Biology of Humans
9. Sensory Systems
In the previous chapter, we learned how the brain integrates sensory information to direct appropriate responses. In this chapter, we explore the human body’s general senses (such as touch, pressure, vibration, temperature, and pain) and our special senses (vision, hearing, balance, smell, and taste). We look closely at vision, hearing, and balance, examining how light, sound, and body position are reported by the intricate structures of the eye and ear. We also explore the relationship between smell and taste.
Sensory Receptors
Information about the external world and about the internal world of our bodies comes to us through our sensory receptors, structures that are specialized to detect and respond to changes in the environment, known as stimuli. If a stimulus is strong enough, these messages eventually become nerve impulses (action potentials) that are then conducted to the brain.
Sensation is an awareness of a stimulus. Whether a sensation is experienced as sight, sound, or something else depends on which part of the brain receives the nerve impulses. For example, photoreceptors respond best to light, but they can also respond to pressure. Regardless of the stimulus, nerve impulses from photoreceptors go to the visual cortex of the brain, and we see light. This is why, if you press gently on your closed eyelids, you will have the sensation of seeing spots of light. The pressure stimulates photoreceptors, which send nerve impulses to the visual cortex, and you sense light.
We use the word perception to describe the conscious awareness of sensations. Perception occurs when the cerebral cortex integrates sensory input (Figure 9.1). For example, light reflected from a banana strikes the eye, stimulating some of the photoreceptors. The brain interprets the pattern of input from the photoreceptors, and we perceive a banana.
· We rely on our senses—sight, hearing, taste, touch, and so on— for identifying the resources and conditions our bodies require and for recognizing danger. Our senses can also bring us pleasure.
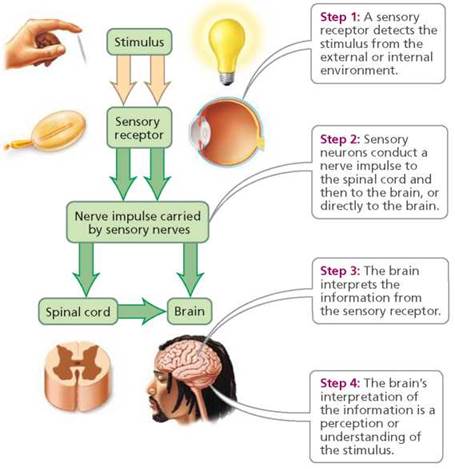
FIGURE 9.1. An overview of the steps involved in sensation and perception.
As we've seen, each type of sensory receptor responds best to one form of stimulus. The response of a sensory receptor is an electrochemical message (a change in the charge difference across the plasma membrane) that varies in magnitude with the strength of the stimulus. For instance, the louder a sound, the larger the change in the charge difference across the membrane—up to a point. When the change reaches a critical level, called threshold level, an action potential (nerve impulse) is generated. Most types of sensory receptors gradually stop responding when they are continuously stimulated. This phenomenon is called sensory adaptation. As receptors adapt in this way, we become less aware of the stimulus. For example, the musty smell of an antique store may be obvious to a person who just walked in, but the salesclerk working in the store no longer notices it. Some receptors, such as those for pressure and touch, adapt quickly. For this reason, we quickly become unaware of the feeling of our clothing against our skin. (Adaptation can also occur in the central nervous system. The reticular activating system in the brain filters stimuli, as discussed in Chapter 8.) Other receptors adapt more slowly or not at all. For instance, the receptors in muscles and joints that report on the position of body parts never adapt. Their continuous input is essential for coordinated movement and balance.
Classes of Receptors
Receptors are classified according to the stimulus they respond to. Several classes of receptors are traditionally recognized:
1. Mechanoreceptors are responsible for the sensations we describe as touch, pressure, hearing, and equilibrium. In addition, the body has mechanoreceptors that detect changes in blood pressure and others that indicate the body's position. Mechanoreceptors respond to distortions in the receptor itself or in nearby cells.
2. Thermoreceptors detect changes in temperature.
3. Photoreceptors detect changes in light intensity.
4. Chemoreceptors respond to chemicals. We describe the input from the chemoreceptors of the mouth as taste (gustation) and those from the nose as smell (olfaction). Other chemoreceptors monitor levels of specific substances such as carbon dioxide, oxygen, or glucose in our body fluids.
