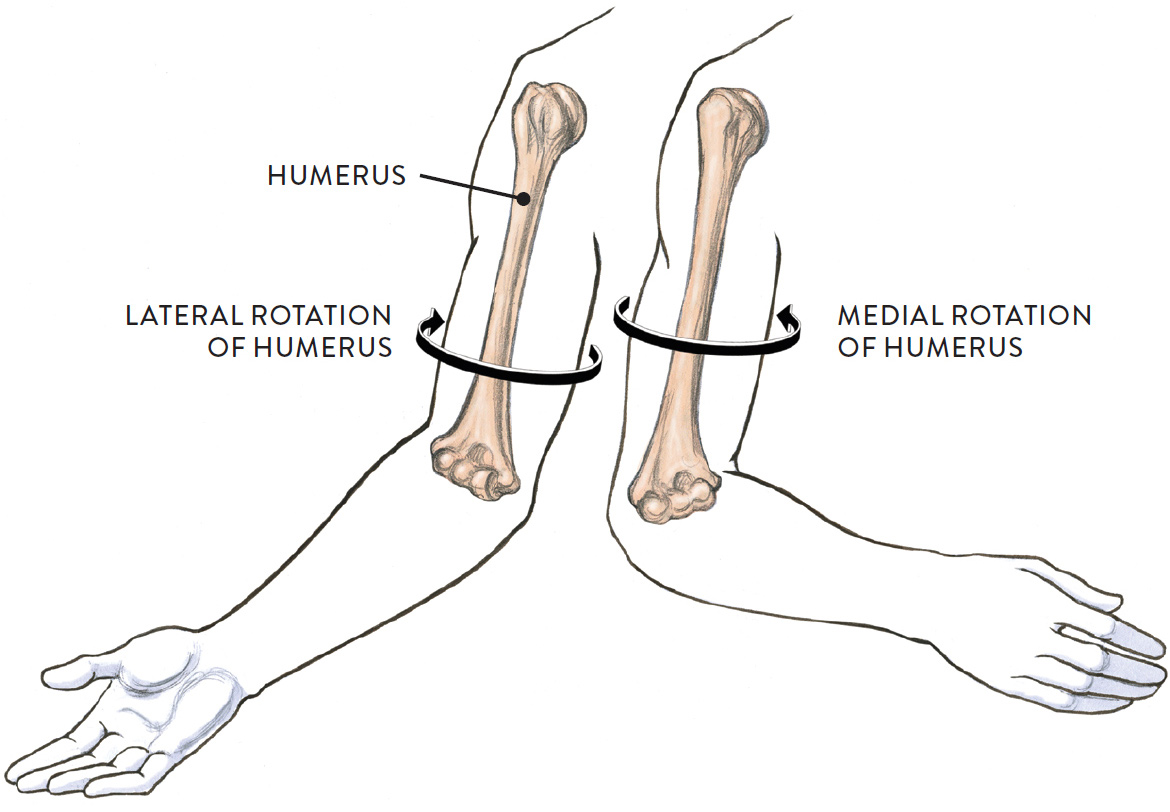
Anterior view of the right upper limb
Finally, in the drawing Circumduction of Humerus at Shoulder Joint, we see the circular movement of the humerus. This movement is often confused with the rotation of the humerus, but the difference is that, in circumduction, the whole humerus (or upper arm) is moving in a circular motion while the head of the humerus at the shoulder joint remains somewhat stabilized. The movement is essentially “drawing a circle” with the hand (with both the upper and lower arm involved) or with the elbow (with the circular movement restricted to the upper arm). Circumduction circles can be broad or narrow and can be executed in a clockwise or counterclockwise direction.
CIRCUMDUCTION OF HUMERUS AT SHOULDER JOINT
Ball-and-socket joint action
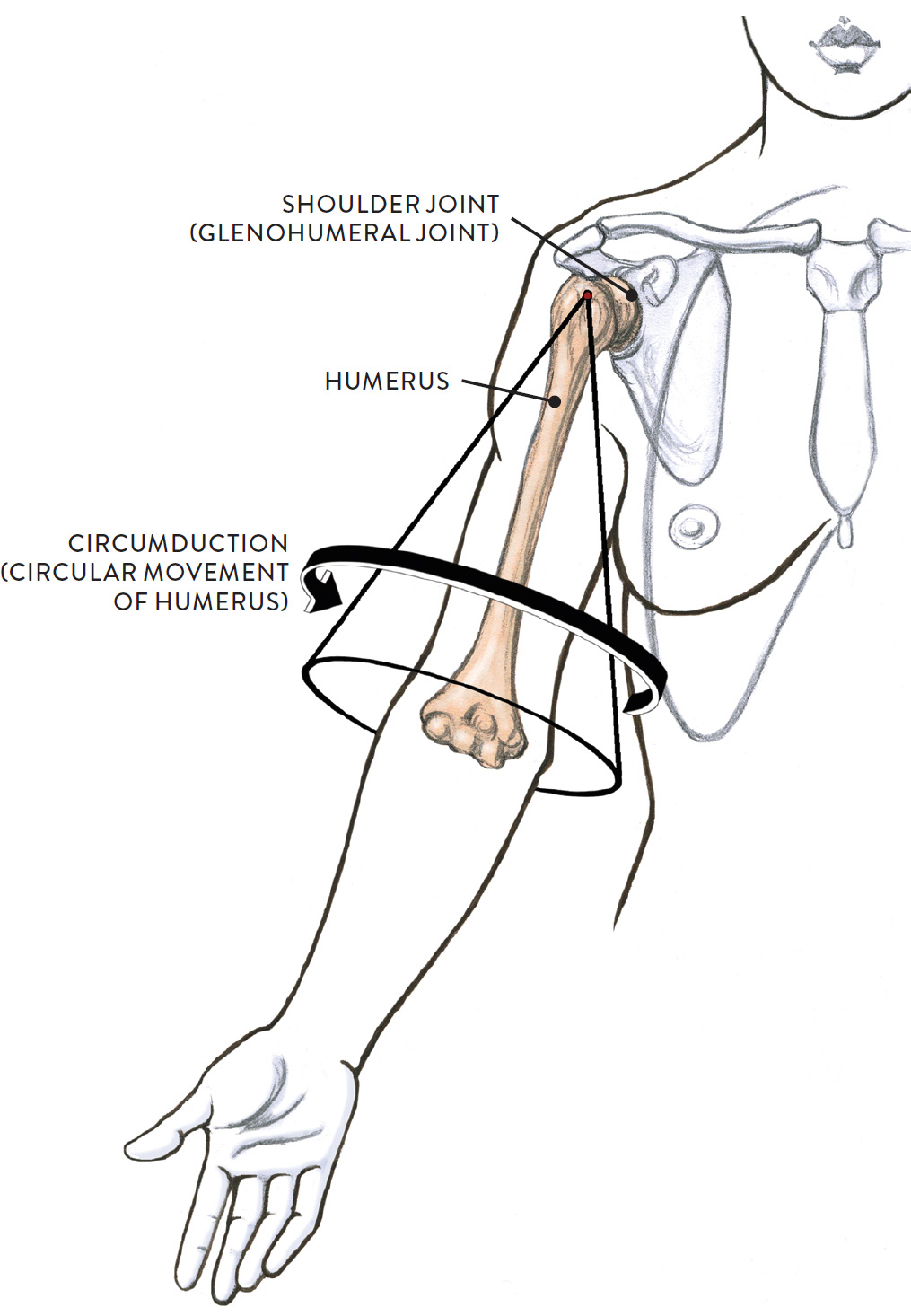
Anterior view of right arm and partial torso
The Elbow Joint
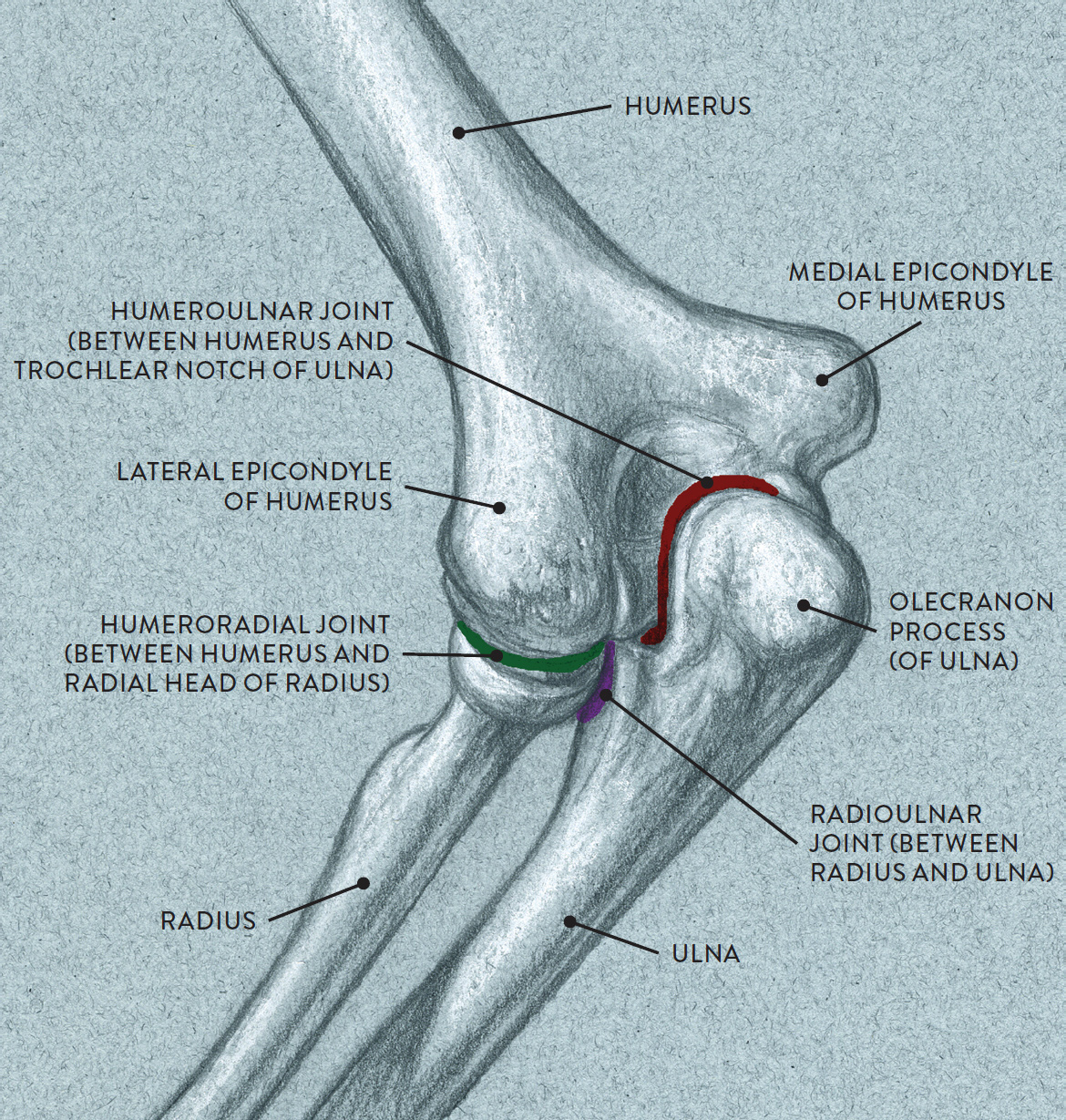
The elbow joint actually consists of three joints: the humeroulnar joint, the humeroradial joint, and the proximal radioulnar joint. Although the functions of these three joints are separate, they share the same joint capsule and are grouped together anatomically as a single joint complex.
ELBOW JOINT
Posterior three-quarter view of left arm
Names of Elbow-Complex Joints
The names of elbow-complex joints provide clues to their location:
· Humero pertains to the humerus bone.
· Radial or radio pertains to the radius bone.
· Ulnar pertains to the ulna bone.
· Proximal refers to the area closest to the body part’s point of attachment.
· Distal refers to the area farthest from the body part’s point of attachment.
The humeroulnar joint (pron., HYOO-mer-o-ULL-nar) occurs between the humerus of the upper arm and the ulna of the lower arm. At the base of the humerus is a smooth surface called the trochlea of the humerus, shaped somewhat like a horizontally positioned sewing spool. At the upper part of the ulna, a bony surface called the trochlear notch of the ulna is shaped like a crescent wrench. The crescent-wrench shape of the ulna fits around the spool-like shape of the humerus.
In the drawing Flexion and Extension of Lower Arm at Elbow Joint, we see that the articulation between the humerus and ulna is a hinge joint that produces a back and forth movement of the ulna bone. Flexion is when the lower arm moves toward the upper arm; extension is the straightening of the lower arm.
FLEXION AND EXTENSION OF LOWER ARM AT ELBOW JOINT
Hinge joint action
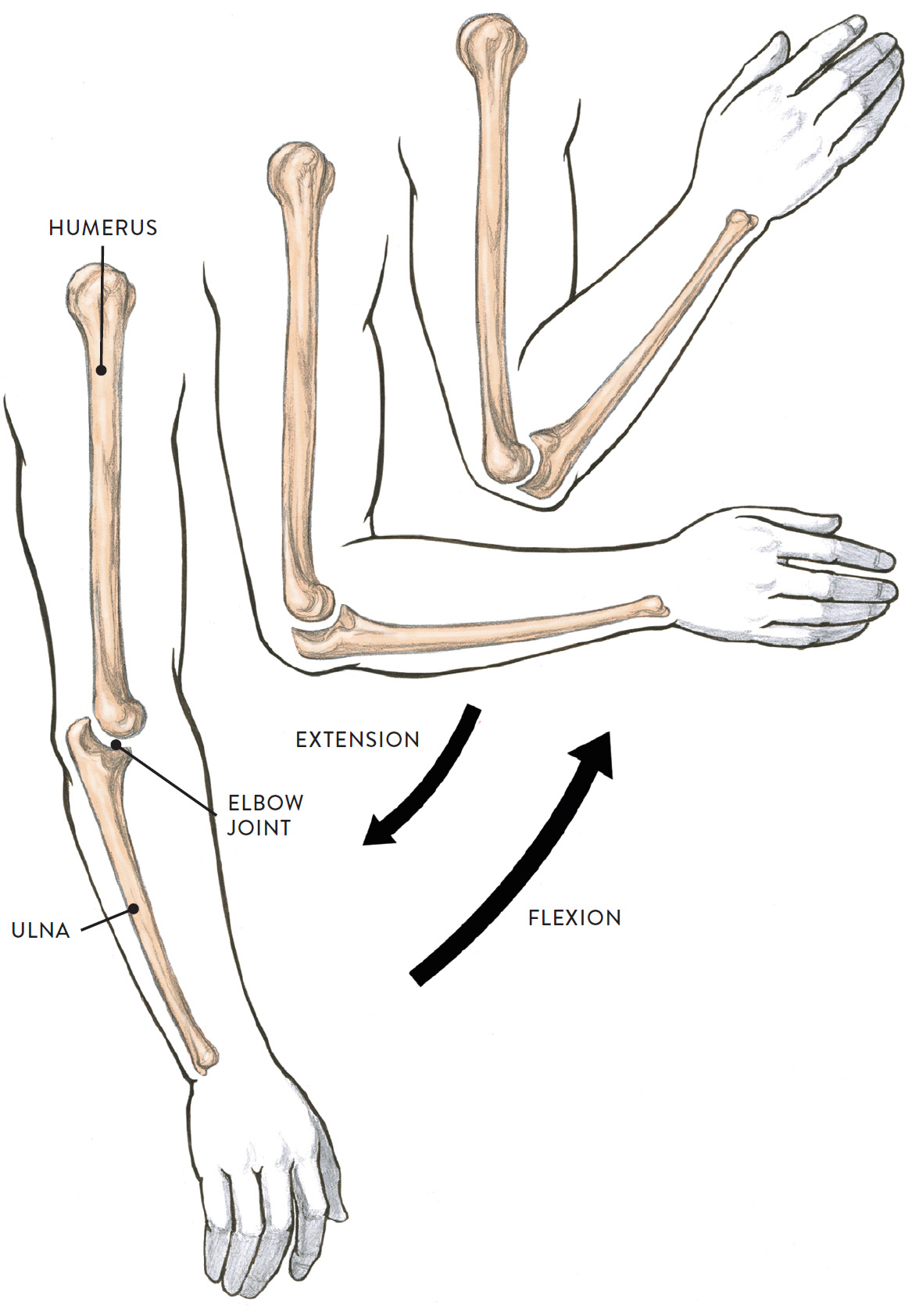
Lateral view of upper and lower right arm (radius bone of lower arm not shown)
The humeroradial joint (pron., HYOO-mer-oh-RAY-dee-ul) is located between the lower portion of the humerus and the upper portion of the radius bone. At the base of the humerus, positioned next to the trochlea of the humerus, is a spherical form called the capitulum of the humerus. At the upper part of the radius is a small wheel-shaped structure called the head of the radius (or radial head). The top surface of the radial head is slightly concave, and this is where it articulates with the round capitulum. The humeroradial joint is classified as a pivot joint and passively participates in the rotational movements of supination and pronation of the lower arm. This joint does not participate in the hinge movement of the elbow.
