Biology of Humans
8a. Drugs and the Mind
In the previous chapters we learned how neurons function and form circuits that function as a nervous system. In this chapter, we will consider how drugs affect the nervous system and alter our state of mind. We will see why the use of some drugs leads to a need to continue using the drug. Then we will take a look at some of the more common mind-altering drugs.
Psychoactive Drugs and Communication between Neurons
A drug that alters one's mood or emotional state is often described as a psychoactive drug. The mind-altering effects of these drugs result from their ability to cross the blood-brain barrier, a membranous structure that prevents most substances from reaching the brain. The drugs then interfere with the communication between nerve cells. As you learned in Chapter 7, neurons communicate with one another using neurotransmitters. Neurotransmitters are released by one neuron, diffuse across a small gap between neurons, and bind to specific receptors on another neuron, triggering changes in the activity of the second neuron. Under normal conditions, the action of the neurotransmitter is stopped almost immediately after its message is conveyed because the neurotransmitter is either broken down by enzymes, reabsorbed into the cell that released it, or simply diffuses away.
A psychoactive drug may alter this communication between neurons in any of several ways (Figure 8a.1). A drug may stimulate the release of a neurotransmitter and enhance the response of the receiving neuron. It may inhibit the release of a neurotransmitter and thus dampen the response of the receiving neuron. Or it may increase and prolong the effect of a neurotransmitter by delaying its removal from the gap between neurons. If the drug is chemically similar to the natural neurotransmitter, the drug may bind to the receptor and affect the activity of the receiving neuron in the same manner as the neurotransmitter, increasing its effect. Alternatively, its binding to the receptor may prevent the neurotransmitter from acting at all.
One of the problems with using psychoactive drugs is that the user may develop some level of psychological or physical dependence on the drug. Before we consider the drugs themselves, let's consider the concepts of tolerance and dependence.
· Alcohol is a legal psychoactive drug.
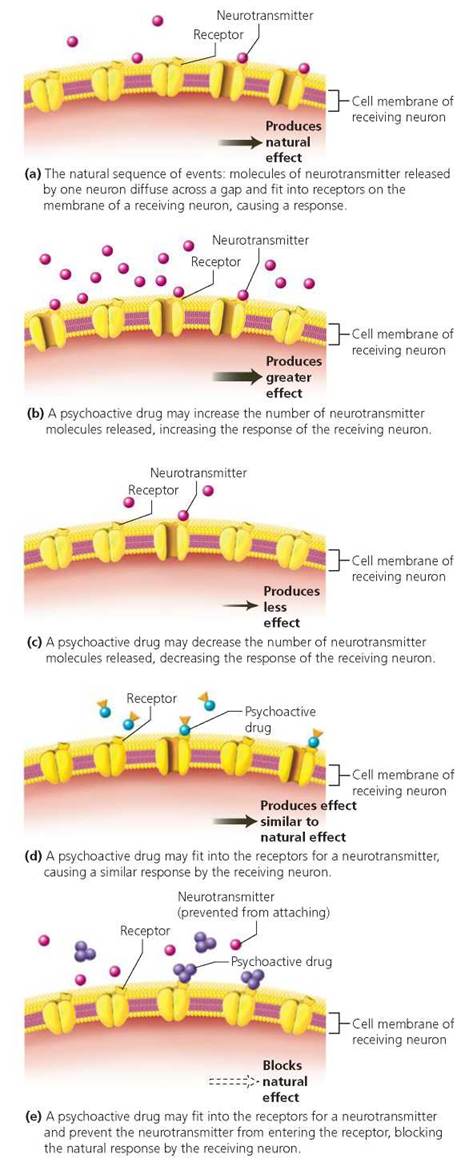
FIGURE 8a.1. Psychoactive drugs alter a person's mental state by affecting communication between neurons.
Stop and think
Why would a drug that increases the amount of a particular neurotransmitter released and a drug that slows the removal of that neurotransmitter from the synapse have the same effects?
Drug Dependence
Tolerance is a progressive decrease in the effectiveness of a drug in a given person. As tolerance to a particular drug develops, a person must take larger or more frequent doses to produce the same effect. Tolerance develops partly because the body naturally steps up its production of enzymes that break down the drug, disabling it from having a continued effect, and partly because of changes in the nerve cells themselves that make them less responsive to the drug. Cross-tolerance occurs when tolerance to one drug results in a lessened response to another, usually similar drug. If a person abuses codeine, for instance, tolerance develops not only for codeine but also for other drugs that have similar effects on the nervous system, such as morphine and heroin.
