CCEA GCSE Biology - Denmour Boyd, James Napier 2017
Unit 2
Reproduction, fertility and contraception

Specification points
This chapter covers sections 2.3.1 to 2.3.7 of the specification. It is about the male and female reproductive systems, pregnancy, sex hormones, the menstrual cycle, infertility and contraception.
Reproduction
Living organisms need to be able to reproduce or they would no longer exist. Humans, like most animals, carry out sexual reproduction. Sexual reproduction involves the joining together of two gametes — the sperm and the egg (ovum).
The male and female reproductive systems
The male reproductive system
The male reproductive system makes sperm (the male gamete) and is adapted to deliver the sperm into the female reproductive system.
Figure 11.1 shows the male reproductive system and describes the role of each part.
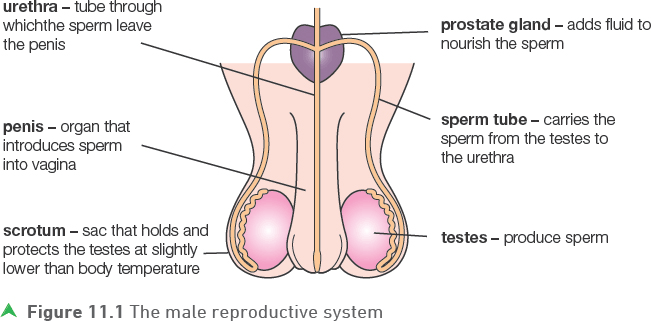
When a man and a woman have sex they are in intimate contact and as a consequence the man’s penis increases in size and becomes firmer. This enables him to place his penis into the vagina of the woman. During ejaculation, sperm is released by reflex action into the female.
Sperm are cells that are highly adapted for their function. They have a flagellum (tail) that allows the sperm to swim to meet the egg. Sperm (and egg cells) are also adapted in being haploid.
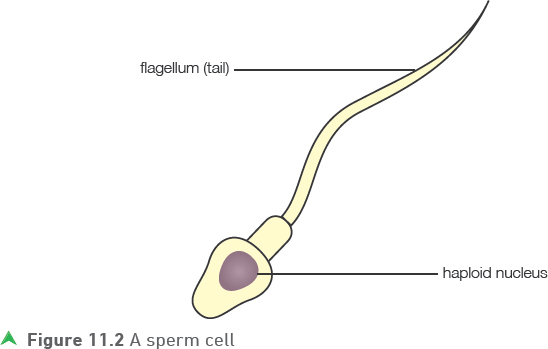
![]()
Sperm also have many mitochondria for energy production.
The female reproductive system
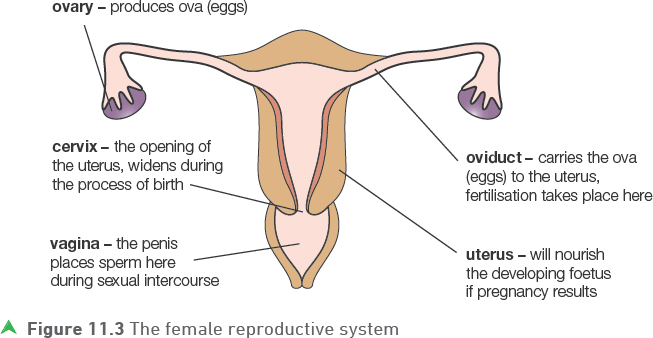
The female reproductive system is the part of the body that makes and releases eggs (ova). Additionally, if a sperm joins with an egg and pregnancy results, the embryo and foetus are protected and nourished within the female reproductive system until birth.
Figure 11.3 shows the female reproductive system and describes the role of each part.
Test yourself
1 What is the role of the prostate gland in the male reproductive system?
2 Name the part of the female reproductive system that produces eggs.
3 In which part of the female reproductive system does fertilisation take place?
Show you can
Describe the path of a sperm from where it is produced until it leaves the male body.