The proximal radioulnar joint (pron., PROCKS-sih-mal RAY-dee-oh-ULL-nar) occurs between the head of the radius and a small indentation on the ulna called the radial notch. A small ligament band (annular ligament) attaches from the ulna and encircles the neck and head of the radius bone, acting like a supportive strap keeping the head of the radius in place as it swivels or rotates. The proximal radioulnar joint is anatomically considered part of the elbow joint since it shares the same joint capsule, but the function of this joint is distinct from that of the elbow joint.
The drawing Supination and Pronation of Lower Arm and Hand at Elbow Joint Region, shows rotational movements occurring at the elbow joint and wrist. The humeroradial and proximal radioulnar joints are both pivot joints, and both participate in the actions of supination and pronation. When the lower arm is in the anatomical position, the two bones (radius and ulna) are parallel. Pronation is the rotational movement of the lower arm in which the radius bone pivots or swivels over the relatively stationary ulna bone. When it does this, the hand flips from facing upward or toward the front to facing downward or toward the back. Supination is the reverse of this action, moving the radius back to a position parallel to the ulna. The pivot movement actually takes place on both ends of the radius and ulna bones—at the proximal radioulnar joint, located in the upper region of the radius and ulna bones (and assisted by the humeroradial joint), as well as at the distal radioulnar joint, which is located at the lower region of the radius and ulna bones. (The distal radioulnar joint shares the joint capsule of the wrist joint and is considered by some experts to be part of the wrist joint.)
SUPINATION AND PRONATION OF LOWER ARM AND HAND AT ELBOW JOINT REGION
Pivot joint action
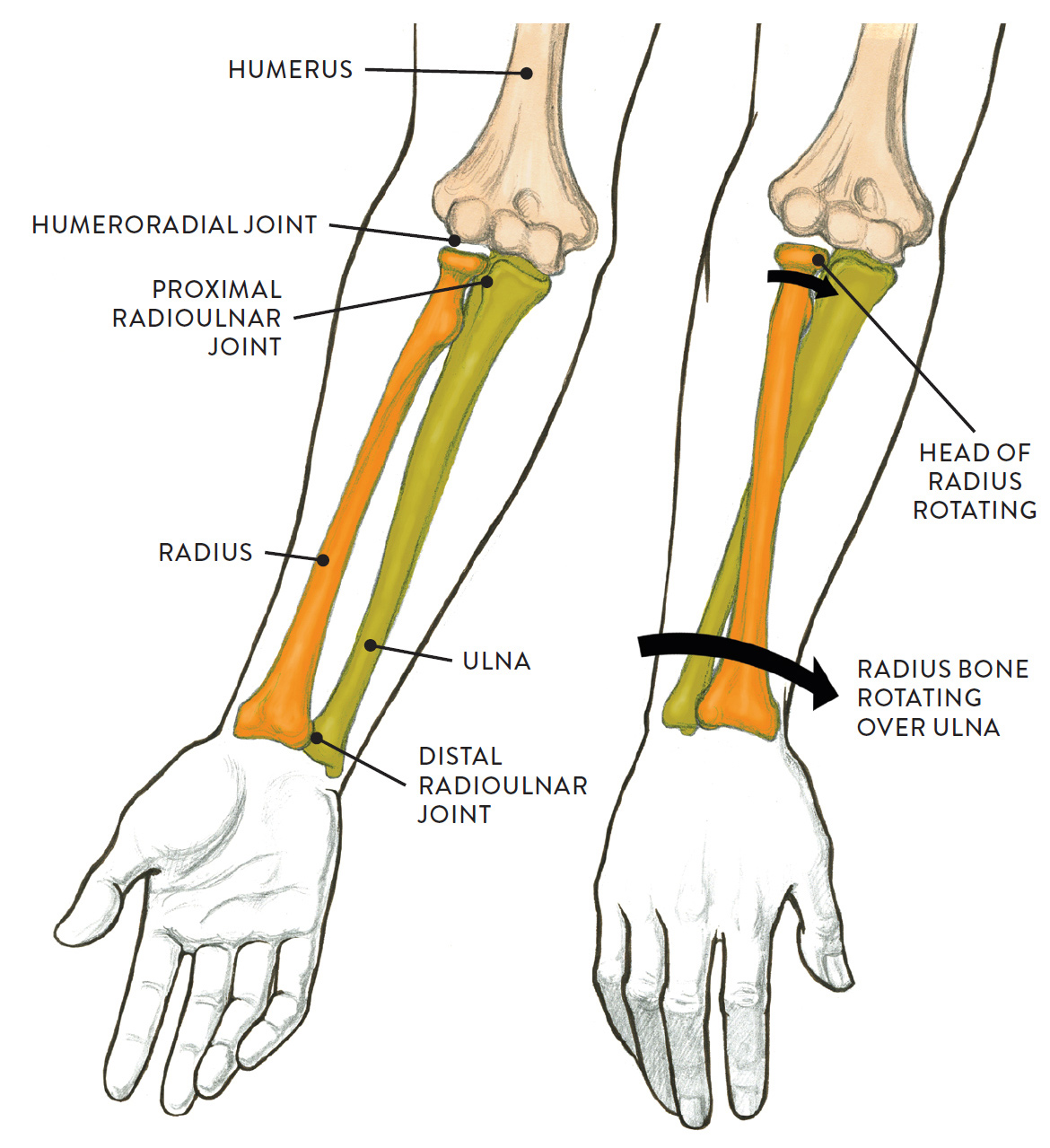
LEFT: Supination
Palm faces toward the front (right arm in anatomical position).
RIGHT: Pronation
Palm faces toward the back (right arm in anatomical position, pronating).
The Joints of the Wrist Region
At the wrist region are three main joints or groups of joints: the intercarpal joints, the midcarpal joint, and the radiocarpal joint. Of the three, only the radiocarpal joint is (somewhat) detectable on the surface, because it is the transitional region between the lower arm and the hand. It is the main joint involved in the movements of bending the hand at the wrist in different directions.
JOINTS OF WRIST REGION
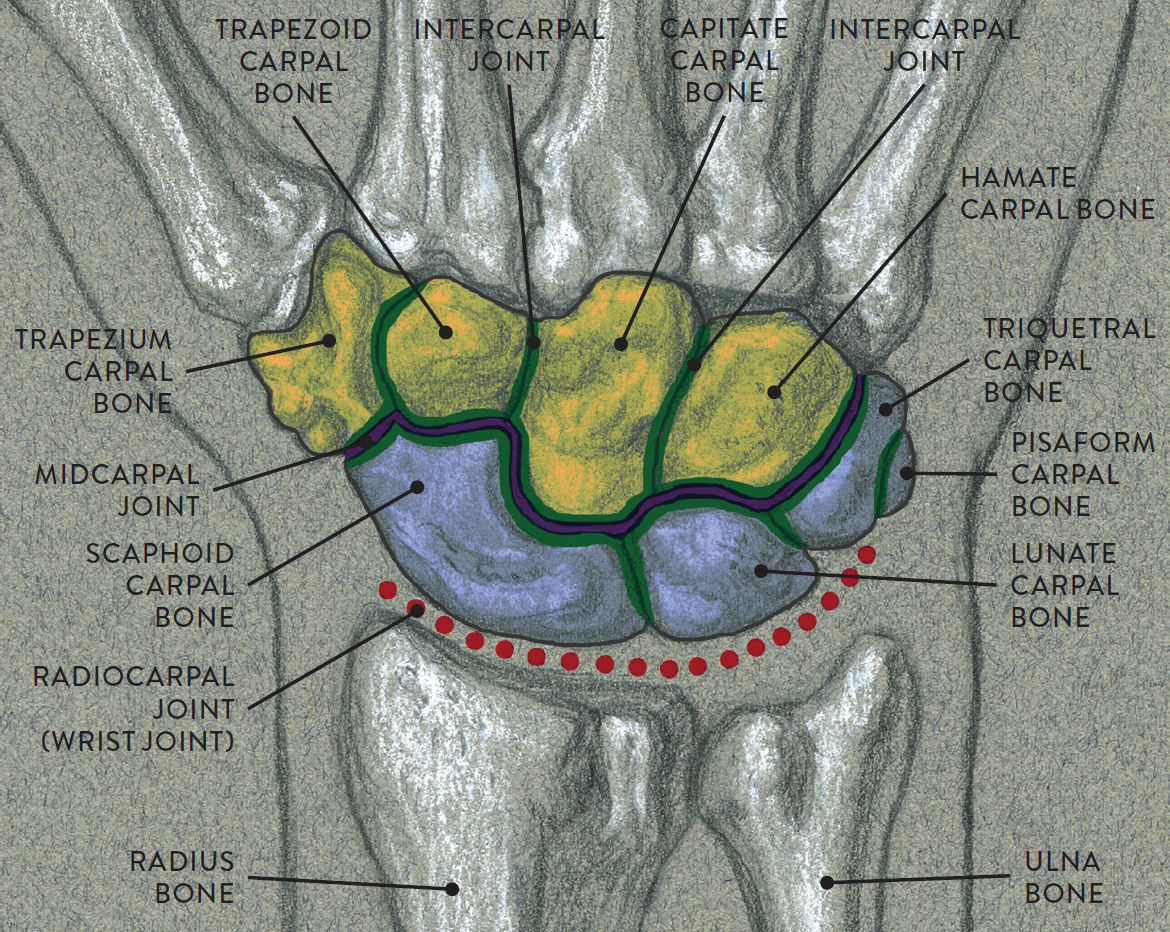
Wrist region of right hand, dorsal surface
GREEN LINES: Intercarpal joints (joints between all the carpal bones)
DARK PURPLE LINE: Midcarpal joint (joint between the proximal and distal rows of carpal bones)
DOTTED RED LINE: Radiocarpal joint (between the radius bone and the scaphoid, lunate, and triquetral carpal bones)
LIGHT PURPLE AREA: Proximal row of carpal bones
YELLOW AREA: Distal row of carpal bones
The intercarpal joints, also known as carpal joints, are the joints between the eight carpal bones. The midcarpal joint is the joint between the proximal and distal rows of carpal bones. Gliding and slight rotational movements occur between the carpal bones during the movements of flexion, extension, abduction, and adduction of the hand at the wrist joint.
The radiocarpal joint (pron., RAY-dee-o-KAR-poll), also known as the wrist joint, is between the lower end of the radius bone of the lower arm and three of the carpal bones (scaphoid, lunate, and triquetral) of the wrist. These three carpal bones are positioned side by side in a convex alignment that articulates with the concave surface of the end of the radius bone. Because of the overall shape of the articulating surfaces, the radiocarpal joint is classified as an ellipsoid/condyloid joint and is capable of moving the hand at the wrist in many ways, including flexion and extension, abduction adduction, and circumduction (the circular movement of the hand at the wrist).
Movements of the wrist joint include flexion and extension (moving the hand up and down from the wrist) and radial abduction and ulnar adduction (side-to-side movements of hand at the wrist). (The wrist can also perform a circular action called circumduction, but this is not shown in the drawings.)
In the drawing Flexion and Extension of Hand at the Wrist Joint, below, we see the downward and upward movement of the hand from the wrist. Flexion is the action of bending the palm side of the hand toward the anterior region of the lower arm, no matter what position the lower arm is in. Extension is the reverse of this action, returning the hand to its neutral position. Extension can go farther, bending the dorsal part of the hand toward the posterior side of the lower arm, no matter what position the lower arm is in. This action of bending the back of the hand from the wrist is also known as hyperextension.
FLEXION AND EXTENSION OF HAND AT THE WRIST JOINT
Ellipsoid/condyloid joint actions
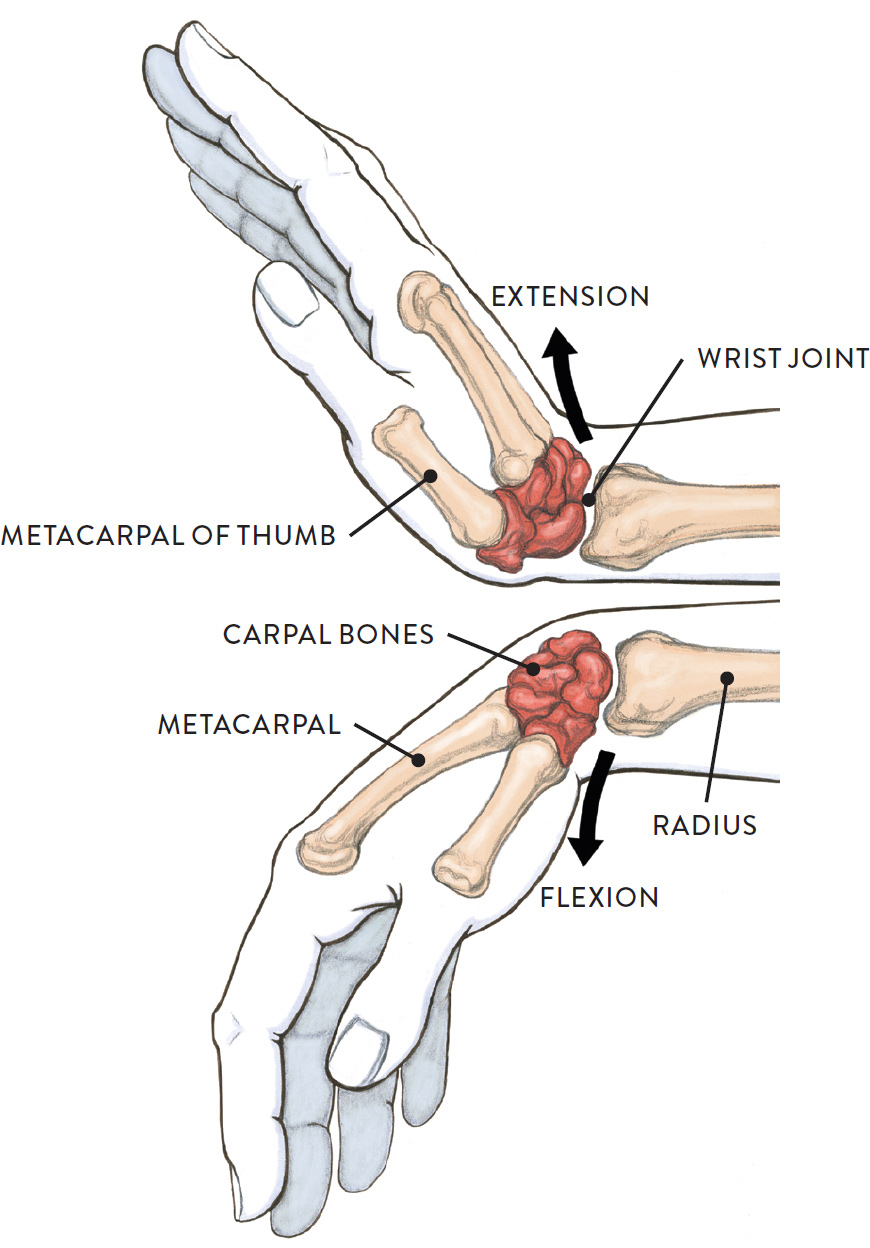
Lateral view of right hand
In the drawing Ulnar Adduction and Radial Abduction of Hand at the Wrist Joint, we see the movement of tilting the hand sideways from the wrist. Ulnar adduction (also called ulnar deviation) is the sideways tilting of the hand on the side of the lower arm containing the ulna bone. Radial abduction (radial deviation) is the sideways tilting of the hand on the side of the lower arm containing the radius bone; this movement is limited by the radial styloid process (a small projection of bone on the radius), which comes into close contact with the scaphoid carpal bone.