A loose definition of dependence might be, "It is what causes a person to continue using a drug." More precisely, dependence is the state in which the drug is necessary for physical or psychological well-being. A person who is physically dependent on a drug experiences physical withdrawal symptoms when the drug use is stopped.
Certain drugs encourage users to continue using them because the drugs stimulate the "pleasure" centers in the limbic system of the brain (see Chapter 8). Just as an animal with electrodes implanted in the pleasure center will quickly learn to press a lever to stimulate this brain region to the point of exhaustion, an animal will learn to press a lever to self-administer a dose of a drug that stimulates the pleasure center. Drugs that stimulate the pleasure center include cocaine, amphetamine, morphine, and nicotine.
In the following discussions of psychoactive drugs, we will consider their habit-forming potential as well as possible health risks associated with their use.
Alcohol
In every alcoholic drink, the alcohol is ethanol. Ethanol is produced as a by-product of fermentation, when yeast cells break down sugar to release energy for their own use. The taste of the beverage is determined by the source of the sugar, which comes from the fruit or vegetable that is fermented. For example, grapes are fermented to make wine, grain (barley, oats, rice, wheat, or malt) to make beer, and malt to make scotch.
The effects of alcohol on a person's behavior depend on the blood alcohol level, which is measured as the number of grams of alcohol in 100 ml of blood. One gram of alcohol in 100 ml of blood is a blood alcohol level of 1%. The blood alcohol level in a person depends on several factors, including how much alcohol is consumed; how rapidly it is consumed (over what period of time); and its rate of absorption, distribution, and metabolism.
A "drink" can mean different things to different people. For some it is a can of beer, for others a glass of wine, and for others it is a scotch on the rocks. The amount of pure ethanol in the beverage varies tremendously. Natural fermentation, the process used to make beer and wine, cannot yield more than 15% alcohol, because the alcohol kills the yeast cells producing it. In contrast, liquor (distilled spirits) is produced by distillation, a process that concentrates the alcohol. The alcohol content of distilled spirits is measured as "proof." One degree of proof equals 0.5% alcohol. Most distilled spirits (vodka, gin, scotch, whiskey, rum, brandy, and cognac) are 80 proof, which means they contain 40% alcohol. But some brands are 90 proof (45% alcohol) or even 100 proof (50%). So, a small 3 oz1martini, which contains only distilled spirits and therefore about 1.2 oz of alcohol, is actually more intoxicating than a larger 8 oz mug of beer, which contains about 0.4 oz of alcohol.
The differences in the alcohol content of beverages are reflected in the standard amounts in which they are served as drinks. Generally, the standard drink contains 0.5 oz of pure ethanol. A standard drink is one bottle or can of beer; a glass of wine; or a jigger (1.5 oz) of 80 proof distilled spirits, such as gin, whisky, vodka, or scotch (alone or in combination with another beverage) (Figure 8a.2).
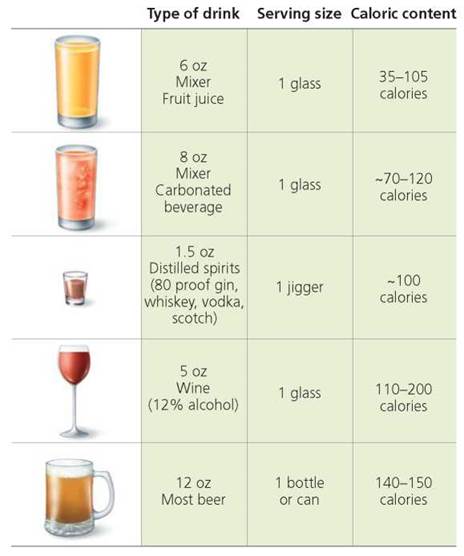
FIGURE 8a.2. A standard drink contains 0.5 oz of alcohol. Different types of alcoholic beverages vary in their alcohol content, so the size of a standard drink varies with its alcoholic content.