Following sexual intercourse, the male sperm cell is able to swim out of the vagina, through the cervix and uterus and into the oviduct where the sperm and egg can fuse (join).
Fertilisation and pregnancy
If a sperm and an egg (ovum) meet and fuse (join) in an oviduct, fertilisation will result. Fertilisation involves the haploid nuclei of the sperm and egg fusing and restoring the diploid (normal chromosome number) condition. The fertilised egg is the first cell (zygote) of the new individual.
The zygote divides by mitosis and grows into a ball of cells referred to as an embryo that develops further as it travels down the oviduct.
Tip
It is important that all gametes are haploid — if they weren’t then every time fertilisation takes place the chromosome numbers in a cell would double!
When the embryo enters the uterus, it sinks into the thick lining that has developed inside the uterus wall, becomes attached and receives nourishment (implantation).
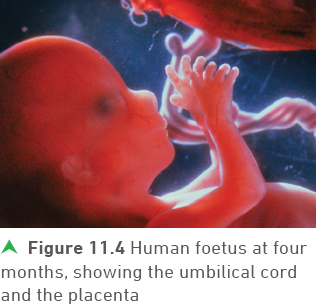
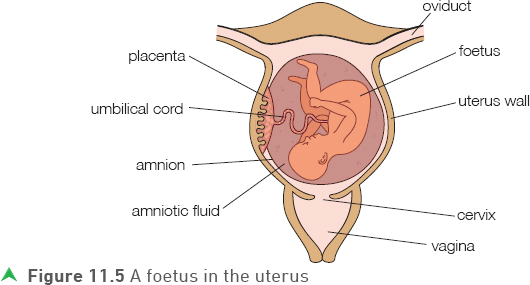
At the point where the embryo begins to develop in the uterus lining, the placenta and umbilical cord form. A protective membrane, the amnion, develops around the embryo, as shown in Figure 11.5. It contains a fluid, the amniotic fluid, within which the growing embryo develops. This fluid cushions the delicate developing embryo, which increasingly differentiates into tissues and organs. The embryo is referred to as a foetus after a few weeks when it begins to become more recognisable as a baby.
Tip
Although the male can release millions of sperm into the female’s vagina during sex, only one sperm is involved in producing a zygote. Most of the sperm do not even make it into the uterus!
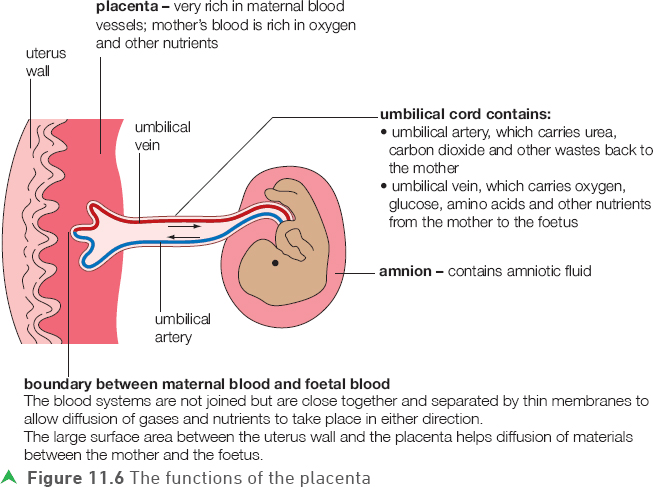
Obviously the foetus cannot breathe when in the amniotic fluid (its lungs will not be developed enough anyway in the early stages), so during pregnancy useful materials including oxygen and dissolved nutrients (for example amino acids and glucose) pass from the mother to the foetus through the placenta and umbilical cord. Waste excretory materials (including carbon dioxide and urea) pass from the foetus back to the mother.
The placenta and umbilical cord in more detail
Figure 11.6 shows the very close relationship between the blood vessels of the uterus and the blood vessels in the placenta.
Tip
The placenta is highly adapted for diffusion as it has a very large surface area at the point of contact with the uterine lining.