ULNAR ADDUCTION AND RADIAL ABDUCTION OF HAND AT THE WRIST JOINT
Ellipsoid/condyloid joint actions, palmar view of the right hand
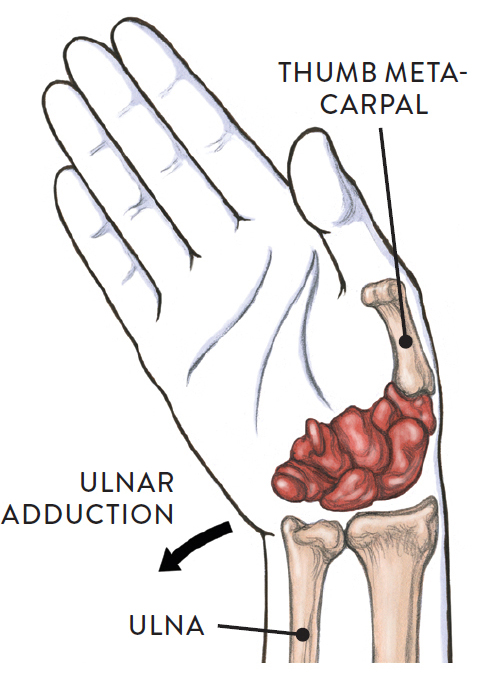
Ulnar adduction (ulnar deviation)
Hand tilts sideways over ulna.
ULNAR ADDUCTION AND RADIAL ABDUCTION OF HAND AT THE WRIST JOINT (CONTINUED)
Ellipsoid/condyloid joint actions, palmar view of the right hand
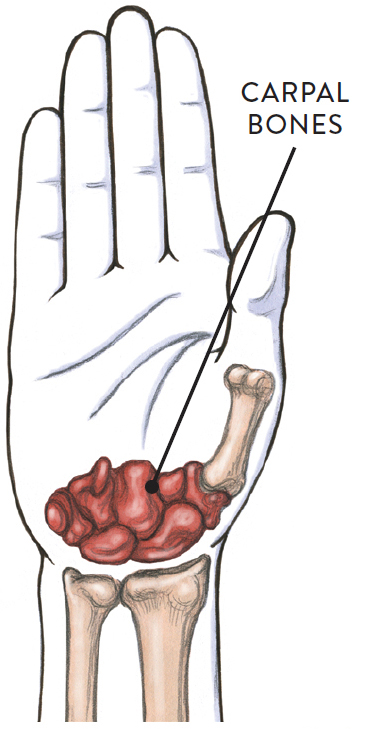
Neutral position of hand
ULNAR ADDUCTION AND RADIAL ABDUCTION OF HAND AT THE WRIST JOINT (CONTINUED)
Ellipsoid/condyloid joint actions, palmar view of the right hand
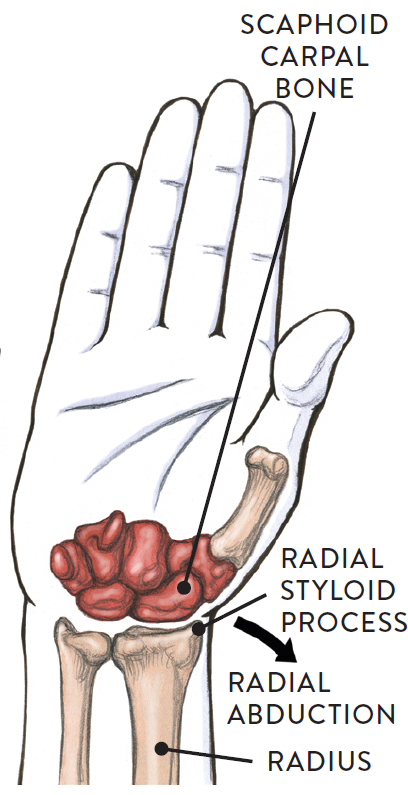
Radial abduction (radial deviation)
Hand tilts sideways over radius.
The Joints of the Hand
The bones of the hand comprise eight carpal bones at the wrist, five metacarpal bones, and fourteen phalanges (twelve finger bones and two thumb bones). Joints between the bones, shown in the next drawing, include the carpometacarpal joints (CMC joints), metacarpophalangeal joints (MCP joints), and interphalangeal joints (IP joints).
JOINTS OF THE HAND
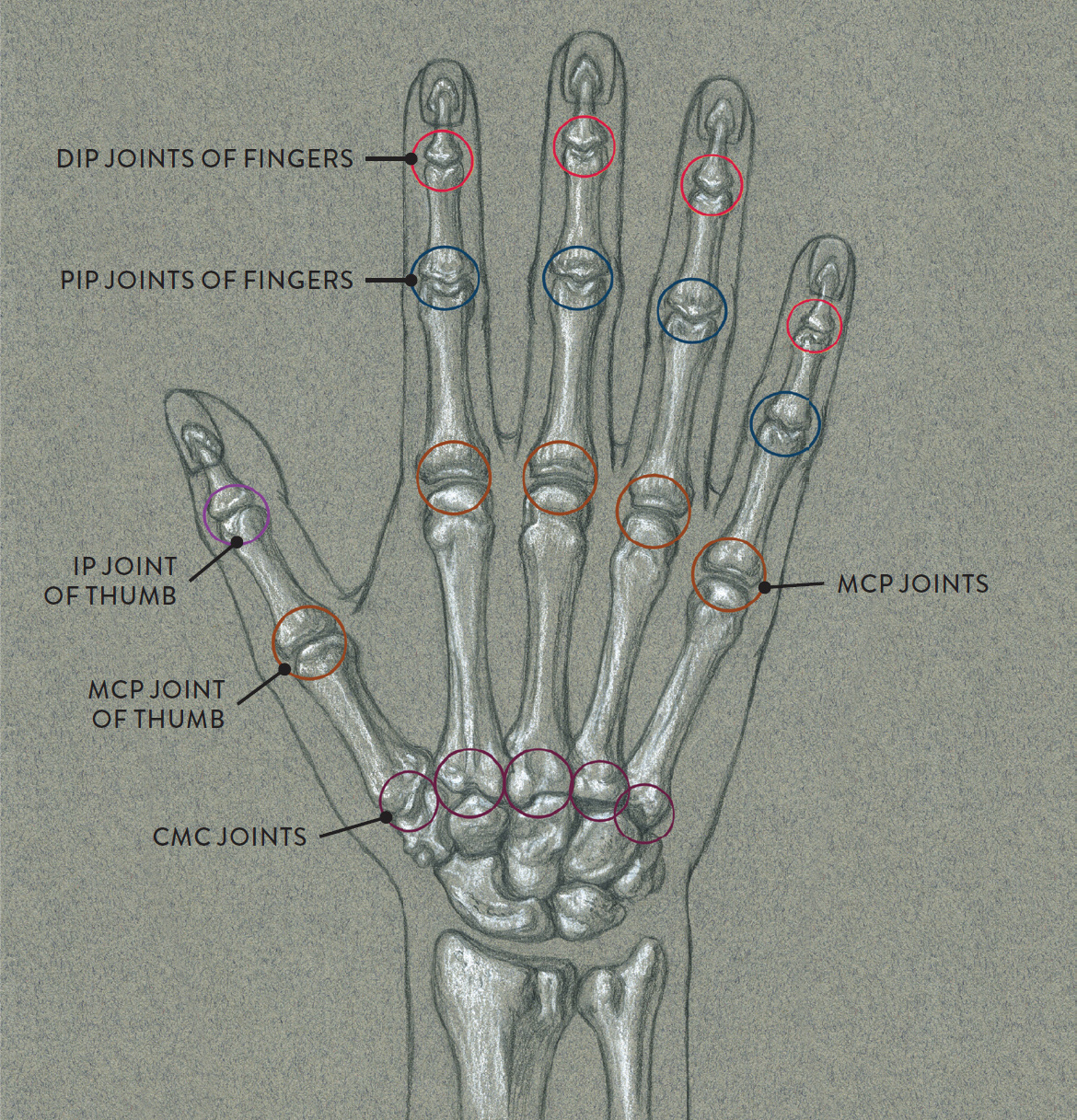
Right hand, dorsal surface
IP JOINT: Interphalangeal joint
DIP JOINT: Distal interphalangeal joint
PIP JOINT: Proximal interphalangeal joint
MCP JOINT: Metacarpophalangeal joint
CMC JOINT: Carpometacarpal joint
The carpometacarpal joints (pron., KAR-poe-met-tah-KAR-poll), or CMC joints, are the joints between the carpal and metacarpal bones. All are classified as gliding/plane joints with the exception of the joint between the metacarpal of the thumb and the trapezium carpal bone, which is a saddle joint. There is very little movement at the CMC joints at the second and third metacarpals. Gliding movement occurs in the fourth and fifth metacarpals.
The CMC joint of the thumb has much greater movement capability than the other CMC joints because of the articulating ends on both the trapezium carpal bone and the metacarpal bone of the thumb. Thumb movements include flexion and extension, which are the bending and straightening of the thumb, and abduction and adduction, which are the moving of the thumb away from the palm in a forward direction and the return of the thumb to the side of the hand. These movements are shown in the drawings Abduction and Adduction of Thumb at the CMC Joint and Flexion and Extension of Thumb at the CMC Joint. Other thumb movements, not shown here, are opposition and reposition, in which the thumb moves across the palm to touch the tips of the fingers and then returns to its neutral position, circumduction, which is the circular movement of the entire thumb.
ABDUCTION AND ADDUCTION OF THUMB AT THE CMC JOINT
Saddle joint action
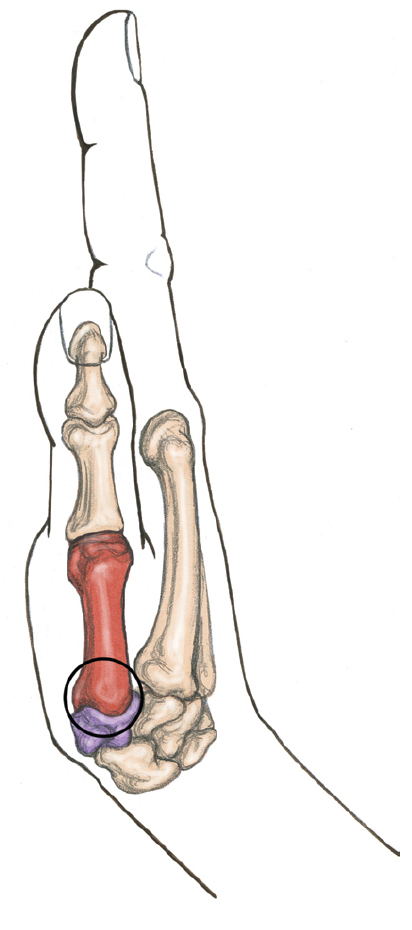
Neutral position of thumb
Circle indicates the CMC joint of thumb and the saddle joint.
ABDUCTION AND ADDUCTION OF THUMB AT THE CMC JOINT (CONTINUED)
Saddle joint action
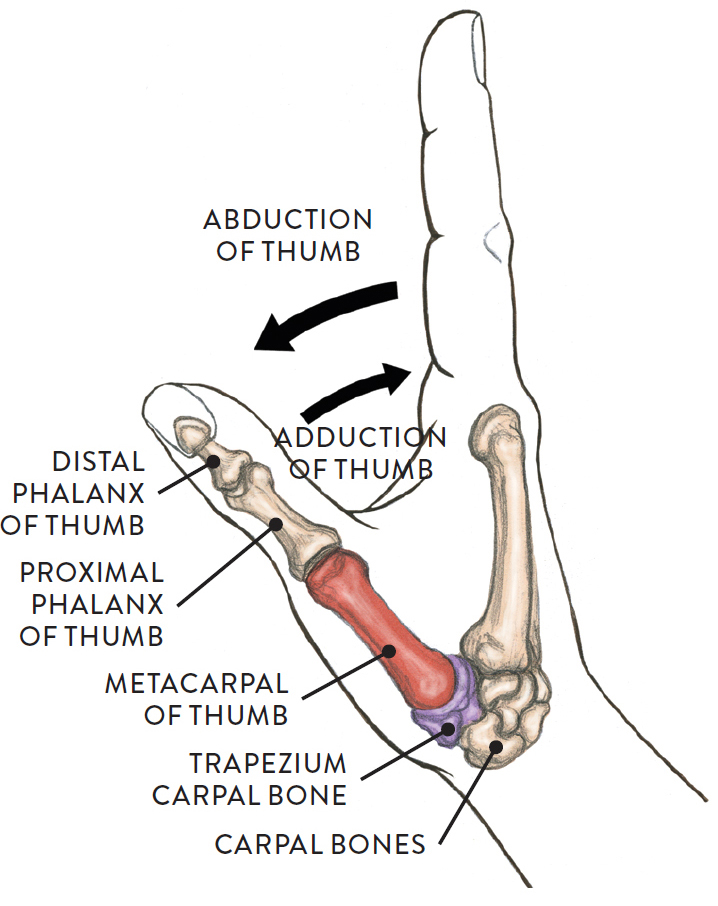
Lateral view of right hand
FLEXION AND EXTENSION OF THUMB AT THE CMC JOINT
Saddle joint action
In the action of flexion, the thumb is pulled across the palm. The reversal of this action is extension.
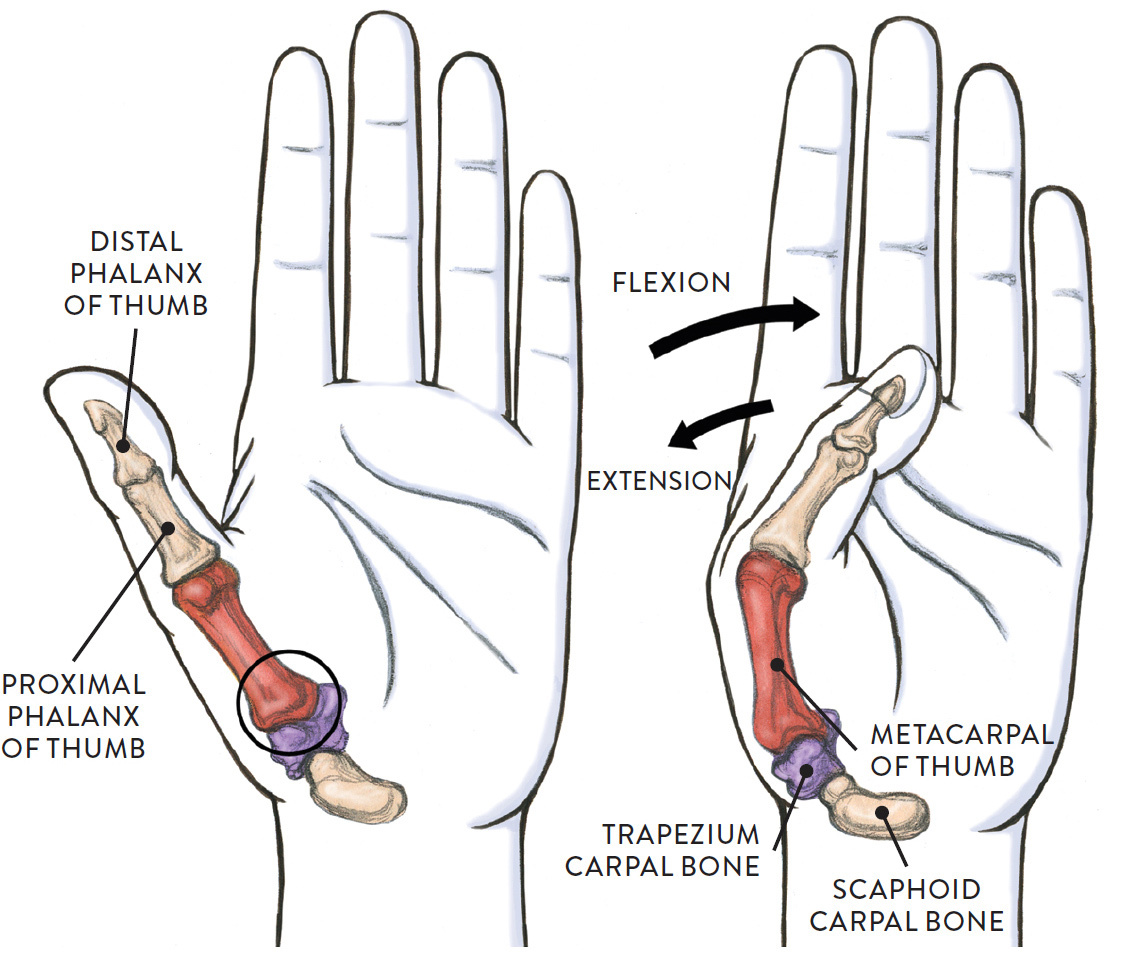
Circle indicates the CMC joint of the thumb and the saddle joint.