5. Pain receptors (or nociceptors) respond to very strong stimuli that usually result from physical or chemical damage to tissues. Pain receptors are sometimes classed with the chemoreceptors because they often respond to chemicals liberated by damaged tissue. These receptors are occasionally classed with the mechanoreceptors because they are stimulated by physical changes, such as swelling, in the damaged tissue.
We can sense stimuli both outside of our bodies and within them. Receptors located near the body surface respond to stimuli in the environment. We are usually aware of these stimuli. Other receptors are inside the body and monitor conditions there. Although we often are unaware of the activity of internal receptors, they play a vital role in maintaining homeostasis. In fact, they are key components of the feedback loops that regulate blood pressure, blood chemistry, and breathing rate. Internal receptors also cause us to feel pain, hunger, or thirst, thereby prompting us to attend to our body's needs.
The general senses—touch, pressure, vibration, temperature, body and limb position, and pain—arise from receptors in the skin, muscles, joints, bones, and internal organs. Although we are not usually aware of the general senses, they are important because they provide information about body position and help keep internal body conditions within the limits optimal for health. The special senses are vision, hearing, the sense of balance or equilibrium, smell, and taste. These are what usually come to mind when we think of "the senses," largely because we are so dependent on them for perceiving and understanding the world. The receptors of the special senses are located in the head. Most of them reside within specific structures.
The General Senses
The receptors for general senses are distributed throughout the body. Some monitor conditions within the body; others provide information about the world around us. Some of the receptors are free nerve endings; in other cases the nerve endings are encapsulated. Free nerve endings, the tips of dendrites of sensory neurons, are not protected by an accessory structure. In contrast, an encapsulated nerve ending is one in which a connective tissue capsule encloses and protects the tips of the dendrites of sensory neurons (Figure 9.2).
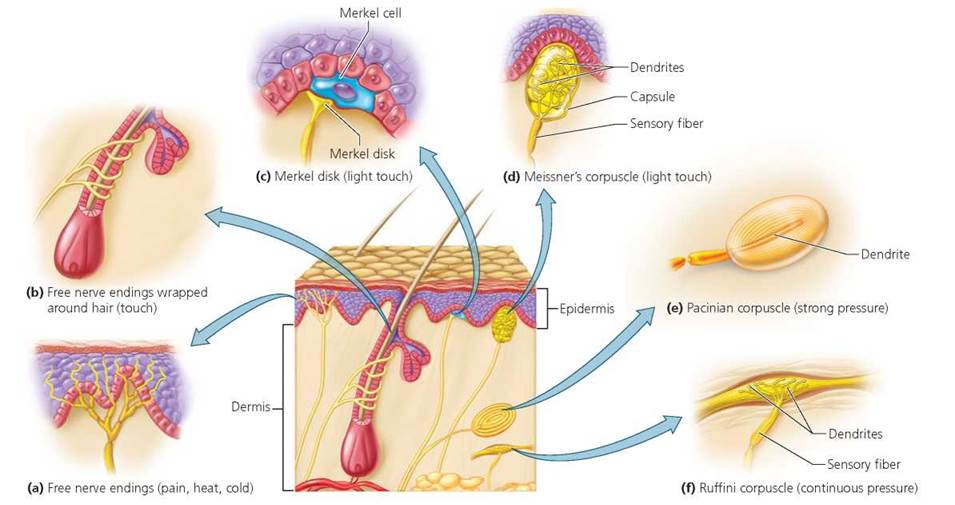
FIGURE 9.2. General sense receptors of the skin allow us to feel touch, pressure, temperature, and pain.
Touch, Pressure, and Vibration
As noted earlier, mechanoreceptors respond to touch and pressure—to any stimulus that stretches, compresses, or twists the receptor membrane. Throughout life, we actively use touch as a way of learning about the world and of communicating with one another. The messages we get from pressure can be equally important. Some pressure receptors inform us of the need to loosen our belt after a big meal. Other pressure receptors monitor internal conditions, including blood pressure.
Light touch, as when the cat's tail brushes your legs, is detected by several types of receptors. For example, free nerve endings wrapped around the base of the fine hairs on the skin detect any bending of those hairs. Free nerve endings and the special cells they end on (Merkel cells) form Merkel disks. When compressed, Merkel cells stimulate the free nerve endings in the associated Merkel disks to tell us that something has touched us. Merkel disks are found on both the hairy and hairless parts of the skin. Meissner's corpuscles are encapsulated nerve endings that tell us exactly where we have been touched. They are common on the hairless, very sensitive areas of skin, such as the lips, nipples, and fingertips.