Absorption
The intoxicating effects of alcohol begin when it is absorbed from the digestive system into the blood and is delivered to the brain. As a rule, the absorption rate of alcohol depends on the concentration of alcohol in the drink: the higher the concentration, the faster the rate of absorption. So wine, beer, or distilled spirits diluted with a mixer will be absorbed more slowly than pure liquor. The choice of mixer also influences the rate of absorption. Carbonated beverages increase the absorption rate because of the pressure of the gas bubbles.
Although very few substances are absorbed across the walls of the stomach, about 20% of the alcohol consumed is absorbed there. The remaining alcohol is absorbed through the intestines. Because alcohol can be absorbed from the stomach, a person begins to feel the effects of a drink quickly, usually within about 15 minutes. The presence of food in the stomach slows alcohol absorption because it dilutes the alcohol, covers some of the stomach lining through which alcohol would be absorbed, and slows the rate at which the alcohol passes into the intestines.
Distribution to All Body Tissues
Ethanol is a small molecule that is soluble in both fat and water, so it is distributed to all body tissues. Therefore, overall body size affects one's blood alcohol level and the degree of intoxication. A large person would have a lower blood alcohol level and as a result be less intoxicated than would a small person after they both consumed the same amount of alcohol (Figure 8a.3).
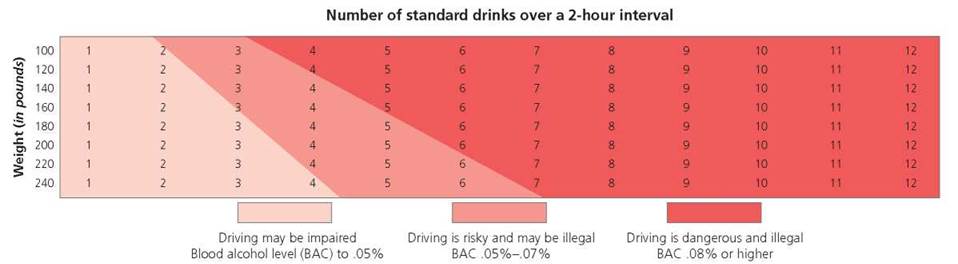
FIGURE 8a.3. Alcohol consumption can impair driving. The blood level of alcohol depends on both the number of drinks consumed and body size. After they consume the same amount of alcohol, a small person has a higher blood alcohol level than a large person does. The blood level of alcohol determines the effect on the nervous system.
If a 140 lb man has three beers over a 2-hour interval, in what range is his blood alcohol level? If a 180 lb man has three beers over a 2-hour interval, in what range is his blood alcohol level?
Probably over .05%; Probably under .05%.
Rate of Elimination
Ninety-five percent of the alcohol that enters the body is metabolized (broken down) before it is eliminated. Most of that metabolism occurs in the liver, which converts alcohol to carbon dioxide and water. The rate of metabolism is slow, about one-third of an ounce of pure ethanol per hour.
In practical terms, it takes slightly more than an hour for the liver to break down the alcohol contained in one standard drink—a can of beer or a glass of wine. Because alcohol cannot be stored anywhere in the body, it continues to circulate in the bloodstream until it is metabolized. Therefore, if more alcohol is consumed in an hour than is metabolized, both the blood alcohol level and the degree of intoxication increase along with consumption.
There is no way to increase the rate of alcohol metabolism by the liver and, therefore, no way to sober up quickly. The caffeine in a cup of coffee may slightly counter the drowsiness caused by alcohol, but it does not reduce the level of intoxication. Furthermore, because muscles do not metabolize alcohol, exercise does not help, either. Walking around the block will not make a person sober, nor will a cold shower.
A small amount of alcohol, about 5%, is eliminated from the body unchanged through the lungs or in the urine. Alcohol eliminated from the lungs is the basis of the breathalyzer test that may be administered by law enforcement officers who want an on-the-spot sobriety check.
Health-Related Effects
Because alcohol has a negative effect on virtually every organ of the body, people do not have to be alcoholics for alcohol to impair their health. In this section we look at some ways that alcohol affects the body.
Nervous system. Many people believe that alcohol is a stimulant, but it is actually a depressant. In other words, it slows down the activity of all the neurons of the brain, beginning with the higher cortical, or "thinking," centers. Alcohol often is mistakenly thought to be a stimulant because it depresses the inhibitory neurons first, allowing the excitatory ones to take over. As alcohol removes the "brakes" from the brain, normal restraints on behavior may be lost. Release from inhibitory controls also tends to reduce anxiety and often creates a sense of well-being. However, discrimination, control of fine movements, memory, and concentration are gradually lost as well.