LEFT: Palmar view of left hand
RIGHT: Thumb moving from the CMC joint
The metacarpophalangeal joints (pron., MET-ah-KAR-poe-fah-LAN-jee-ul), or MCP joints, are the joints between the metacarpal bones and the phalanges (finger bones and thumb bone) and are classified as ellipsoid/condyloid joints. The heads of the metacarpals (commonly referred to as the knuckles of the hand) appear near the surface when the fingers and thumb bend at the MCP joints. When the fingers or thumb extend or straighten, the knuckles are no longer visible on the surface.
The movements of the fingers at the MCP joints are flexion and extension (bending and straightening of the fingers at the MCP joint), abduction and adduction (the spreading of fingers and the return of the spread fingers to normal position), and circumduction, which is the circular movement of a whole finger (not shown in drawing).
In the drawing Abduction and Adduction of Fingers at the MCP Joints, we see the action of spreading the fingers apart and back. The third finger (middle finger) remains stabilized in the movements of abduction and adduction and is considered the midline of the hand. The second finger moves sideways away from the third finger, and the fourth and fifth fingers move sideways away from the third finger in the other direction.
ABDUCTION AND ADDUCTION OF FINGERS AT THE MCP JOINTS
Ellipsoid/condyloid joint actions
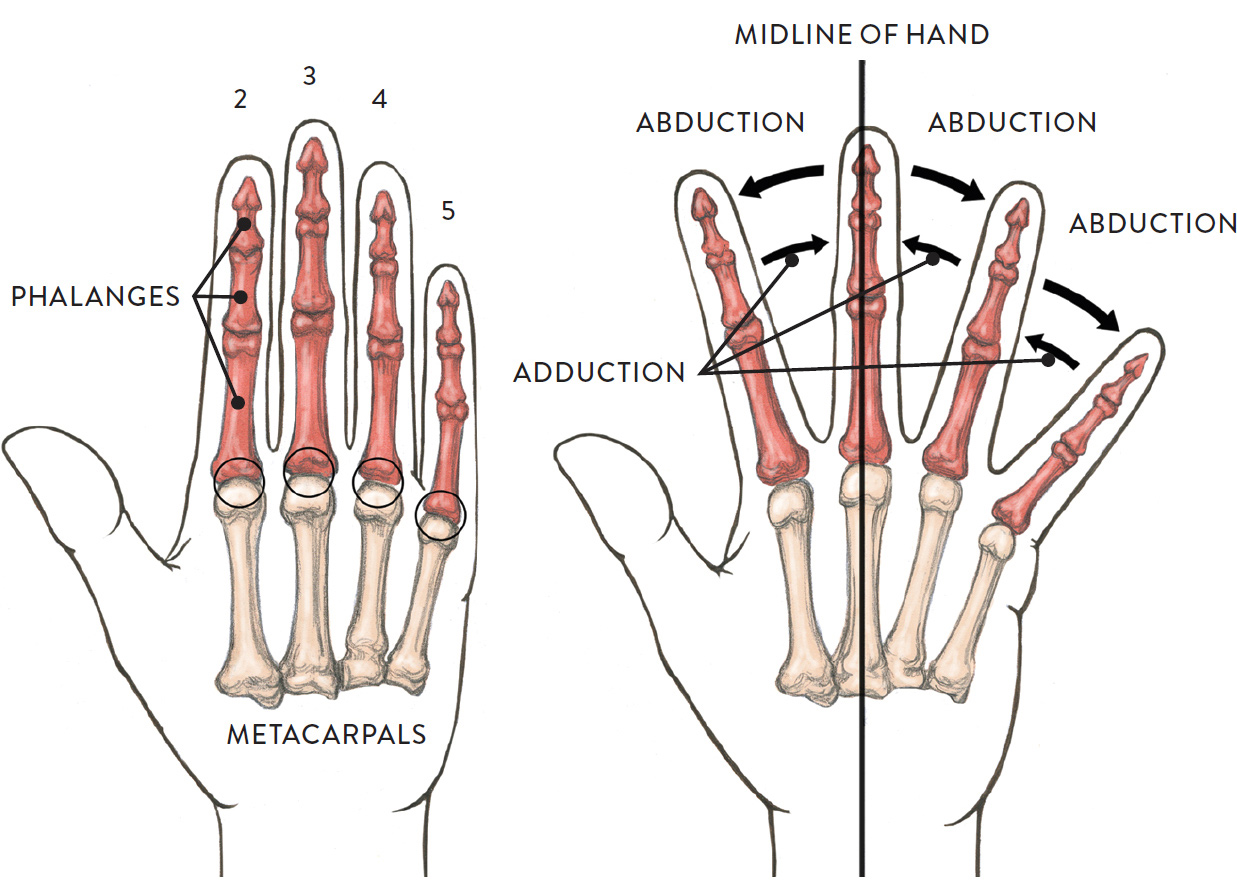
Circles indicate MCP joints.
LEFT: Fingers in straight alignment to the palm—palmer view of the left hand
RIGHT: Fingers spreading outward from the midline is abduction; the reverse of this action is adduction
The movements of the thumb at the MCP joint, not shown here, are flexion and extension. Flexion is the bending together of the two phalanges of the thumb at the MCP joint; extension returns the two thumb phalanges back to their normal position. The thumb can also slightly rotate from its CMC joint because this joint is a saddle joint, allowing more movement than the ellipsoid/condyloid joint at the MCP.
The interphalangeal joints (pron., in-ter-fah-LAN-jee-ul), or IP joints, are the joints between the phalanges; they are classified as hinge joints. They are also referred to as the knuckles of the fingers. The proximal interphalangeal joint (PIP joint) is located between the proximal phalanx (closer to wrist) and the middle (or intermediate) phalanx. The distal interphalangeal joint (DIP joint) is located between the distal phalanx (farther from wrist) and the middle (or intermediate) phalanx. The only movements the fingers can produce at the IP joints (PIP and DIP) are flexion and extension—the bending and straightening of the phalanges (finger bones).
In the drawing Flexion and Extension of Finger at the IP Joints, we see a lateral view of the straight index finger and, below it, the movements of flexion and extension. In the movement of flexion the finger bones (phalanges) can either bend slightly or tightly curl the whole finger. Extension is the action of straightening the bones of the fingers from a flexed position. As mentioned, flexion and extension also occur at the knuckles (MCP joints) of the hand. The thumb (not shown) has only one IP joint, which also flexes and extends.
FLEXION AND EXTENSION OF FINGER AT THE IP JOINTS
Hinge joint action
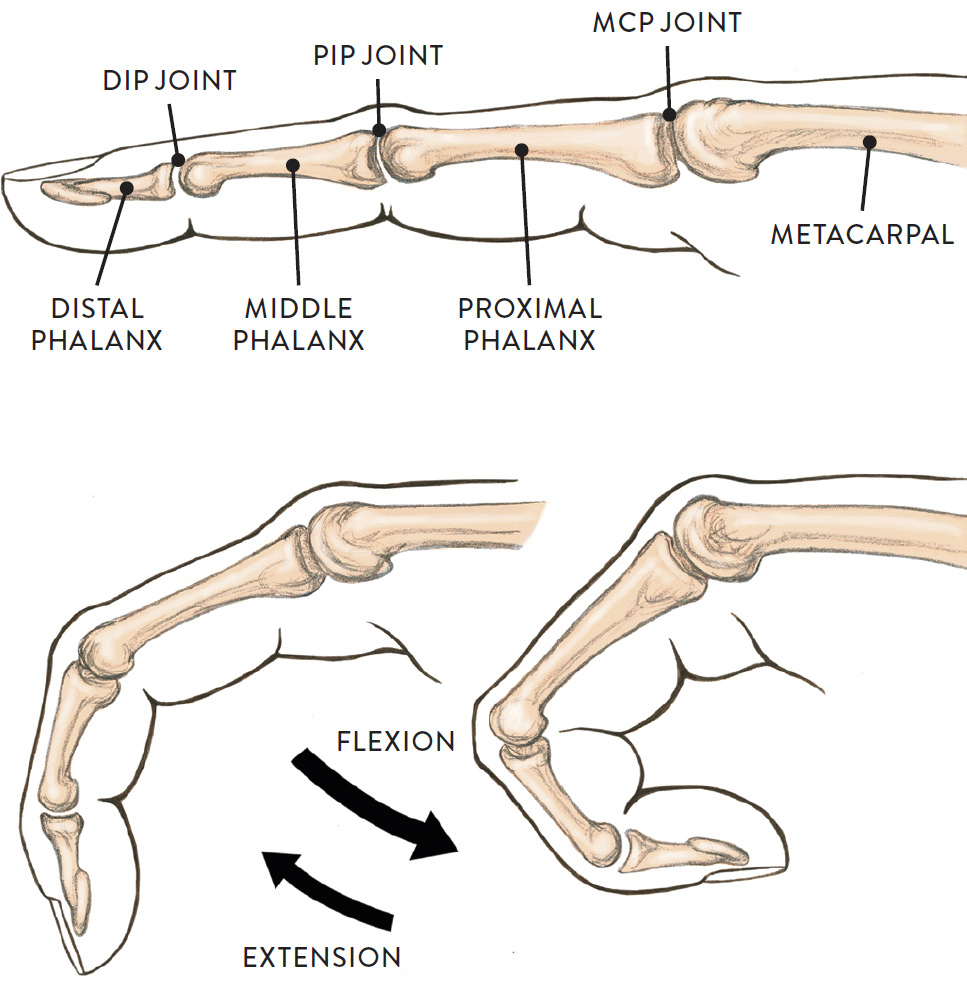
Lateral view of index finger of right hand
Joints of the Lower Limb
The main joints of the lower limb, shown in the drawing next, include the hip joint, knee joint, ankle joint, and the joints of the foot and toes. The pelvic girdle is considered to be an important component of this region because it is the supportive framework into which the lower limbs connect. Since we have already looked at the joints of the pelvis, we focus here on the joints of the lower limb to see how they function in various movements.
MAIN JOINTS OF THE LOWER LIMB
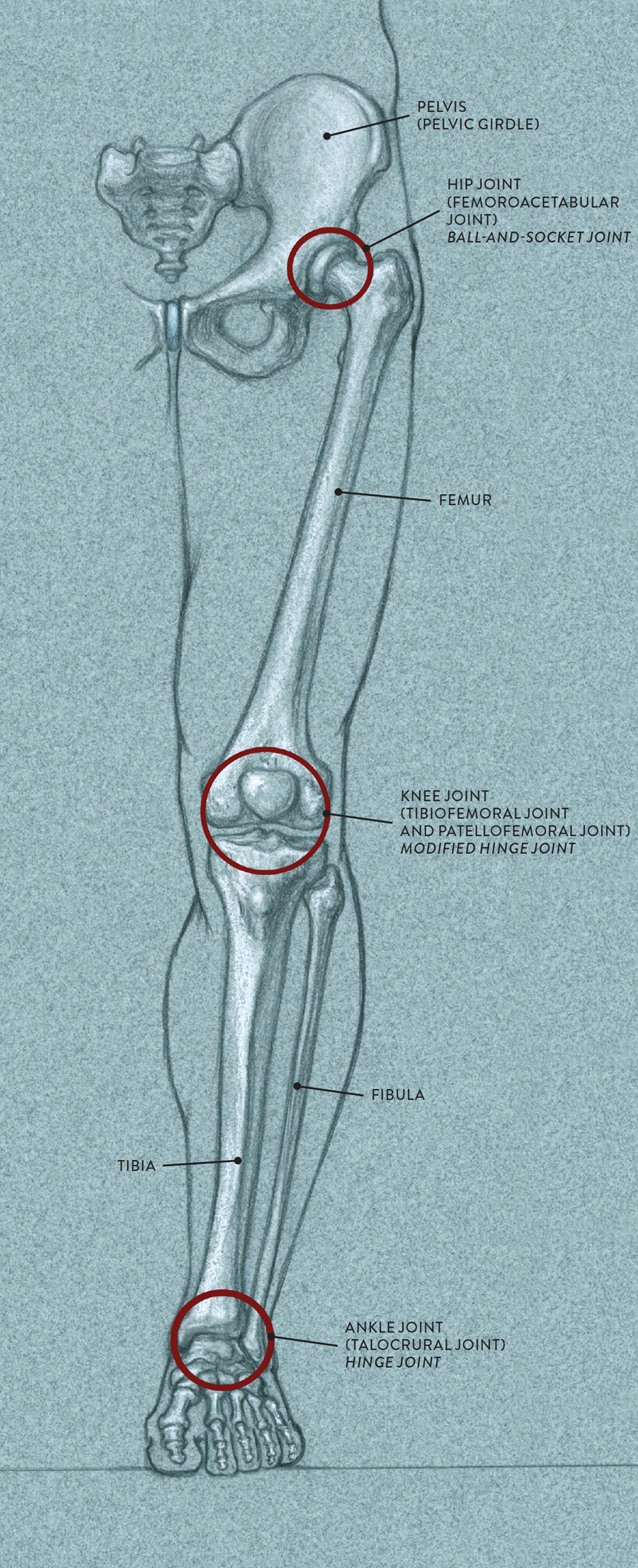
Left leg, anterior view
The Hip Joint
The hip joint, also called the femoroacetabular joint (pron., FEM-er-oh-ah-see-TAB-byoo-lar), consists of the golf ball–shaped head of the femur and the cup-shaped socket (acetabulum) within the pelvis. The femur of the upper leg has the capability of moving in a wide variety of directions because of the shape of this ball-and-socket joint. The hip joint itself is hidden under ligaments and muscular forms and so cannot be seen on the surface; however, landmarks such as the greater trochanter of the femur can be detected, helping locate the general placement of the hip joint.