The sensation of pressure generally lasts longer than does touch and is felt over a larger area. Pacinian corpuscles, which consist of onionlike layers of tissue surrounding a nerve ending, respond when pressure is first applied and therefore are important in sensing vibration. They are scattered in the deeper layers of skin and the underlying tissue. Ruffini corpuscles are encapsulated endings that respond to continuous pressure.
Temperature Change
Thermoreceptors respond to changes in temperature. In humans, thermoreceptors are specialized free nerve endings found just below the surface of the skin. One kind responds to cold and another responds to warmth. They are widely distributed throughout the body but are especially numerous around the lips and mouth. You may have noticed that the sensation of hot or cold fades rapidly. This fading occurs because thermoreceptors are very active when temperature is changing but adapt rapidly when temperature is stable. As a result, the water in a hot tub may feel scalding at first, but very soon it feels comfortably warm.
Body and Limb Position
Whether you are at rest or in motion, the brain "knows" the location of all your body parts. It continuously scans the signals from muscles and joints to check body alignment and coordinate balance and movement. Muscle spindles—specialized muscle fibers wrapped in sensory nerve endings—monitor the length of a skeletal muscle. Golgi tendon organs—highly branched nerve fibers located in tendons (connective tissue bands that connect muscles to bones)—measure the degree of muscle tension. The brain combines information from muscle spindles and Golgi tendon organs with information from the inner ear (as we see shortly) to coordinate our movements.
Pain
The receptors for pain are free nerve endings found in almost every tissue of the body. When tissue is damaged, cells release chemicals that alert the free nerve endings of the injury. The stimulated sensory neurons then carry the message to the brain, where it is interpreted as pain. Aspirin and ibuprofen reduce pain by interfering with the production of one of the released chemicals. Any stimulus strong enough to damage tissues, including heat, cold, touch, and pressure, can cause pain.
Many of our internal organs also have pain receptors. However, pain originating in an internal organ is sometimes perceived as pain in an uninjured region of the skin (Figure 9.3). This phenomenon is called referred pain. For example, the pain of a heart attack is often experienced as pain in the left arm. This pain probably occurs because sensory neurons from the internal organ and those from a particular region of the skin communicate with the same neurons in the spinal cord. Because the message is delivered to the brain by the same neurons, the brain interprets the input as coming from the skin.
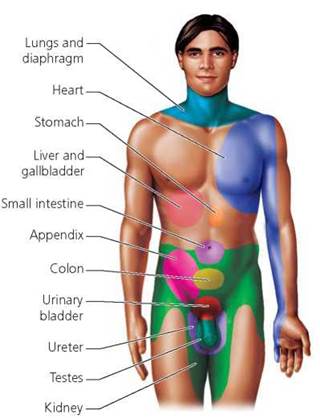
FIGURE 9.3. Referred pain. Pain from certain internal organs is sensed as originating in particular regions of the skin.
Pain is an important mechanism that warns the body and protects it from further injury. For example, pain usually prevents a person with a broken leg from causing additional damage by moving the limb. Nonetheless, few of us appreciate the value of pain while we are experiencing it. Furthermore, pain that persists long after the warning is needed can be debilitating.
Vision
Humans are very visual creatures. We may not see detail as well as an eagle or movement as well as an insect, but we see far better than most other mammals and depend on vision in most of the activities that make up our daily lives.
Wall of the Eyeball
The human eyeball is an irregular sphere about 25 mm (1 in) in diameter. As shown in Figure 9.4, the wall of the eyeball consists of three layers: the sclera and cornea; the choroid, ciliary body, and iris; and the retina. The outermost layer is a tough, fibrous covering with two distinct regions: the sclera and the cornea. The sclera, often called the white of the eye, protects and shapes the eyeball and serves as an attachment site for the muscles that move the eye. In the front and center of the eye, the transparent cornea bulges slightly outward and provides the window through which light enters the eye.
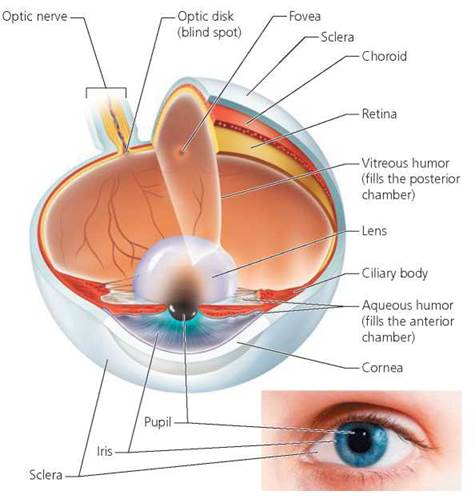
FIGURE 9.4 .Structure of the human eye. Light enters the eye through the transparent cornea and then passes through the pupil. The lens focuses light on the light-sensitive retina, which contains the rods and cones.