The brain centers for balance and coordination are affected next, causing a staggering gait. Numbed nerve cells send slower messages, resulting in slower reflexes. Eventually, the brain regions responsible for consciousness are inhibited, causing a person to pass out. Still higher concentrations of alcohol can cause coma and death from respiratory failure.
Liver. Excessive alcohol consumption damages the liver, an organ that performs many vital functions in the body. Severe damage to the liver is a serious threat to life. Alcohol is metabolized in the liver before fats are, which allows fats to accumulate in liver cells. Four or five drinks daily for several weeks are enough to cause fat accumulation to begin. At this early stage, however, the liver cells are not yet harmed; and with abstinence, they can be restored to normal. With continued drinking, the accumulating fat causes liver cells to enlarge, sometimes so much that the cells rupture or form cysts. The accumulated fat in liver cells also reduces blood flow through the liver, causing inflammation known as alcoholic hepatitis. Signs of alcoholic hepatitis include fever and tenderness in the upper abdominal region. Gradually, fibrous scar tissue may form, a condition known as cirrhosis, which further impedes blood flow and impairs liver functioning. Cirrhosis can lead to intestinal bleeding, kidney failure, fluid accumulation, and eventually death, if drinking continues. Indeed, cirrhosis of the liver, the ninth leading cause of death in the United States, is most often caused by alcohol abuse.
Cancer. A person who drinks heavily is at least twice as likely to develop cancer of the mouth, tongue, or esophagus than is a nondrinker. Evidence also exists that the combined risk of cancer from both drinking and smoking cigarettes is greater than the sum of the risks caused by either drinking or smoking alone.
Heart and blood vessels. Here's the good news: Moderate amounts of alcohol can be good for the heart. Teetotalers are more likely to suffer heart attacks than are persons who drink moderately, say a drink a day. One reason may be that the relaxing effect of alcohol helps to relieve stress. But alcohol also seems to raise the levels of the "good" form of a cholesterol-carrying particle—HDL—in the blood (discussed in Chapters 12 and 15a). This form of cholesterol reduces the likelihood that fats in the blood will be deposited in the walls of blood vessels, clog the vessels, and reduce the blood supply to vital organs such as the heart or brain. In addition, moderate amounts of alcohol reduce the likelihood that blood clots will form when they should not. Such clots can cause a heart attack by blocking blood vessels that nourish the heart muscle. Thus, persons who imbibe moderately generally live longer than nondrinkers.
When alcohol is consumed in more than moderate quantities, however, it damages the heart and blood vessels. It weakens the heart muscle itself, reducing the heart's ability to pump blood. It also promotes the deposit of fat in the blood vessels, making the heart work harder to pump blood through them. Consuming more than moderate quantities of alcohol may also elevate blood pressure substantially. Together, these effects—damage to heart muscle, blood vessels clogged with fatty materials, and high blood pressure—can enlarge the heart to twice its normal size (Figure 8a.4).

FIGURE 8a.4. The alcoholic's heart, on the right, is nearly twice the normal size.
What would you do?
Fetal alcohol syndrome (FAS) is a pattern of growth abnormalities and birth defects common among children of women who drink during pregnancy. These include mental retardation, growth deficiency, and characteristic facial features, although all the characteristics of FAS are not always present in any one infant. Recent studies suggest that a fetus' genes may be permanently altered by exposure to alcohol during development. Considering these long-term effects on the child, do you think that there should be legal consequences for women who drink during pregnancy?
Alcoholism. Alcohol is a legal drug, and alcoholism is America's number one drug problem. Alcoholics can be young or old, rich or poor, and of any race, economic status, or profession. Because there is no such thing as a typical alcoholic, alcoholism can be difficult to identify.
Different alcoholics have different drinking patterns. Some binge, and some chronically overindulge. But what they all share is a loss of control over their drinking. When an alcoholic takes the first sip of alcohol, he or she cannot predict how much or how long the drinking episode will continue.
Marijuana
Marijuana is the most widely used illegal drug in the United States today. It consists of the leaves, flowers, and stems of the Indian hemp plant, Cannabis sativa. The principal psychoactive ingredient (the component that produces mind-altering effects) is delta-9-tetrahydrocannabinol, or THC.