HIP JOINT (FEMOROACETABULAR JOINT)
Ball-and-socket joing
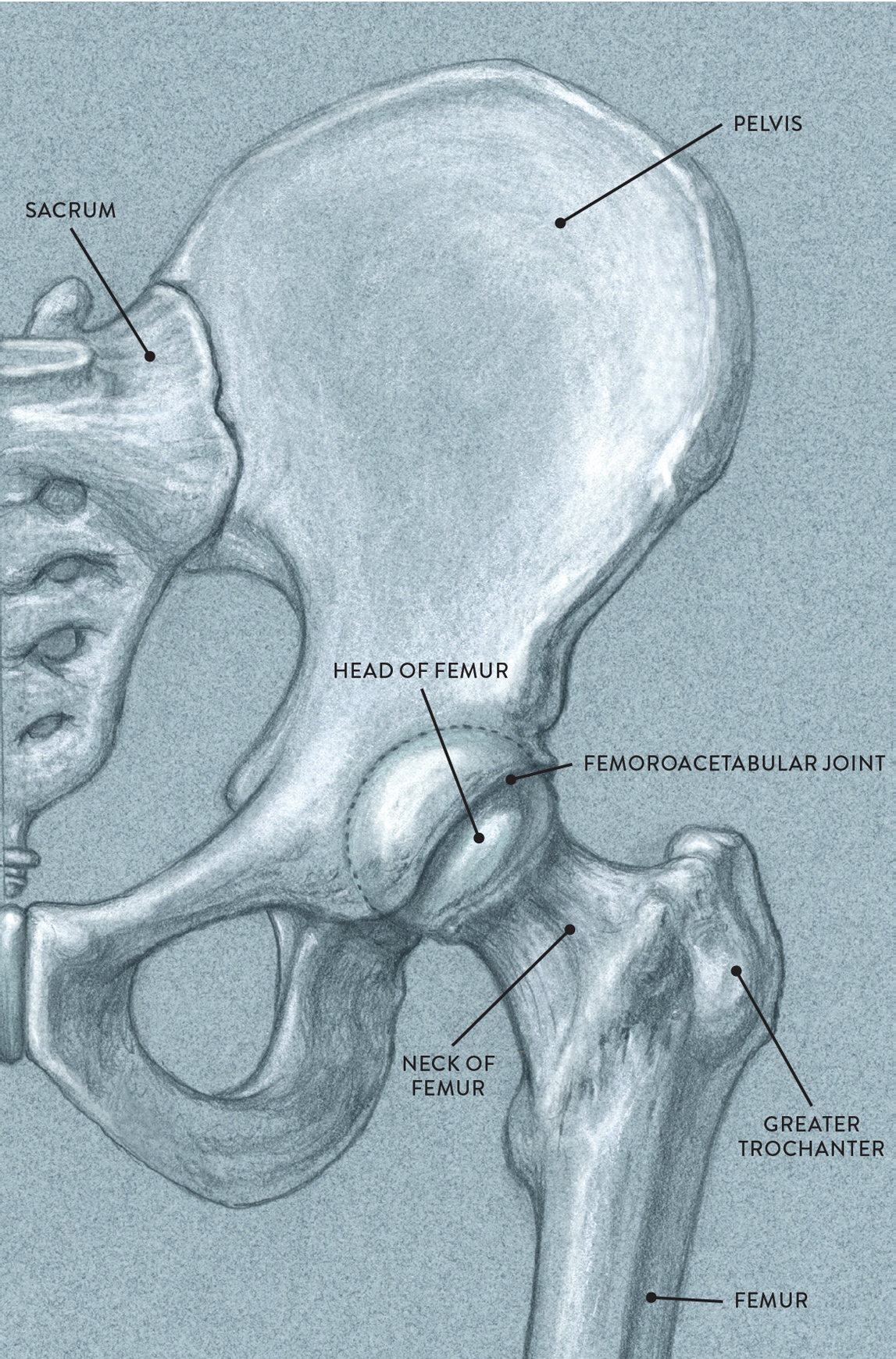
Anterior view of left side of pelvis and upper portion of femur
Movements produced at the hip joint include flexion and extension (moving the femur in forward-and-back directions), abduction and adduction (moving the femur sideways), lateral and medial rotation of the femur (rotating the femur outward or inward), and circumduction (circular motion of entire femur). In the drawing Flexion and Extension of Femur at the Hip Joint, we see the forward-and-back movements of the femur. In flexion, the upper leg can move forward with the lower leg bent or with the lower leg in the same straight alignment as the upper leg. This action is seen in many dance movements and in sports actions such as kicking a ball. Extension is the return of the femur back to its normal position, or it can extend farther back, which is sometimes referred as hyperextension of the femur.
FLEXION AND EXTENSION OF FEMUR AT THE HIP JOINT
Ball-and-socket joint action
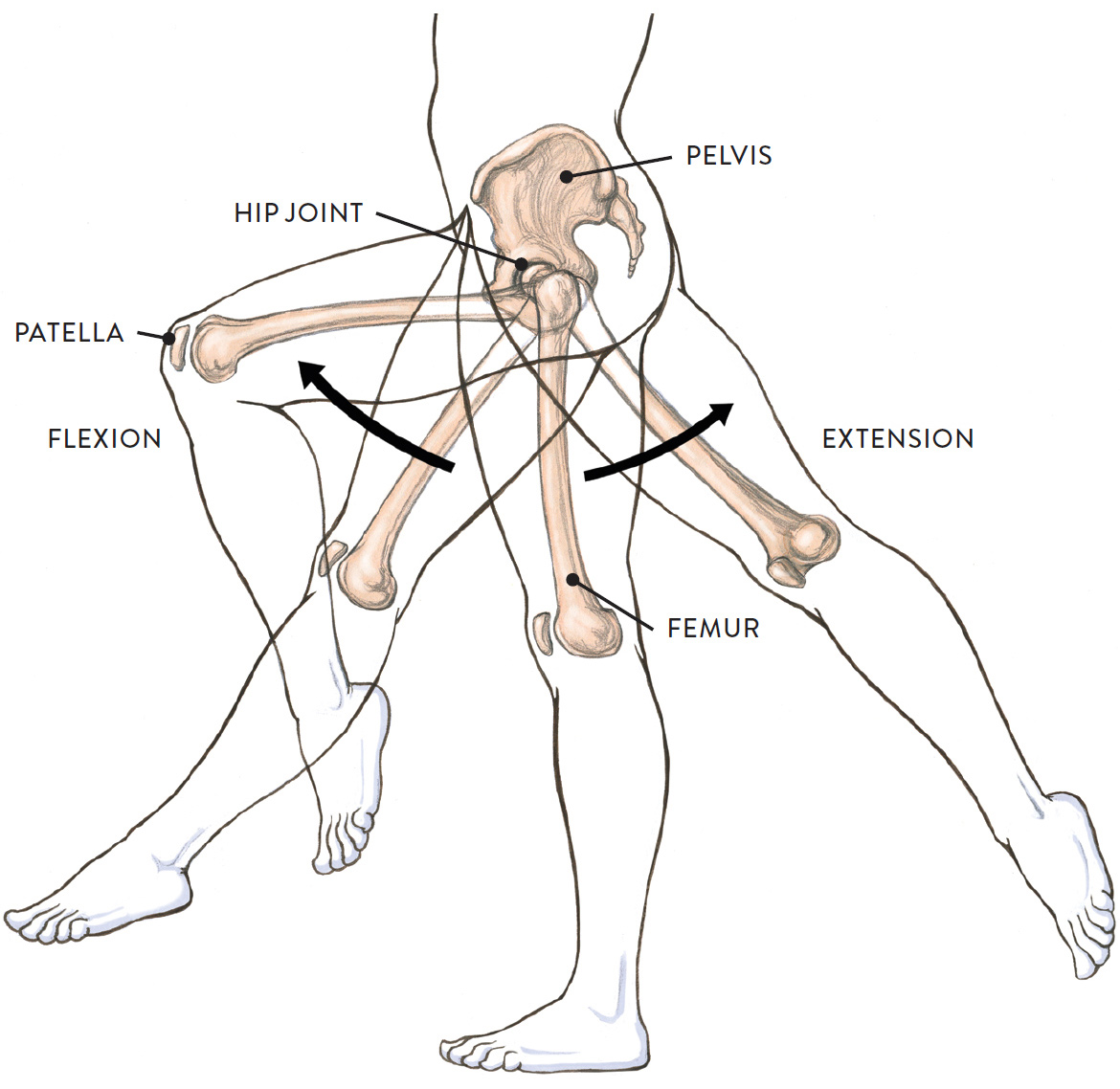
Lateral view of pelvis and left upper and lower leg
The drawing Abduction and Adduction of Femur at the Hip Joint, shows the side-to-side movements of the femur. Abduction is the action of moving the femur away from the medial line (midline) of the body. Adduction is the action of returning the femur back to its normal position. Adduction can go farther, moving the femur past the medial line, as in the action of crossing one leg past the other seen in many dance and sports movements.
ABDUCTION AND ADDUCTION OF FEMUR AT THE HIP JOINT
Ball-and-socket joint action
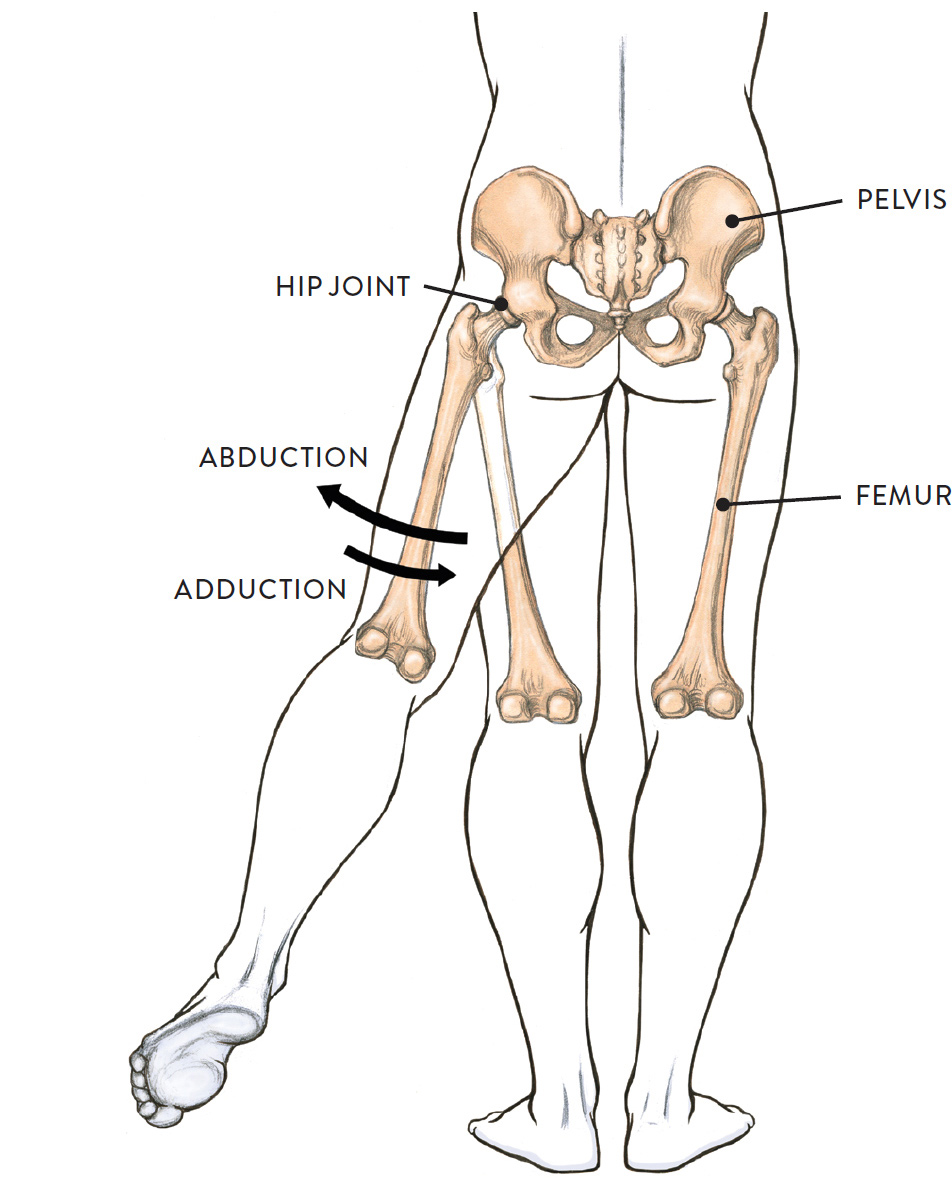
Posterior view of the pelvis and upper and lower legs
Next, in the drawing Lateral and Medial Rotation of Femur at the Hip Joint, we see the rotation of the whole femur, which means the bone is rotating or twisting on its own axis. Medial rotation is rotating the femur toward the midline of the torso; lateral rotation is rotating the femur away from the midline. Both medial and lateral rotation can be combined with other movements.
LATERAL AND MEDIAL ROTATION OF FEMUR AT THE HIP JOINT
Ball-and-socket joint action
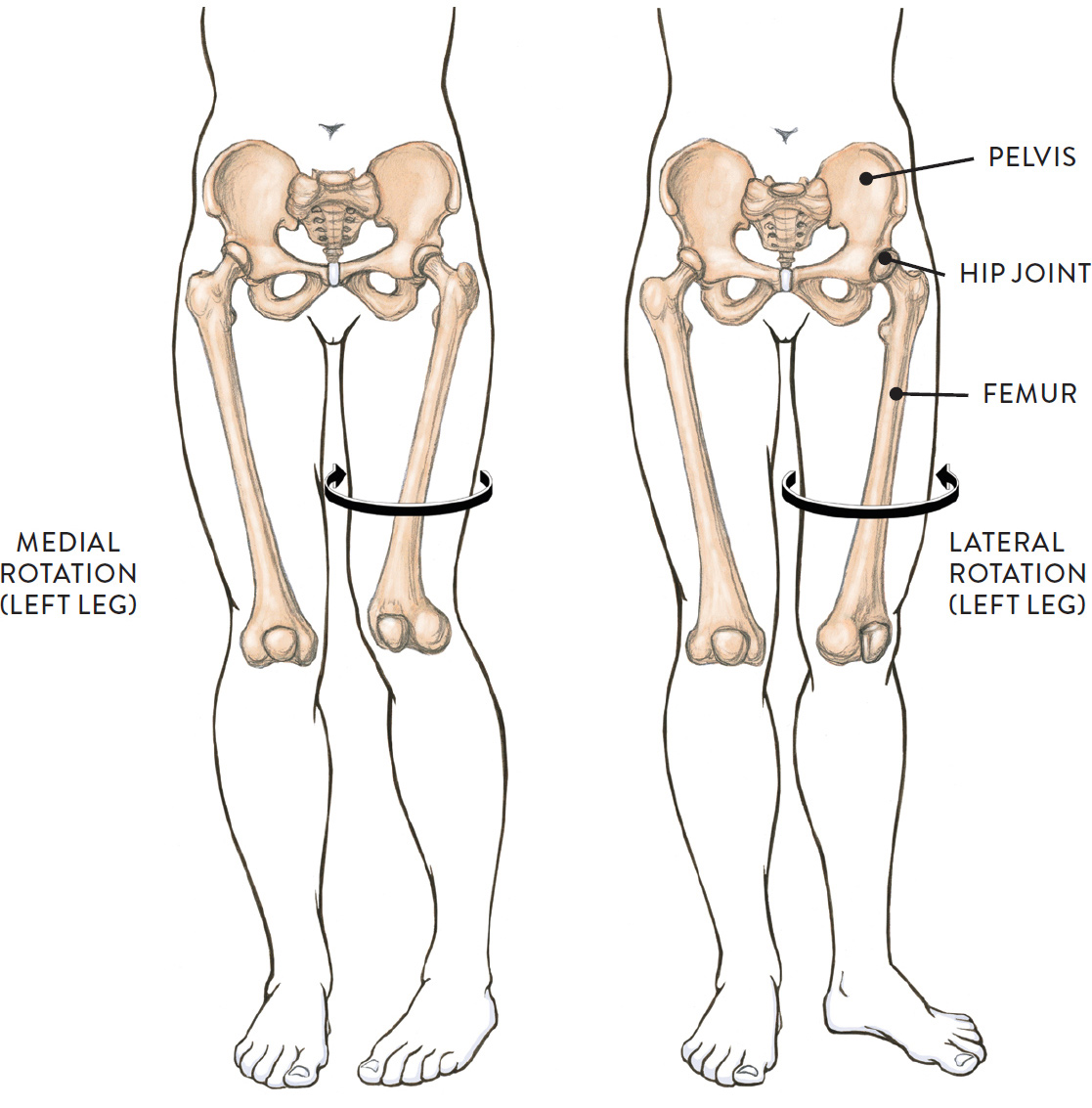
Anterior view of the pelvis and upper and lower legs
Medial and lateral rotation of left leg with a stationary pelvis
Finally, the drawing Circumduction of Femur at the Hip Joint, shows the circular action of the femur. Circumduction is often confused with the rotation of the femur. The difference is that, in circumduction, the whole femur (or thigh) is moving in a circular manner while the head of the femur remains somewhat stabilized in the hip joint, while in rotation the femur is turning on its own axis. The movement of circumduction is essentially that of drawing an imaginary circle with the foot or knee. It can be performed in either a clockwise or counterclockwise direction, and the circular motion can be broader or narrower.