![]()
Tip
The villi are important in further increasing the surface area over which diffusion can take place between the mother and the placenta.
The surface area between the uterine wall and the placenta is further increased by small villi (extensions) in the placenta that extend into the uterus wall.
Sex hormones and secondary sexual characteristics
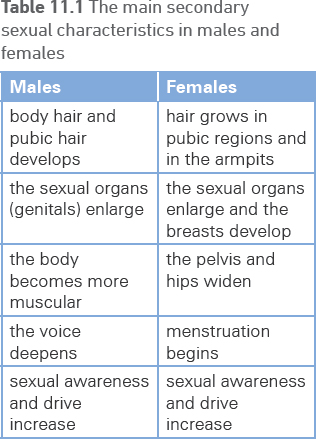
Testosterone (produced by the testes in males) and oestrogen (produced by the ovaries in females) are important hormones in overall sexual development. One effect they have is the development of the secondary sexual characteristics that are a feature of puberty. The changes that occur in males and females are different but in both sexes they serve to prepare the body for reproduction, both physically and by increasing sexual awareness and drive.
The main secondary sexual characteristics produced by testosterone and oestrogen are summarised in Table 11.1.
The menstrual cycle
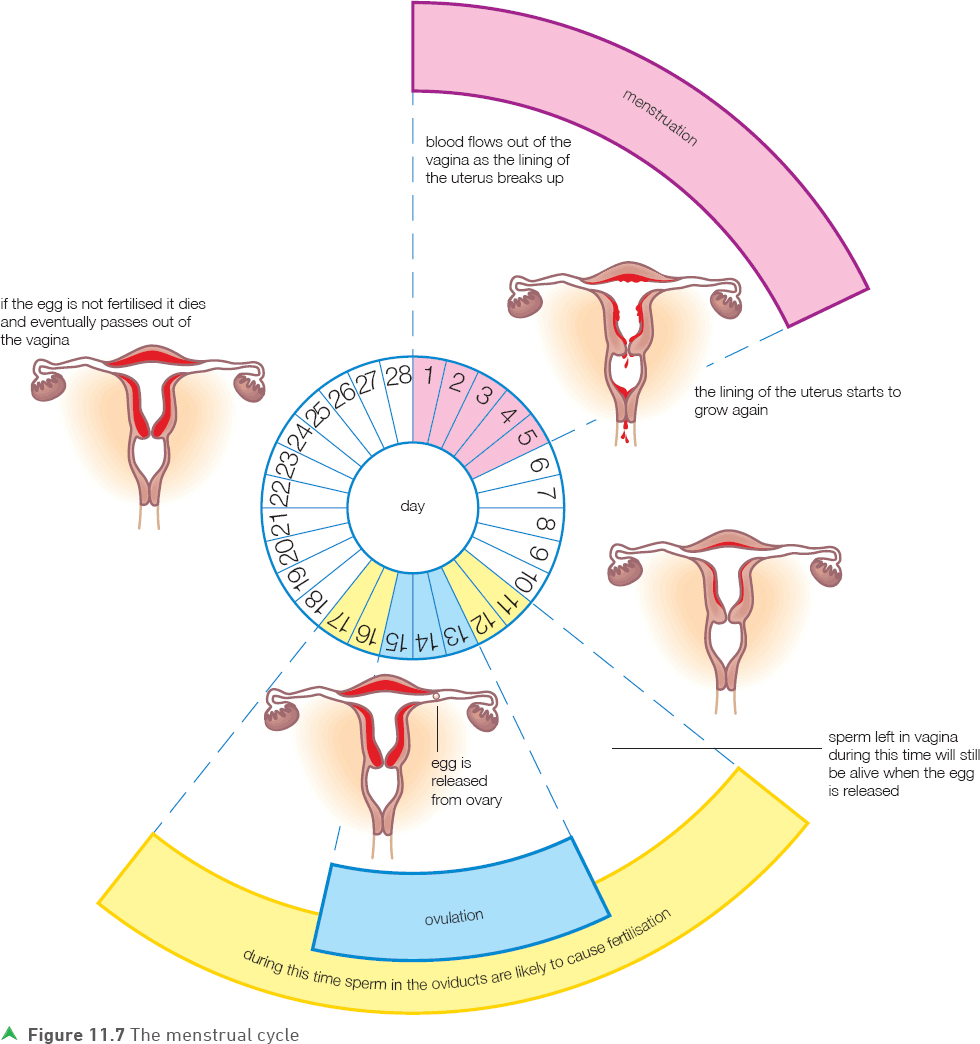
The menstrual cycle, shown in Figure 11.7, occurs in females from puberty until the end of reproductive life (usually sometime between the ages of 45 and 55). Each menstrual cycle lasts about 28 days. It is a cyclical event with the release of an ovum, the development of a thick lining on the uterus wall, and the breakdown of this lining (menstruation) occurring in each cycle. The purpose of the menstrual cycle is to prepare the reproductive system for pregnancy by controlling the monthly release of an egg and renewing and replacing the uterine lining.