The effects of marijuana depend on the concentration of THC and on the amount consumed. In small to moderate doses, THC produces feelings of well-being and euphoria. In large doses, THC can cause hallucinations and paranoia. Anxiety may even reach panic proportions at very high doses.
Marijuana is not addicting in the sense of producing severe, unpleasant withdrawal symptoms. Nonetheless, a withdrawal syndrome has been identified. It includes symptoms such as restlessness, irritability, mild agitation, insomnia, nausea, and cramping. Withdrawal symptoms are not common and, if they do occur, are usually relatively mild and short-lived.
THC Receptors in the Brain
Researchers are just beginning to understand how marijuana affects the brain. When THC binds to certain receptors on nerve cells, it triggers a cascade of events that ultimately lead to the "high" that the user experiences (Figure 8a.5).2 After discovering the receptors, researchers quickly set about looking for the neurotransmitter that normally binds to them, reasoning that the receptors did not evolve millions of years ago just in case someone would someday decide to smoke marijuana. The researchers sorted through thousands of chemicals in pig brains to find one that would bind to THC receptors. The first one to be identified was a hitherto unknown chemical messenger they named anandamide, after the Sanskrit word meaning "internal bliss" (ananda). Anandamide functions as the brain's own THC. Its normal functions probably include the regulation of mood, memory, pain, appetite, and movement. In addition to mimicking anandamide, THC seems to stimulate the release of dopamine in the reward pathways of the brain.
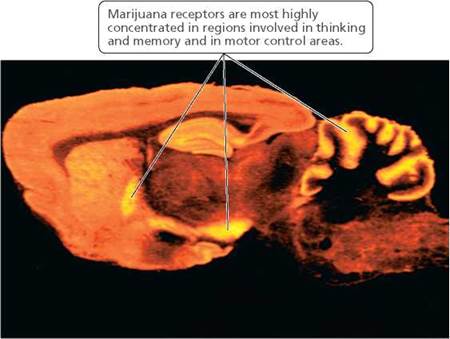
FIGURE 8a.5. The areas with marijuana receptors appear yellow in this photograph showing a section of a rat's brain.
Health-Related Effects of Long-Term Use
Marijuana is usually smoked. It should not be surprising, then, that the most clearly harmful effects of marijuana are on the respiratory system. However, the damage, it seems, is done by the residual materials in the smoke and not by the THC itself. Compared to the daily consumption of cigarettes by tobacco smokers, marijuana smokers smoke fewer joints (marijuana cigarettes) per day. However, compared with a regular cigarette, a joint has 50% more tar, which contains cancer-causing chemicals. Also, marijuana smoke is usually inhaled more deeply and held within the lungs longer. As a result, three times as much tar is deposited in the airways, and five times as much carbon monoxide is inhaled than with a normal cigarette. Carbon monoxide prevents red blood cells from carrying needed oxygen to the cells of the body. The end result of prolonged smoking of marijuana is marked trauma to the respiratory system. Similar to cigarette smoke, marijuana smoke inflames air passages and reduces breathing capacity.
Another known effect of smoking marijuana is that it makes the heart beat faster, sometimes double its normal rate. In some people, marijuana also increases blood pressure. Either change increases the heart's workload and could pose a threat to people with preexisting cardiovascular problems, such as high blood pressure or atherosclerosis (fatty deposits in the arteries). Thus, although the risk is small, marijuana increases one's risk of immediate heart attack.
Some studies have shown that THC can interfere with reproductive functions in both males and females. At least some of these disturbances may result from the structural similarity between THC and the sex hormone estrogen. Males who smoke marijuana often have lower levels of the sex hormone testosterone and produce fewer sperm than do nonusers. Testosterone and sperm levels return to normal when THC is cleared from the body.
The effects of marijuana on the female reproductive system are not clear. Although we know that THC interferes with ovulation in female monkeys, we know less about what it may do to human females. Some doctors, however, report menstrual problems and reproductive irregularities in women who smoke marijuana.
What would you do?
More than a dozen states have legalized marijuana for medical purposes, but controversy continues. How much research is enough, and how much credence should be given to anecdotal evidence? When people say they feel better, is that enough evidence that they do? What other factors should be considered? So, should marijuana be legalized for medical purposes? For testing purposes? What information would you want before voting on the legalization of marijuana for medical purposes?