CIRCUMDUCTION OF FEMUR AT THE HIP JOINT
Ball-and-socket joint action
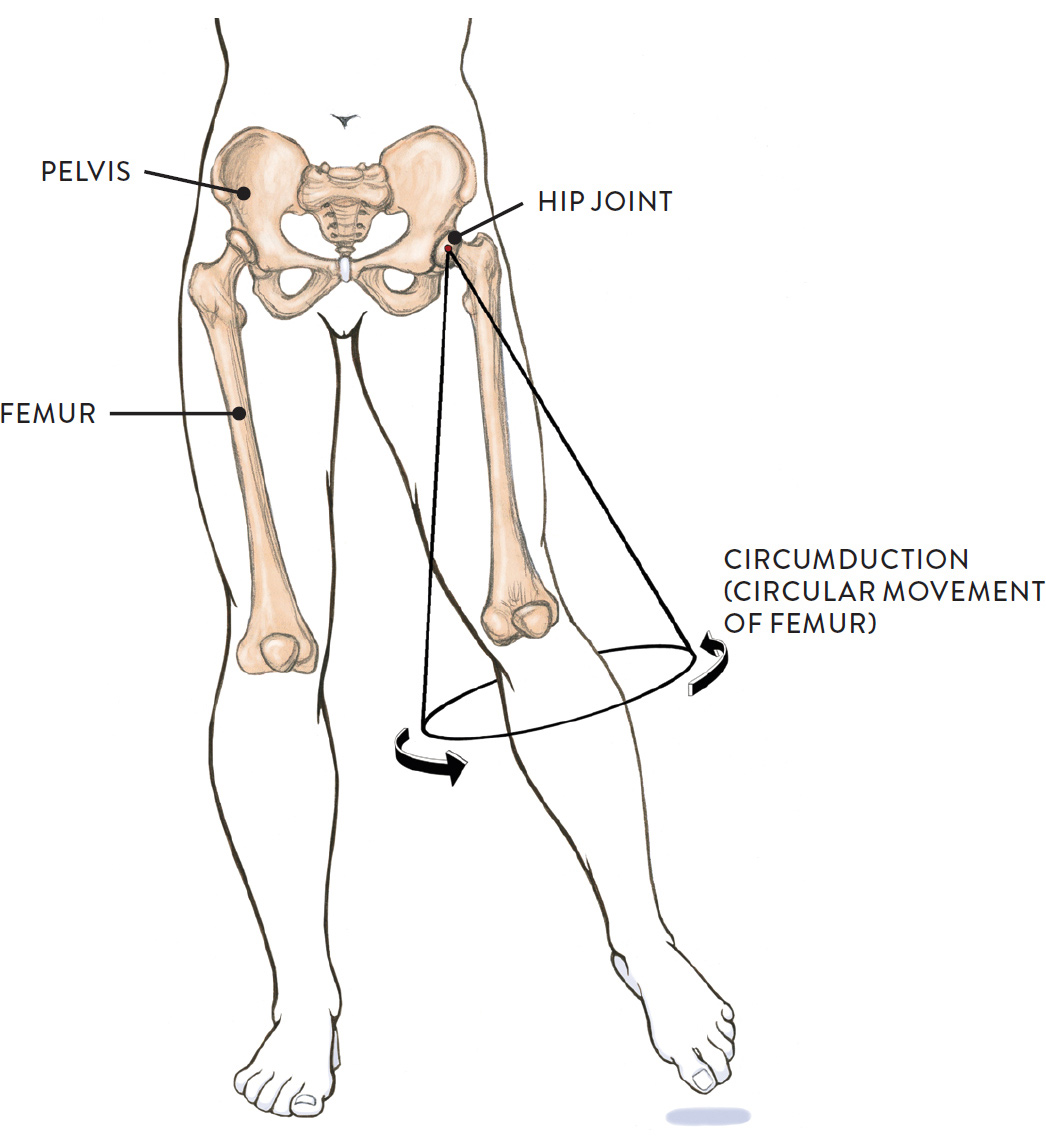
Anterior view of the pelvis and upper and lower legs
The Knee
The knee, which is the largest synovial joint in the body, actually consists of two different joints: the tibiofemoral joint, located between the condyles of the femur bone and the condyles of the tibia, and the patellofemoral joint, which is the joint between the lower anterior portion of the femur bone and the patella. The bones of the knee joint are encased in and connected together by strong cartilages and ligaments.
Names of Knee Joints
The names of knee joints provide clues to their location:
· Tibio pertains to the tibia bone of the lower leg.
· Femoral pertains to the femur bone of the upper leg.
· Patello pertains to the patella (kneecap).
The tibiofemoral joint (pron., TIB-ee-o-FEM-or-al) consists of the condyles of the femur and the condyles of the tibia. In the drawing Movement of the Tibia or Femur at the Tibiofemoral Joint of the Knee, we see the knee movements of flexion and extension, in which the femur condyles roll and glide on top of the tibia condyles. These actions occur when bending and straightening the lower leg, as when kicking a ball, or when bending and straightening the upper leg over a fixed lower leg, as in the actions of sitting down and standing up. In the action of sitting, the hip joint is also activated. During flexion and extension, there is also a slight lateral rotation or medial rotation of the femur condyles; because of these additional minimal movements, the tibiofemoral joint is considered a modified hinge joint.
MOVEMENT OF THE TIBIA OR FEMUR AT THE TIBIOFEMORAL JOINT OF THE KNEE
Modified hinge joint action between the condyles of the femur and tibia
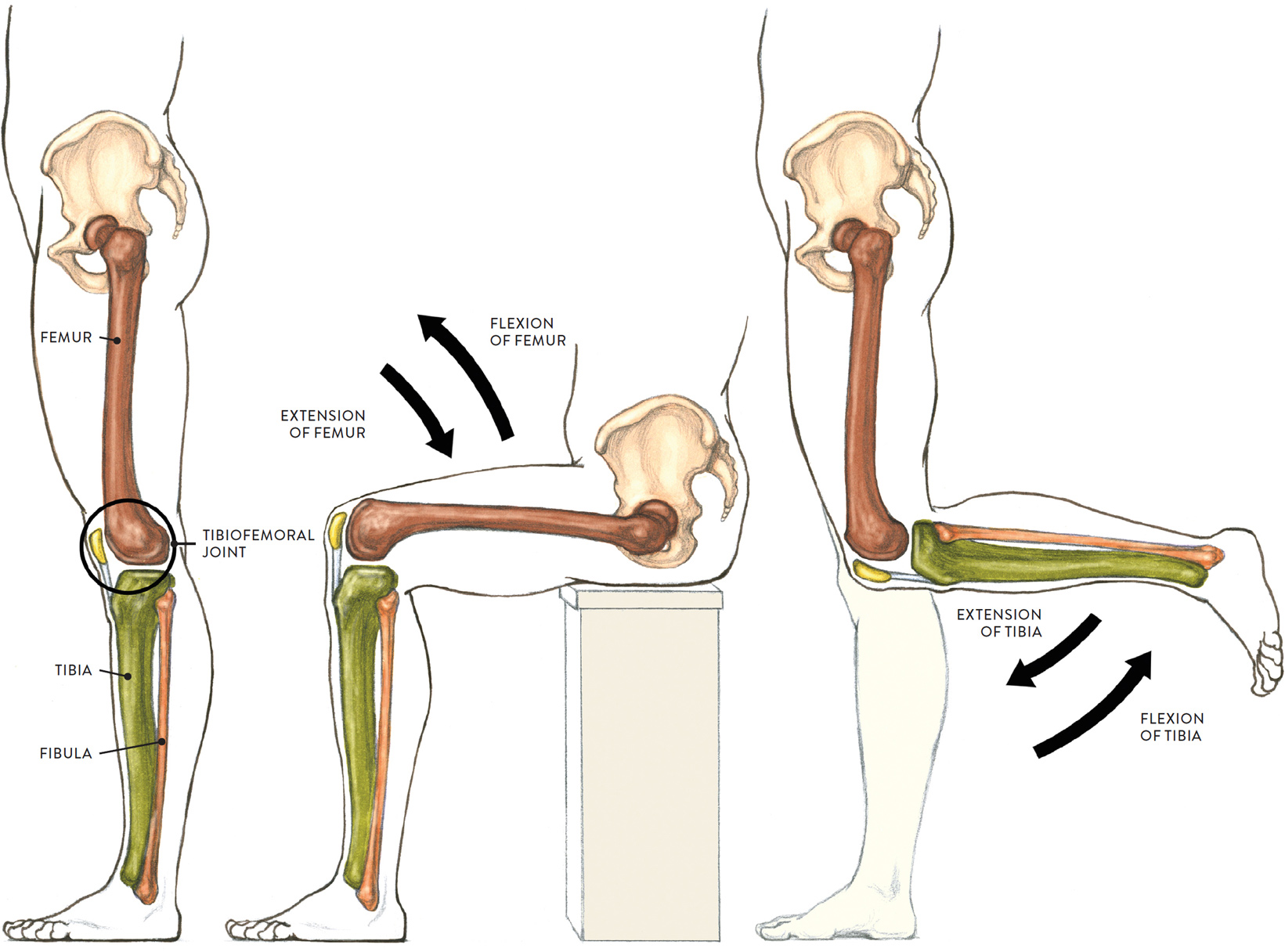
Lateral view of the pelvis and left leg
LEFT: Neutral position
CENTER: Sitting down and standing up
RIGHT: Lifting and lowering lower leg
The second articulation of the knee joint is the patellofemoral joint (pron., puh-TELL-o-FEM-or-al). This joint between the femur and the patella is considered a gliding/plane joint. The quadriceps tendon runs along a smooth, slightly indented surface on the femur called the patellar surface of the femur, which is located between the two anterior femoral condyles. The tendon attaches into the patella, embedding it in its fibers. The patellar ligament, a straplike form, continues from the lower portion of the patella to attach on the tibial tuberosity, which is a noticeable small protrusion on the upper part of the tibia. The quadriceps tendon, patella, and the patellar ligament act like a cable moving between the large condyles of the femur, which are shaped somewhat like a pulley.
The drawing Movement of the Patella at the Patellofemoral Joint of the Knee, shows how the patella (kneecap) moves during flexion and extension of the knee region. The kneecap moves in slightly upward and downward directions during flexion and extension. Various ligaments attach into the patella to keep it from moving side to side. When the quadriceps muscle contracts on a standing leg, the patella is pulled upward from its normal position.
MOVEMENT OF THE PATELLA AT THE PATELLOFEMORAL JOINT OF THE KNEE
Gliding joint action between the patella and femoral condyles
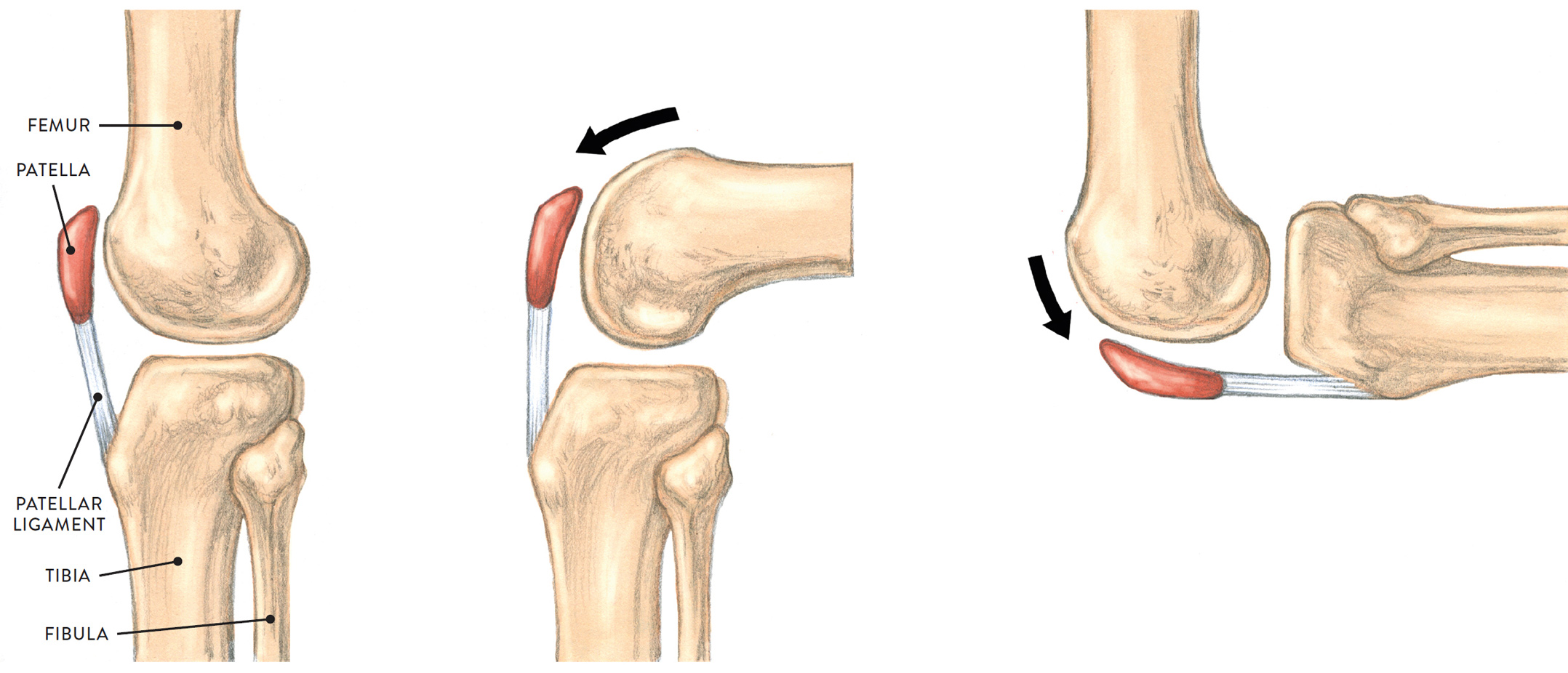
Lateral view of left knee joint
LEFT: Neutral position
CENTER: Upper leg bending with fixed lower leg
RIGHT: Lower leg bending with fixed upper leg
When knee is bent (as shown in CENTER and RIGHT images), the patella glides on the patellar surface of the femur, moving slightly downward.
The Ankle Joint
The ankle joint, also called the talocrural joint (pron., TAY-lo-KROO-rul) joins three bones: the lower portions of both the tibia and the fibula bones and the upper portion of the talus bone of the foot. These bones help support the weight of the body and also play an important role in locomotion. The ankle joint is classified as a hinge joint.
As shown in the drawing, the upper portion of the talus (the trochlear portion or talar dome) is smooth and somewhat dome-shaped and is wedged between, or gripped by, the two ankle bones—the lateral malleolus of the fibula (outer ankle) and medial malleolus of the tibia (inner ankle).
ANKLE JOINT (TALOCRURAL JOINT)
Hinge joint
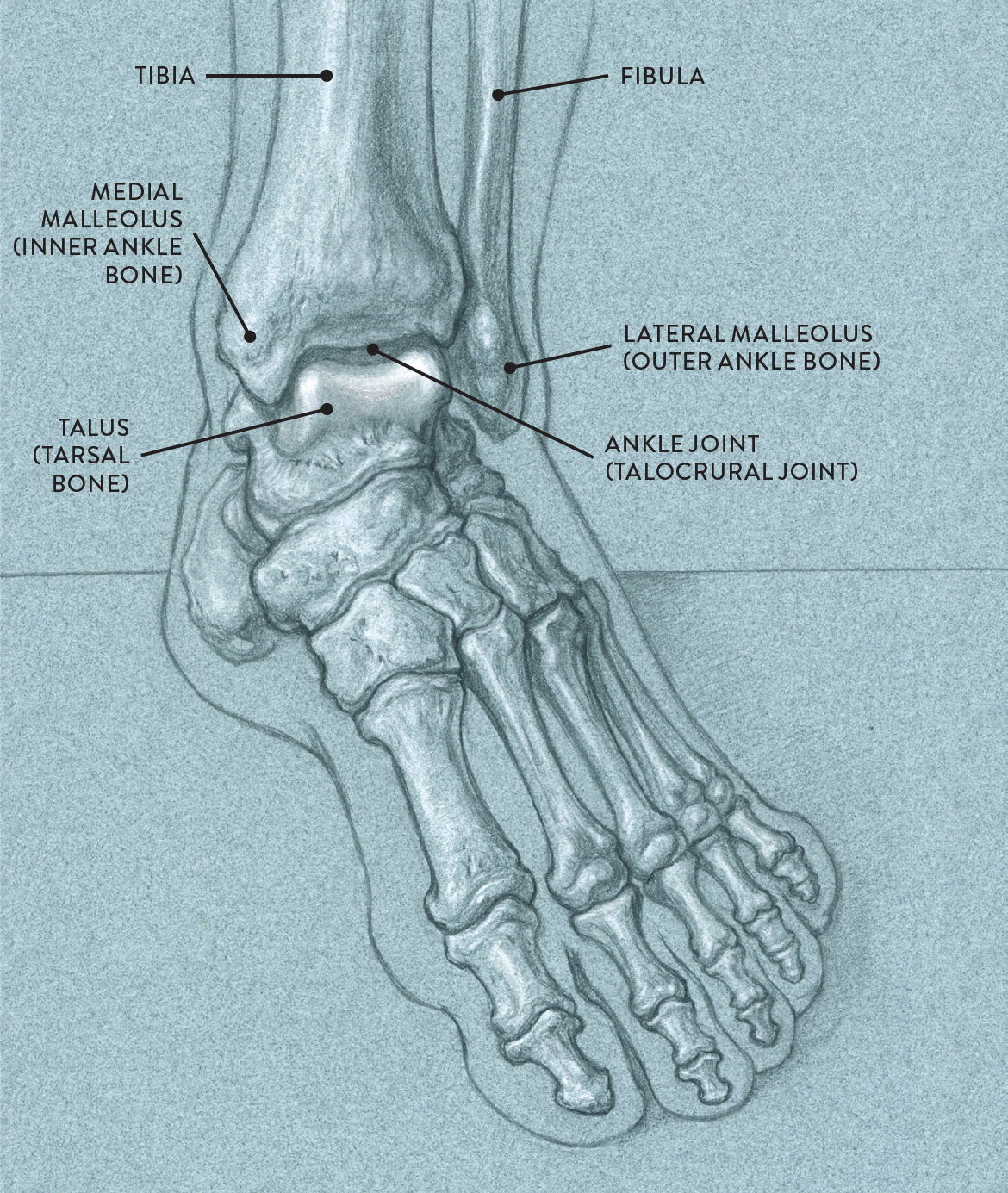
Three-quarter anterior view of the left foot and ankle region
In the drawing Dorsiflexion and Plantar Flexion at the Ankle Joint, we see how the foot moves in up and down directions at the ankle joint. Dorsiflexion is lifting or swinging the front part of the foot upward and pushing the heel downward. In this particular movement, the toes tend to spread apart slightly. This movement occurs in walking and running, preventing the toes from scraping the ground when the foot moves forward in a stride. Plantar flexion is the pointing of the front portion of the foot downward and lifting the heel upward. In this action, the toes tend to push together, as can be seen in many ballet movements. This hingelike action propels the body forward in movements such as walking, running, and leaping.