The menstrual cycle is controlled by a number of female hormones. One of the most important hormones is oestrogen. At the start of each menstrual cycle (the onset of bleeding, which we call day 1), the level of oestrogen is low. As the cycle progresses the level of oestrogen rises. It peaks in the middle of the cycle, causing the release of an egg (ovulation). Another very important hormone is progesterone. The level of progesterone is also low during menstruation and peaks in the days following ovulation. The role of the progesterone is to build up and maintain the thick uterine lining (and the subsequent development of the placenta and other structures associated with pregnancy) should pregnancy occur. Oestrogen is also important in the initial buildup of the uterine lining.
Tip
Oestrogen has two main functions in the menstrual cycle: the initial repair and buildup of the uterus wall and the stimulation of ovulation.
Progesterone is responsible for the buildup and maintenance of the uterus lining.
If pregnancy does not occur, the levels of oestrogen and progesterone drop towards the end of the cycle and this causes menstruation to occur. Then the cycle begins again.
Tip
Figure 11.7 shows the times in the menstrual cycle during which fertilisation of an egg can occur. You should know that fertilisation can occur if sex takes place in the days immediately before, or immediately after, ovulation.
Test yourself
4 Give two functions of oestrogen in the menstrual cycle.
5 What is the function of progesterone in the cycle?
Show you can
Use information provided in earlier sections to draw a diagram to show how the level of oestrogen changes throughout the menstrual cycle.
![]()
Fertility problems (infertility) and their treatment
Some people have problems that prevent them having children (fertility problems). Reasons include:
• the failure of ovaries to produce eggs
• the oviducts may be blocked or twisted, possibly due to infection
• complications of some sexually transmitted infections
• the lining of the uterus does not develop properly to enable implantation to occur
• the vagina may be hostile to sperm entering, for example the lining may be too thick or too acidic
• males may not produce enough sperm or the sperm may not be healthy — this can be affected by smoking or drinking alcohol in excess
• impotence in males.
There are a number of treatments that can be used to improve the chances of having a baby in someone with a fertility problem. The actual treatment used depends on the nature of the problem.
Fertility drugs (hormone treatment)
These are given to the woman to increase the production of eggs. This may solve the problem if low egg production is the issue but if there are other problems such as blocked oviducts then in-vitro fertilisation may be necessary.
In-vitro fertilisation (test-tube babies)
Normally women opting for in-vitro fertilisation are given fertility drugs so that several eggs are produced. The eggs are collected from the ovaries surgically. Sperm from a donor (usually the husband or partner) is collected and the sperm and eggs are mixed in the laboratory. Following fertilisation, embryos are placed in the mother’s uterus (she will have undergone hormonal treatment to ensure her uterus lining is ready). If the process is successful, an embryo (or possibly more than one) will implant in the uterus lining. Usually only a small number of embryos are placed in the mother’s uterus to give a balance between ensuring a successful pregnancy and avoiding multiple births.