Stimulants
Stimulants are drugs that excite the central nervous system (CNS; see Chapter 8). Here we'll look at three types of stimulants: cocaine, the amphetamines, and nicotine.
Cocaine
Cocaine is extracted from the leaves of the coca plant (Erythroxylon coca), which grows naturally in the mountainous regions of South America. When cocaine powder extracted from the plant is inhaled into the nasal cavity ("snorted"), it reaches the brain within a few seconds and produces an effect almost as intense as when a solution of cocaine is injected. Smoking the drug is an even more effective delivery route. Forms of cocaine that can be smoked—specifically, freebase and crack—are obtained by further extraction and purification of the coca plant.
When ingested in one of these ways, cocaine brings about a rush of intense pleasure, a sense of self-confidence and power, mental alertness, and increased physical vigor. It does so by increasing the levels of two "feel-good" neurotransmitters: dopamine and norepinephrine (Figure 8a.6). The euphoria is caused primarily by cocaine's effect on dopamine, a neurotransmitter used by nerve cells in the pleasure centers of the brain. Normally, dopamine is almost immediately reabsorbed into the nerve cell that released it, and its effect soon ceases. Cocaine, however, interferes with the reuptake of dopamine, thus increasing and prolonging dopamine's effect. Cocaine also increases the effects of another neurotransmitter, norepinephrine. Norepinephrine stimulates the effects of the sympathetic nervous system, the part of the nervous system that prepares the body to face an emergency. Thus, cocaine also triggers the responses that ready the body for stress: increased heart rate and blood pressure, narrowing of certain blood vessels, dilation of pupils, a rise in body temperature, and a reduction of appetite.
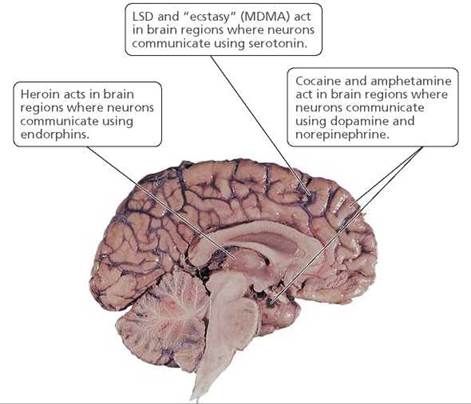
FIGURE 8a.6. The effects of certain drugs on the brain
The effects of cocaine are short-lived, lasting from 2 to 90 minutes depending on how the cocaine enters the body. When the high wears off, it is generally followed by a "crash," a period of deep depression, anxiety, and extreme fatigue. These uncomfortable feelings often produce a craving for more cocaine. The higher the high, the harder the crash, and therefore, the more intense the craving for more of the drug. Crack, which is estimated to be about 75% pure cocaine compared with the 10% to 35% purity of street cocaine, causes higher highs and lower crashes and therefore is extremely addicting.
Cardiovascular risks. Cocaine may cause heart attack or stroke, emergencies in which an interruption of blood flow deprives heart cells or brain neurons of oxygen and nutrients. One way that cocaine blocks blood flow is by constricting arteries. Thus, one way it produces heart attack is by causing spasms in the arteries supplying the heart. Blood flow to the heart can also be disturbed by irregularities in heartbeat. By disabling the nerves that regulate heartbeat, cocaine can cause disturbed heartbeat rhythms that result in chest pain and heart palpitations (that uncomfortable feeling of being aware of your heart beating). Cocaine use may even cause the heart to stop beating. In addition, cocaine increases blood pressure, which may cause a blood vessel to burst.
Respiratory risks. Stimulation of the CNS is always followed by depression. As the stimulatory effects of cocaine wear off, the respiratory centers in the brain that are responsible for breathing become depressed, or inhibited. Breathing may become shallow and slow and may stop completely. In short, cocaine use can cause respiratory failure that can lead to death.
Damage to the respiratory system as a result of cocaine use depends largely on how the drug is taken. If it is snorted, cocaine causes damage to the nerves, lining, and blood vessels of the nose. It can dry out the nose's delicate mucous membranes so that they crack and bleed almost continuously. Symptoms of a sinus infection—a perpetually runny nose and a dull headache spanning the bridge of the nose—are common. What is more alarming, the partition between the two nasal cavities may disintegrate. Because cocaine is a painkiller, considerable damage to the nose may occur before being discovered.