DORSIFLEXION AND PLANTAR FLEXION AT THE ANKLE JOINT
Hinge joint action
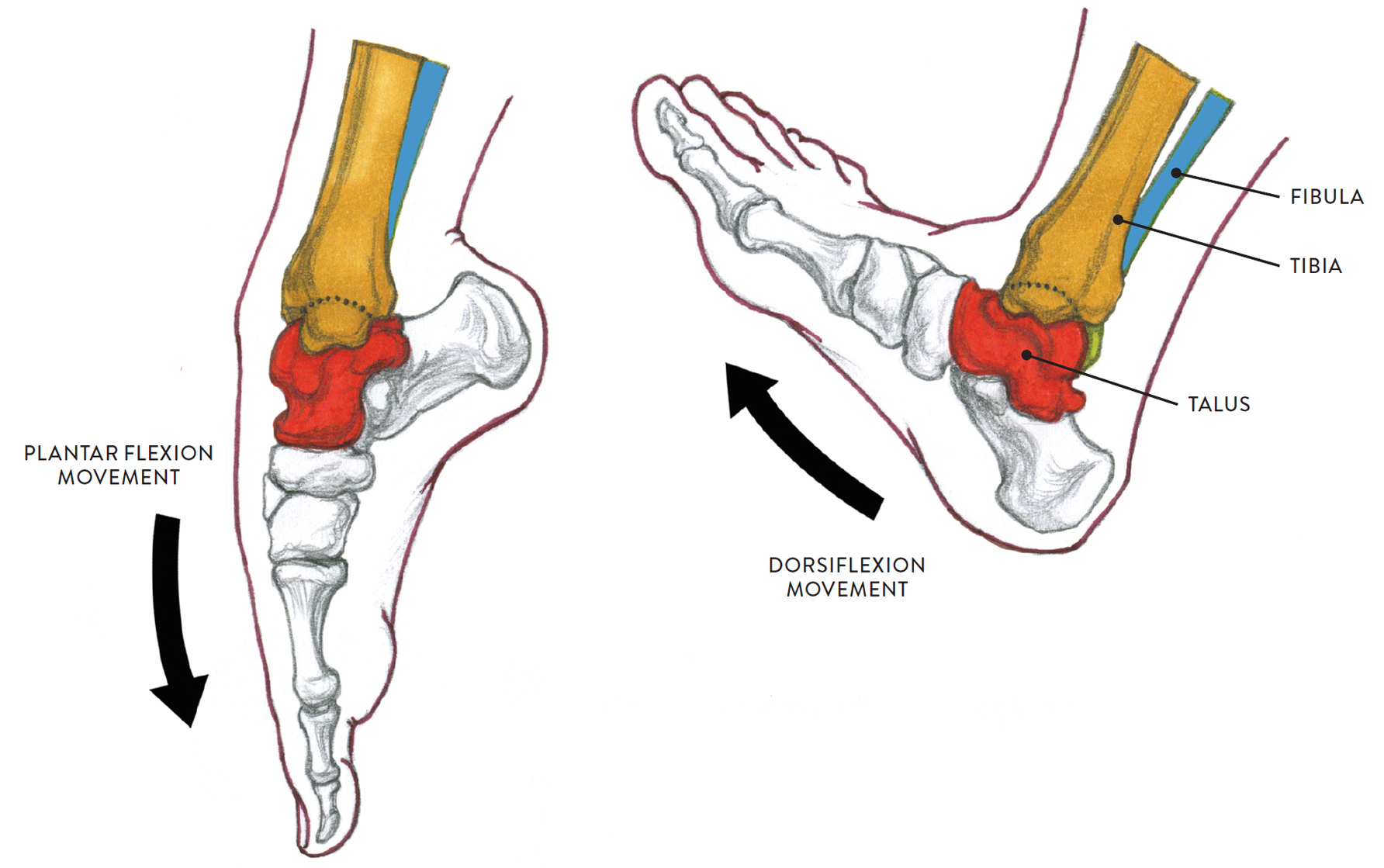
Non-weight-bearing positions (foot suspended above ground)
DORSIFLEXION AND PLANTAR FLEXION AT THE ANKLE JOINT (CONTINUED)
Hinge joint action
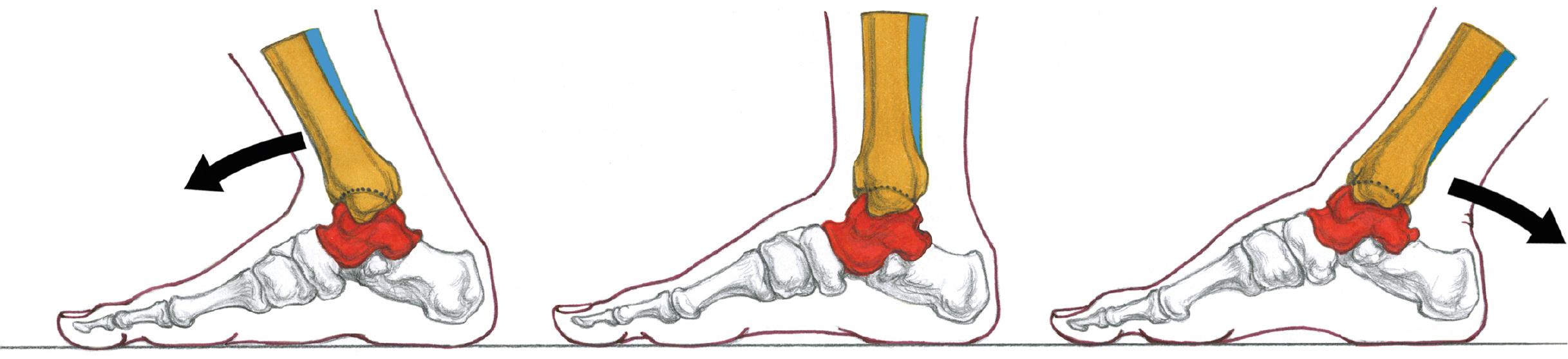
Weight-bearing positions (foot placed on the ground)
LEFT: Lower leg leans forward, with arch pressed lower to the ground
CENTER: The foot is in neutral position, with normal arch
RIGHT: Lower leg leans back, with arch raised higher
The Joints of the Foot
As Leonardo da Vinci noted, the human foot is a masterpiece of engineering. It is not only capable of supporting the weight of the entire body but also serves as a biomechanical structure helping propel the body in various movements, both horizontally (walking, running) and vertically (jumping).
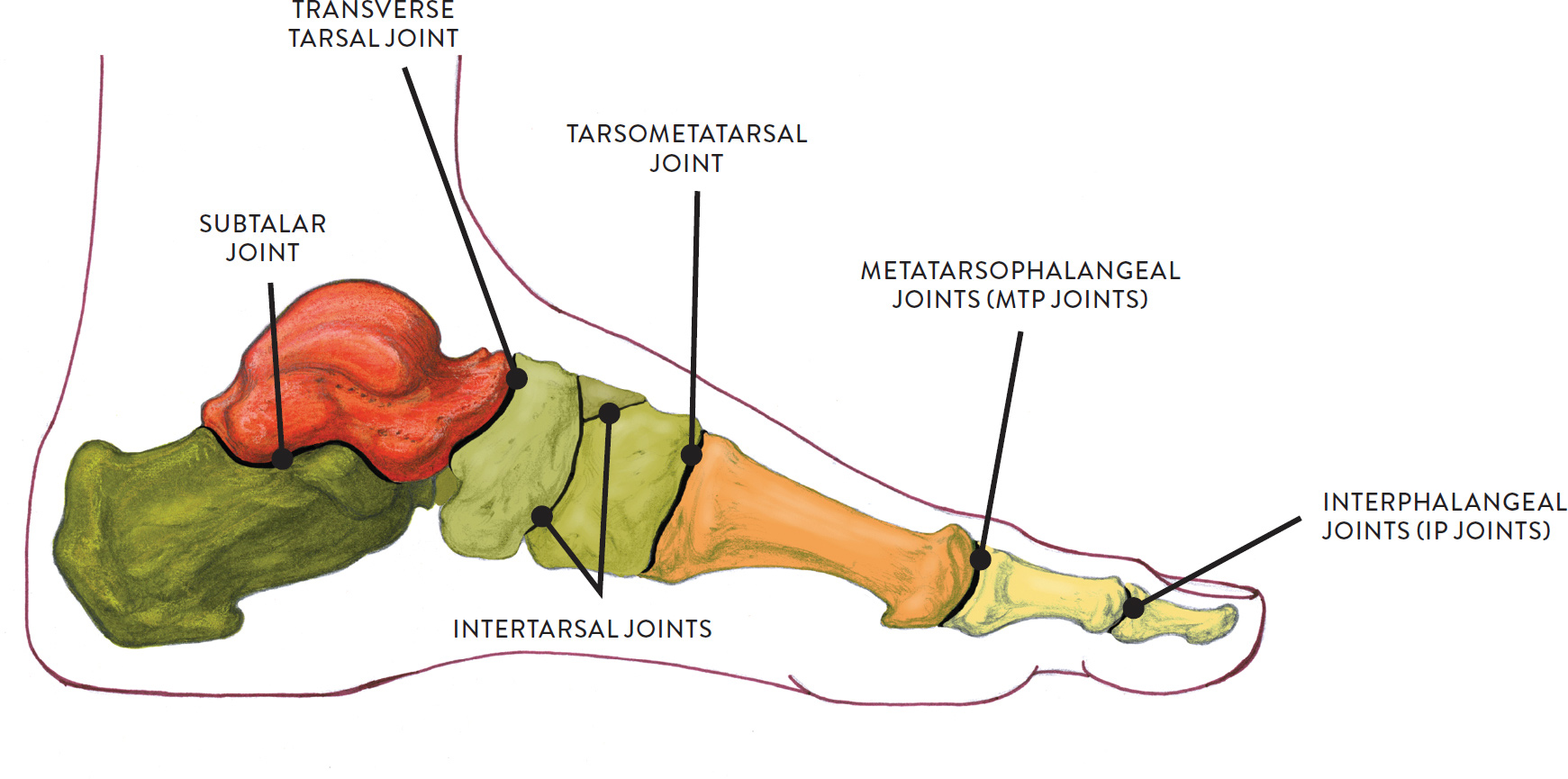
The bones of the foot comprise seven tarsal bones, five metatarsal bones, and fourteen phalanges (toe bones). The joints of the foot, shown in the drawing on this page, are organized into several groups. The first consists of the joints of the tarsal bones: the subtalar joint, tranverse tarsal joint, tarsometatarsal joints (TMT joints), and various small intertarsal joints. Then there are the joints between the metatarsals and toe bones (the metatarsophalangeal joints, or MTP joints) and the joints of the toes (the interphalangeal joints, or IP joints). Most of the joints between the tarsal bones are considered gliding joints.
THE JOINTS OF THE FOOT
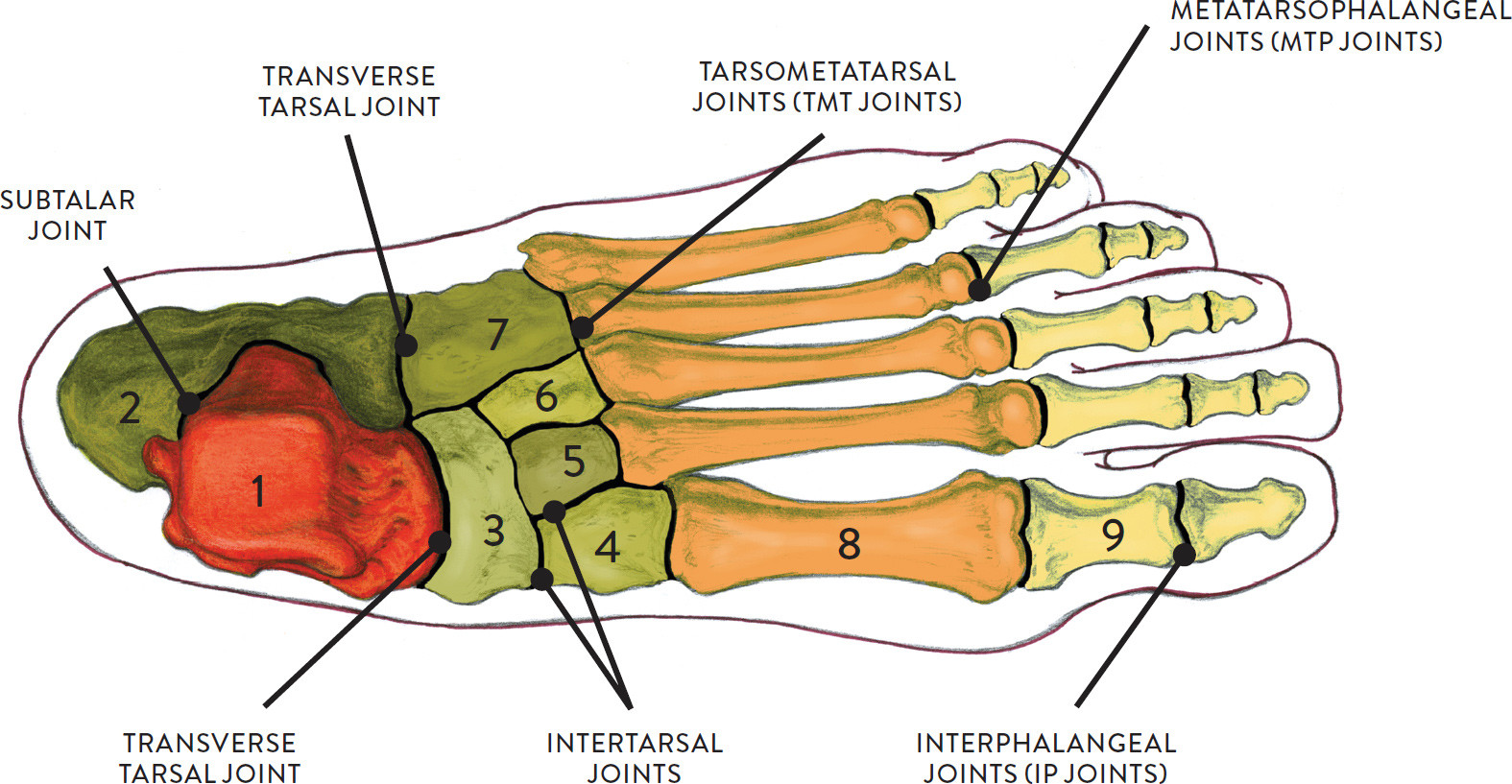
Superior view of left foot
NAMES OF BONES
1. talus
2. calcaneus
3. navicular
4. cuneiform (medial)
5. cuneiform (middle)
6. cuneiform (lateral)
7. cuboid
8. metatarsal
9. phalanx
Intertarsal joints is the collective name for the many joints between the tarsal bones of the foot. Most important are the subtalar joint, tranverse tarsal joints, and tarsometatarsal joints, but there are also numerous little joints between the three cuneiform tarsal bones and the cuboid and navicular tarsal bones. Each of these smaller joints has its own name, but they are identified in the drawings simply as intertarsal joints.