Tip
Two or more eggs (rather than one) are often used in each cycle of in-vitro fertilisation. This is because the process is very complicated and expensive and the use of more than one egg increases the probability of success.
Fertility research and treatment is a controversial area. It is now possible to screen embryos to check for abnormalities and even to check the sex of embryos before they are placed in the woman’s uterus.

Test yourself
6 Give two causes of infertility in men.
7 Why are fertility drugs used to treat female infertility?
Show you can
Explain why women undergoing fertility treatment may need two different types of hormone treatment.
Contraception — preventing pregnancy
Many people want to have sex but do not want to have children at that particular time. Pregnancy can be prevented by contraception.

Methods of contraception
There are three main types of contraception: mechanical, chemical and surgical. Examples of each and an explanation of how they work, together with their main advantages and disadvantages, are given in Table 11.2.
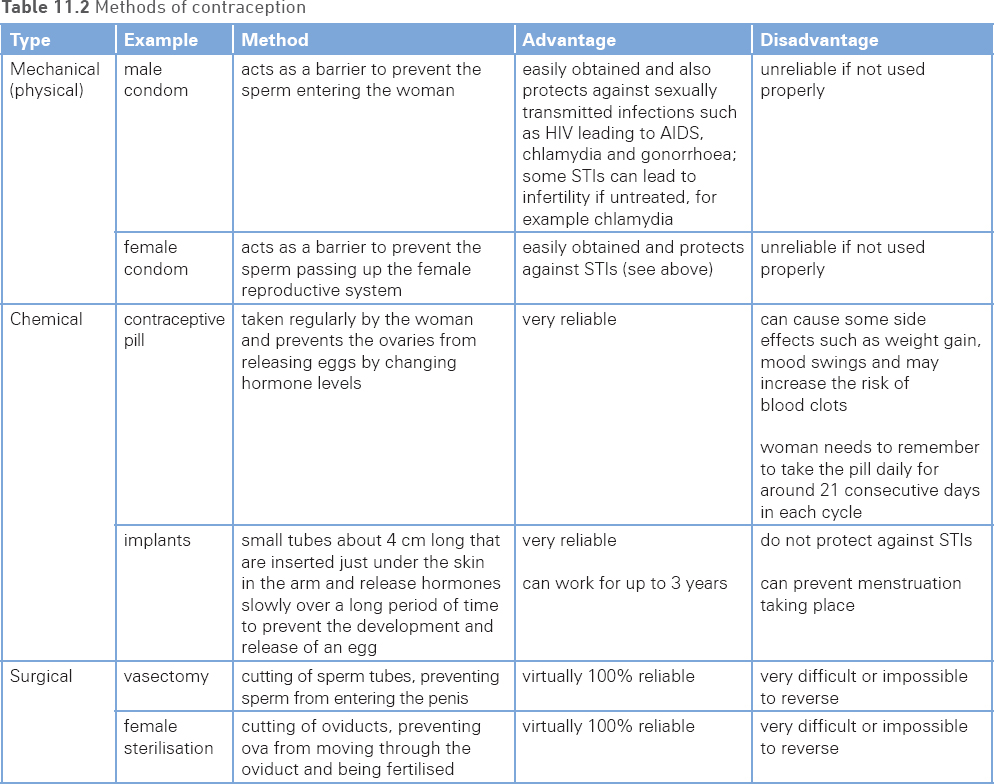
You need to be able to explain how each method of contraception works, its main advantage(s) and disadvantage(s).
Tip
The actual hormones used in different types of contraceptive pill and implants vary but they are almost always oestrogen and/or progesterone.
Example
Explain how female sterilisation works and give one advantage and one disadvantage.
Answer
Both oviducts are cut and this prevents eggs (and sperm coming in the other direction) from passing beyond this point so fertilisation cannot occur. The main advantage is that it is virtually 100% reliable. The disadvantage is that it is very difficult or impossible to reverse.
Tip
Do not confuse contraceptive implants with contraceptive patches. Patches work for a much shorter time than implants and they work in a slightly different way.