Smoking crack, on the other hand, damages the lungs and airways. The chronic irritation leads to bronchitis and may also cause lung damage from reduced oxygen flow into the lungs or blood flow through the lungs.
Amphetamines
Amphetamines are synthetically produced stimulants that closely resemble dopamine and norepinephrine (the same neurotransmitters whose levels are increased by cocaine). There are many forms of amphetamine, including dextroamphetamine and methamphetamine, also known as crystal meth. Metham-phetamine is illegally sold as a powder that can be injected, snorted, swallowed, or smoked. All amphetamines are stimulants of the CNS. Like cocaine, when active, amphetamines make the user feel good—exhilarated, energetic, talkative, and confident. They suppress appetite and the need for sleep. Amphetamines are active for longer periods than cocaine— hours as opposed to minutes.
Amphetamines can be swallowed in a pill or injected intravenously. One crystalline form of methamphetamine is smoked to produce effects similar to those of crack cocaine. Methamphetamine can produce hazardous effects, including blood vessel spasm, blood clot formation, insufficient blood flow to the heart, and accumulation of fluid in the lungs.
Amphetamines bring about their physical and psychological effects by causing the release of certain neurotransmitters, such as norepinephrine and especially dopamine. As a result, the drugs elevate blood pressure, increase heart rate, and open up airways in the lungs.
Tolerance to amphetamines develops (accompanied by simultaneous tolerance to cocaine) along with both physical and psychological dependence. Withdrawal symptoms include extreme fatigue, depression, and increased appetite. Also, the pleasurable feelings caused by amphetamine use can lead to a compulsion to overuse the drug.
Amphetamines cross the placenta and can affect the developing fetus. Compared to nonusers, women who use amphetamines during pregnancy are more likely to give birth prematurely and to have a low-birth-weight baby.
Nicotine
Nicotine, the psychoactive ingredient in tobacco products, is a stimulant that activates acetylcholine receptors. In the peripheral nervous system, activation of acetylcholine receptors increases heart rate and blood pressure. In the central nervous system, activation of acetylcholine receptors, which facilitates the release of dopamine and serotonin, creates pleasurable feelings of relaxation. It is nicotine that causes smokers to become "hooked" on cigarettes, ensuring continued exposure to the other injurious substances in the smoke.
Although smoking can be relaxing, nicotine is actually a stimulant of the brain and heart and blood vessels. Under the influence of nicotine, the heart beats as many as 33 more beats per minute. At the same time, the blood vessels constrict, so the heart is not only beating faster, but it is forcing blood through a less receptive circulatory system. The result is an increase in blood pressure. Nicotine also affects the platelets in the blood (these are described in Chapter 11 as cell fragments containing chemicals that initiate clotting). Nicotine causes the platelets to become sticky, increasing the likelihood of abnormal clots forming that may lead to heart attacks or strokes. A heart attack is the death of heart muscle cells, and a stroke is the death of nerve cells in the brain. Either can be caused by blockage of a blood vessel by a clot.
Nicotine is powerfully addictive. Ninety-five percent of smokers are physiologically dependent on it. Nicotine causes dopamine to be released in the brain's reward center, causing a pleasurable feeling. Drugs that stimulate the brain's reward center, such as nicotine, cocaine, and heroin, are highly addictive. Thus, smokers experience withdrawal symptoms when they try to quit. When a smoker tries to quit, nerve cells become hyperactive, causing withdrawal symptoms that include irritability, anxiety, headache, nausea, constipation or diarrhea, craving for tobacco, and insomnia. Most smokers continue smoking to avoid these unpleasant symptoms. Those who quit find that most of the withdrawal symptoms begin to lessen after a week without nicotine, but some may continue for weeks or even months. Certain symptoms, such as drowsiness, difficulty concentrating, and craving for a cigarette, seem to worsen about 2 weeks after quitting. Consequently, many smokers return to their habit and resume their exposure to nicotine and the other harmful substances in smoke.
Hallucinogens
The drugs that are classified as hallucinogenic are grouped together because of their similar effects, despite having very different structures. These effects include visual, auditory, or other distortions of sensation as well as vivid, unusual changes in thought and emotions.