The subtalar joint (pron., SUB-TAL-ar) is the primary tarsal joint of the foot. This is the joint between the lower portion of the talus bone and the upper portion of the calcaneus bone. It is classified as a gliding joint.
The transverse tarsal joint (pron., TAR-sal) is a combination of two joints: One joint is between the talus and navicular tarsal bones and is classified by some experts as a modified ball-and-socket joint because of its convex and concave surfaces. Its movements, however, are limited. The other is between the calcaneus and cuboid tarsal bones and is considered a gliding joint. This combination of joints travels across the foot, hence the term transverse.
The tarsometatarsal joints (pron., TAR-so-MET-a-tar-sal) are the joints between the tarsal bones (cuneiform #1–3 and cuboid) and the proximal ends of the metatarsal bones. They are gliding joints. In weight-bearing movements such as walking, running, and jumping, these joints can alter the general shape of the arches by flattening the foot or “cupping” the foot, depending on the action.
Names of Foot Joints
The names of foot joints provide clues to their location:
· Tarso pertains to the tarsal bones.
· Talo or talar pertains to the talus (a tarsal bone).
· Metatarso pertains to the metatarsal bones.
· Phalangeal pertains to the phalanges (toe bones).
· Calcaneo pertains to the calcaneus (heel bone).
· Transverse means “lying across the long axis of a body part” (in this case, the foot).
· Inter means “in between.”
· Sub means “beneath” (a prefix to other terms).
The movements of eversion and inversion of the foot are produced by gliding and sliding movements between the tarsal and metatarsal bones, combined with movements of dorsiflexion and plantar flexion. These subtle movements are necessary to keep the body balanced when walking on unstable ground, such as a rocky path or sandy terrain. They are also implemented in sports actions such as cupping the foot when hitting a soccer ball or turning the flattened foot outward in martial-arts kicking maneuvers. In the drawing Eversion and Inversion of Foot at the Tarsal and Metatarsal Joints, we see how the foot can bend slightly outward or inward. Eversion is turning the sole or bottom of the foot outward, away from the midline of the body, as when hitting a hacky sack with the outer edge of the foot. Inversion is turning the sole or bottom of the foot toward the midline of the body, as when you look at the bottom of your foot with the sole curling toward you. Inversion can also often be seen in soccer, when a player lifts the ball with the inner edge of the foot.
EVERSION AND INVERSION OF FOOT AT THE TARSAL AND METATARSAL JOINTS
Gliding joint action
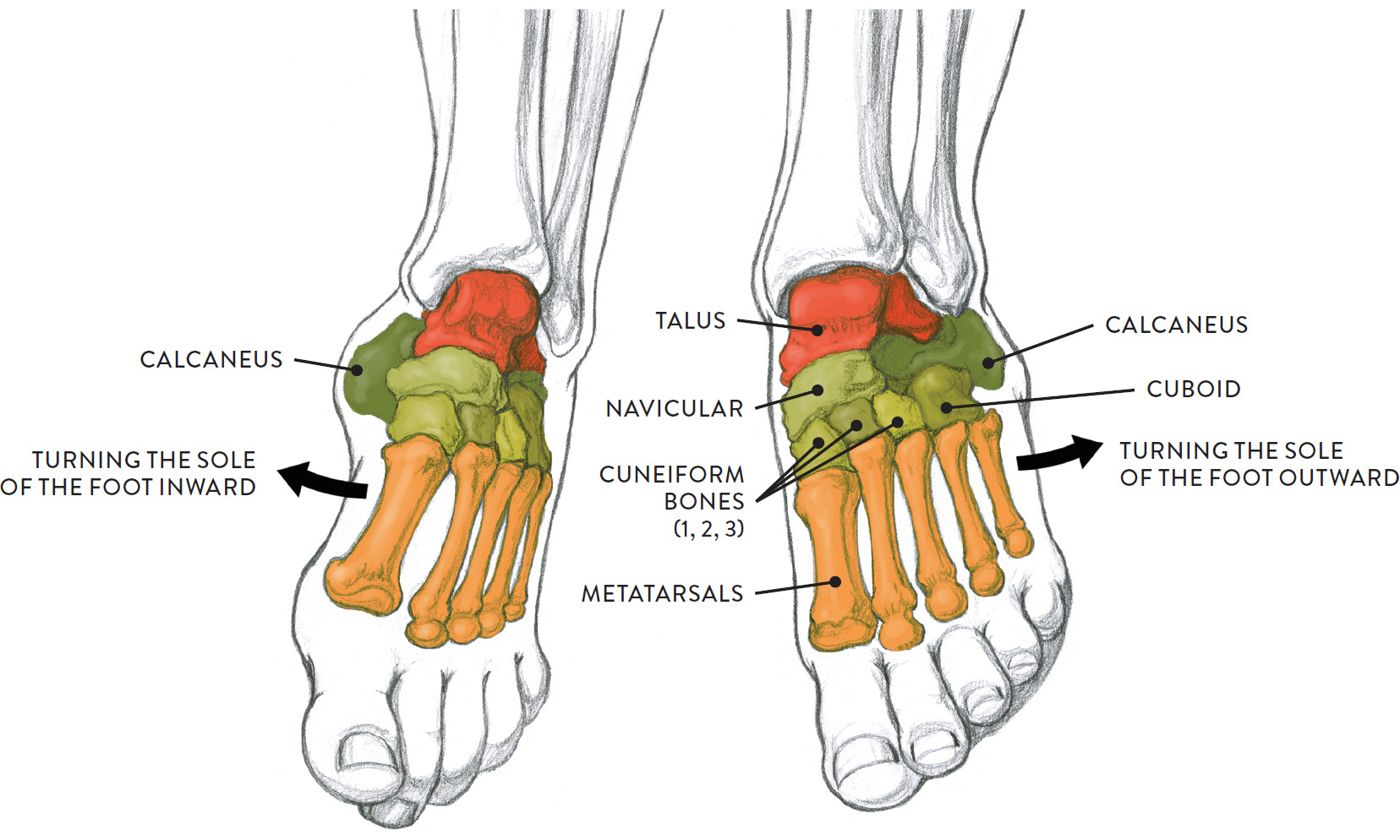
LEFT: Inversion of left foot
RIGHT: Eversion of left foot
The two main types of toe joints are the metatarsophalangeal joints (MTP joints) and the interphalangeal joints (IP joints). The movements of the toes, while not as dynamic as those of the fingers, are nonetheless important in the gait mechanics of walking, running, and other actions. When, in walking, the foot moves off the ground and swings in a forward direction, the toes extend upward and spread slightly to avoid being dragged against the ground. As the foot lands, the toes flex or bend and then “grip” the ground as a stabilizing maneuver.
The metatarsophalangeal joints (pron., MET-a-TAR-so-fa-lan-GEE-al), or MTP joints, are the joints between the heads of the metatarsals and the bases of the phalanges (toe bones). They are considered ellipsoid/condyloid joints.
The interphalangeal joints of the foot (pron., IN-ter-fa-lan-GEE-al), or IP joints, are the joints between the toe bones (phalanges) and are considered hinge joints.
Movements at these joints include abduction and adduction (spreading the toes away from the midline of the foot and then bringing them back together) and flexion and extension (bending and straightening the toes). These actions are shown in the drawings Abduction and Adduction of Toes at the MTP Joint and Flexion and Extension of Toes at the MTP and IP Joints.
ABDUCTION AND ADDUCTION OF TOES AT THE MTP JOINT
Ellipsoid/condyloid joint action
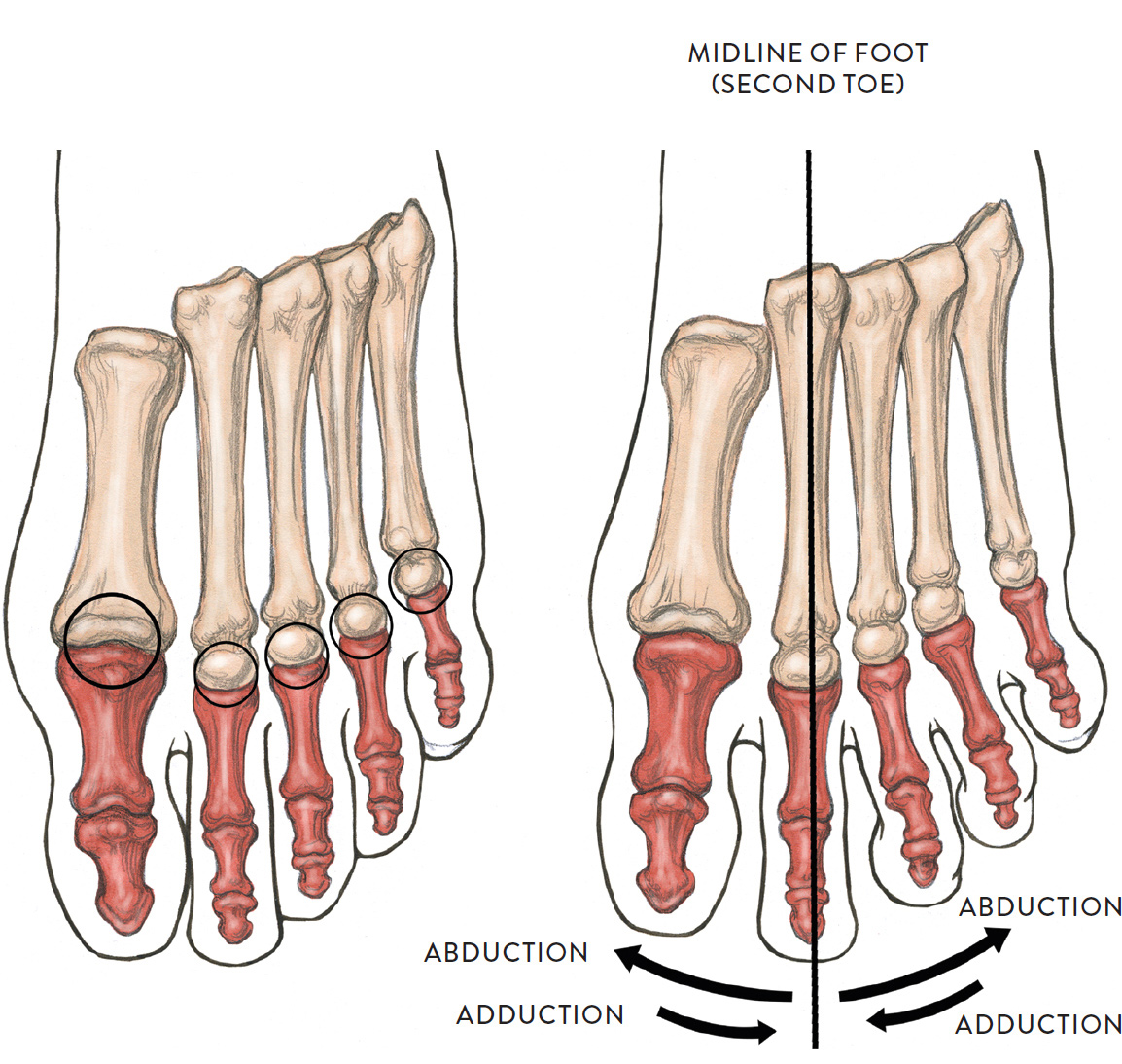
Superior view of left foot
Circles indicate the MTP joints and the ellipsoid/condyloid joints
LEFT: Neutral position of toes
RIGHT: Toes moving at the MTP joint
Abduction is the movement of the great toe and the third, fourth, and fifth toes away from the second toe (midline). Adduction is the reverse of this action.
FLEXION AND EXTENSION OF TOES AT THE MTP AND IP JOINTS
Hinge joint action
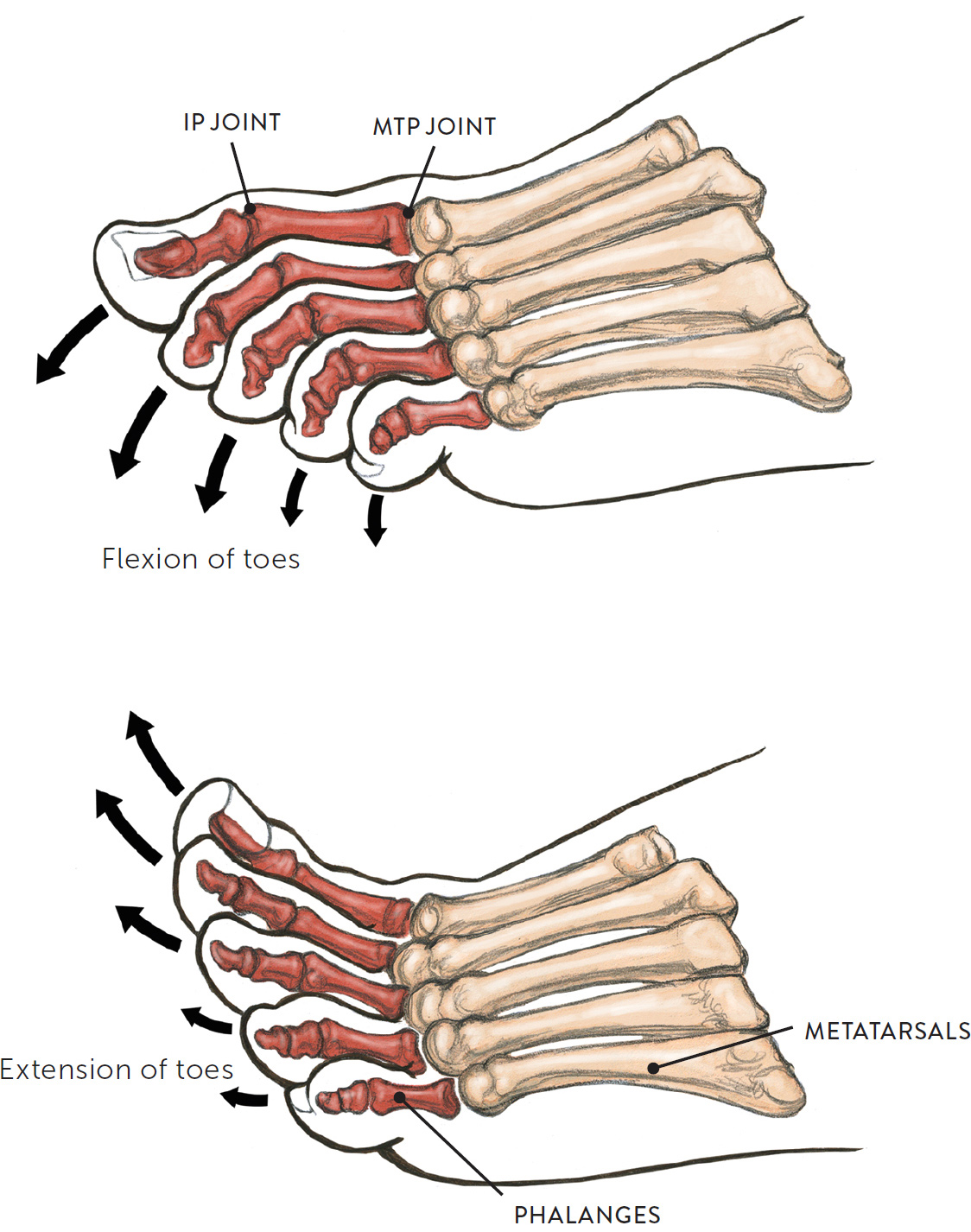
Lateral view of left foot
SITTING ÉCORCHÉ FIGURE
Graphite pencil and colored pencils on light toned paper.