Some people are opposed to contraception but may want to reduce their chances of having children — often because they have a large family already. They can do this by avoiding having sex around the time when the woman releases an ovum each month — this has been called the rhythm or natural method of contraception.
Some people choose this method for religious or ethical reasons but it is much less effective than contraception. In many women the menstrual cycle is irregular, making it difficult to know exactly when an egg is being released.
Test yourself
8 Describe how mechanical contraceptives work.
9 Give one advantage of using a mechanical contraceptive.
10Give one disadvantage of using a mechanical contraceptive.
Show you can
Explain why doctors may be unwilling to sterilise an unmarried 25-year-old who has no children.
Practice questions
1 Figure 11.10 represents the female reproductive system.
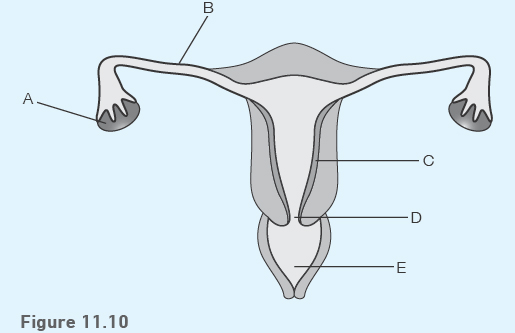
a) Identify parts A and B.
(2 marks)
b) Give the letter on the diagram that represents where:
i) fertilisation can take place
ii) an embryo (ball of cells) can implant
iii) male sperm is deposited during sex.
(3 marks)
2 a) Sperm have a haploid nucleus.
i) Describe what is meant by the term haploid.
(1 mark)
ii) Why is it important that sperm have a haploid nucleus?
(1 mark)
b) Figure 11.11 summarises what happens to the zygote following fertilisation.
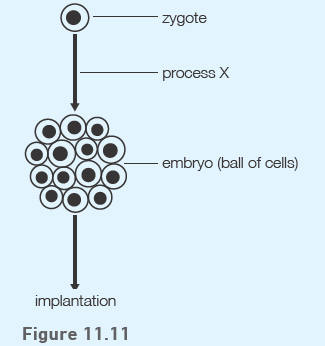
i) Name process X that leads to a zygote forming a ball of cells.
(1 mark)
ii) Describe what happens to the ball of cells during and after the process of implantation.
(2 marks)
3 Figure 11.12 represents the menstrual cycle.
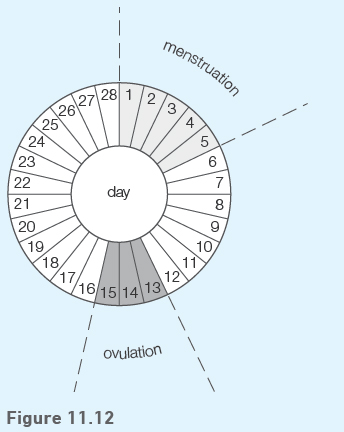
a) Describe one change that would occur in the uterus between day 6 and day 12.
(1 mark)
b) Name the hormone responsible for this change.
(1 mark)
c) Explain fully why it would be possible for a female to get pregnant if sex took place on day 16.
(2 marks)
4 a) Suggest the effect a blockage in one of the oviducts will have on the chances of a female becoming pregnant. Explain your answer.
(3 marks)
b) Figure 11.13 represents the male reproductive system.
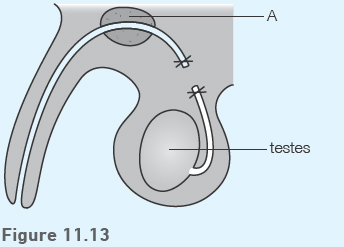
i) Name the gland labelled A.
(1 mark)
ii) Name the method of contraception shown.
(1 mark)
iii) Using the diagram, explain fully how this method prevents pregnancy.
(2 marks)
iv) Give one disadvantage of this method of contraception.
(1 mark)