The psychedelic drugs include some natural and some synthetic compounds. There are about six natural psychedelic drugs, the best known being mescaline, which comes from peyote cactus, and psilocybin, which is found in certain mushrooms. There are also synthetic drugs, including LSD (lysergic acid diethylamide) and MDMA,3 which is popularly known as ecstasy.
These drugs are thought to act by augmenting the action of the neurotransmitters serotonin, norepinephrine, or acetylcholine. For example, LSD, psilocybin, DMT (dimethyltrypta- mine), and bufotenin bind to the serotonin receptors in the brain, thereby mimicking the natural effects of serotonin. Ecstasy both binds to serotonin receptors and promotes the release of serotonin and dopamine. Mescaline, on the other hand, is structurally similar to norepinephrine and binds to norepinephrine receptors.
The normal physiological reactions to psychedelic drugs are not especially harmful, but the distortions of reality that the drugs produce may lead to behavior that is quite dangerous. "Bad trip" is the term most often used to describe an unpleasant reaction to a psychedelic drug. The symptoms may include paranoia, panic, depression, and confusion.
Tolerance for psychedelic drugs develops quickly. Furthermore, cross-tolerance among these drugs is the rule; that is, a person who has become tolerant of one psychedelic drug will be tolerant to others as well. Craving and withdrawal reactions are unknown, however, and laboratory animals offered LSD will not take it voluntarily.
Ecstasy deserves additional consideration because its use is growing rapidly. It is sometimes called the "love drug" or "hug drug" because of users who say it puts them at peace with themselves and at ease with others. Also a stimulant, ecstasy causes increases in heart rate, blood pressure, and body temperature—sometimes to dangerous levels. People using ecstasy feel energetic enough to dance all night, sometimes suffering dehydration and heat stroke, which occasionally lead to death. (Deaths are rare, however.) The release of serotonin from neurons causes a euphoric high, but the temporary depletion of serotonin in the days following ecstasy use can bring depression and anxiety. Ecstasy can also cause nausea, vomiting, and dizziness. Another danger is that ecstasy pills may contain drugs other than ecstasy. Among the drugs commonly found in these pills are the cough suppressant dextromethorphan, caffeine, ephedrine, and pseudoephedrine. Even the poison strychnine has been found.
Opiates
The opiates are natural or synthetic drugs that affect the body in ways similar to morphine, the major pain-relieving agent in opium. These and related drugs have two faces. On one hand, they have a high potential for abuse because tolerance and physical dependence occur. On the other hand, they are medically important because they alleviate severe pain.
Morphine and codeine, which come from the opium poppy, were among the first opiates used. Heroin is a synthetic derivative of morphine that is more than twice as powerful. Heroin is usually injected intravenously, but there are now forms that can be smoked or inhaled into the nasal cavity. Regardless of how it enters the body, heroin reaches the brain very quickly, producing a feeling that is usually described in ecstatic or sexual terms.
The opiates, including heroin, exert their effects by binding to the receptors for the body's endogenous (natural, internally produced) opiates: compounds called endorphins, enkephalins, and dynomorphins. These are neurotransmitters whose functions include roles in the perception of pain and fear.
Heroin and other commonly abused opiates have effects similar to those of morphine: euphoria, pain suppression, and reduction of anxiety. They also slow the breathing rate. An overdose may cause the user to fall into a coma or stop breathing. Overdose is always a potential problem with opiates bought on the street for illegal use. The buyer has no idea of the strength of the drug. Street supplies are often diluted with sugar. If a heroin addict who is accustomed to a diluted drug injects heroin that is much more potent than he or she is used to, death due to overdose often occurs. Extremely constricted pupils in an unconscious person are a sign of heroin overdose.
Many of the problems associated with heroin use arise because heroin addicts often suffer from a general disregard for good health practices. Other problems are associated with the injections themselves. Frequent intravenous injection of any drug is associated with certain ailments. Because of the constant puncturing, veins can become inflamed. In addition, shared needles may spread disease-causing organisms, including the viruses that cause AIDS and hepatitis and the bacterium that causes syphilis.
Looking ahead
In this chapter, we considered how psychoactive drugs affect communication among neurons. In the next chapter, we will examine how our sensory receptors detect external and internal stimuli.
__________________________________________________
1 In this chapter, the term oz (ounce) refers to a fluid ounce, which is equal to about 29 ml.
2 A slightly different type of THC receptor is found primarily on cells of the immune system.
3 3,4-methylenedioxymethamphetamine