If you had pain caused by a kidney stone, where would you experience the pain?
The lower body trunk and inner thigh.
The middle layer of the eye has three distinct regions—the choroid, the ciliary body, and the iris. The choroid is a layer containing many blood vessels that supply nutrients and oxygen to the tissues of the eye. The choroid layer also contains the brown pigment melanin, which absorbs light reflected from the light-sensitive layer inside the eye (the retina). This absorption of light results in sharper vision by helping to prevent excessive reflection of light within the eye.
Toward the front of the eye, the choroid becomes the ciliary body—a ring of tissue, primarily muscle—that encircles the lens, which focuses light on the retina. The ciliary body holds the lens in place and controls its shape, which is important for focusing light on the light-sensitive layer of the eye.
The part of the choroid layer in front of the ciliary body is the iris. The iris, the colored portion of the eye that can be seen through the cornea, regulates the amount of light that enters the eye. The iris is shaped like a flat doughnut. The doughnut hole—the opening in the center of the iris through which light enters the eye—is called the pupil.
The iris contains smooth muscle fibers that automatically adjust the size of the pupil to admit the appropriate amount of light. The pupil becomes larger (dilates) in dim light and smaller (constricts) in bright light. Pupil size is also affected by emotions. The pupils dilate when you are frightened or when you are very interested in something. They constrict when you are bored. Candlelight creates a romantic setting partly because its dimness dilates the pupils, making the lovers appear more attentive and interested.
The innermost layer of the eye, the retina, contains almost a quarter-billion photoreceptors, the structures that respond to light by generating electrical signals. The retina contains two types of photoreceptors: rods and cones. The structure and function of rods and cones are discussed in more detail later in the chapter. The photoreceptors are most concentrated in a small region in the center of the retina called the fovea. Therefore, when we want to see fine details of an object, the light reflected from the object must be focused on the fovea. However, the fovea is only the size of the head of a pin. Consequently, at any given moment, only about a thousandth of our visual field is in sharp focus. Eye movements bring different parts of the visual field to the fovea. The optic nerve carries the message from the eye to the brain, where the message is interpreted. The region where the optic nerve leaves the retina has no photoreceptors. As a result, we cannot see an image that strikes this area. This area is called the blind spot. To find your blind spot, cover your left eye and focus on the X with your right eye. You should see the circle in your peripheral vision. Place this book in front of you and slowly move your head toward it. As your head moves, the image of the circle becomes focused on different regions of the retina. When the circle disappears, its image is focused on the blind spot.

You are not usually aware of your blind spot because involuntary eye movements constantly move the position of the image on the retina, allowing the brain to "fill in" the missing parts as the visual information is processed by the brain. Table 9.1 summarizes the structures of the eye and their functions.
Fluid-Filled Chambers
The ciliary body and lens divide the interior of the eyeball into two fluid-filled cavities, or chambers (see Figure 9.4). The posterior chamber, located at the back of the eye between the lens and the retina, is filled with a jellylike fluid called vitreous humor. This fluid helps keep the eyeball from collapsing and holds the thin retina against the wall of the eye. The anterior chamber, located at the front of the eye between the cornea and the lens, is filled with a fluid called aqueous humor. This clear fluid supplies nutrients and oxygen to the cornea and lens and carries away their metabolic wastes. In addition, the aqueous humor creates pressure within the eye, helping to maintain the shape of the eyeball. Unlike the vitreous humor, which is produced during embryonic development and is never replaced, aqueous humor is replaced bit by bit about every 90 minutes. It is continuously produced from the capillaries of the ciliary body, circulates through the anterior chamber, and drains into the blood through a network of channels that surround the eye.
TABLE 9.1. A Review of the Structures of the Eye and Their Functions
Structure |
Description |
Function |
Outer layer |
|
|
Sclera |
Outer layer of the eye |
Protects the eyeball |
Cornea |
Transparent dome of tissue forming the outer layer at the front of the eye |
Refracts light, focusing it on the retina |
Middle layer |
||
Choroid |
Pigmented layer containing blood vessels |
Absorbs stray light; delivers nutrients and oxygen to tissues of eye |
Ciliary body |
Encircles lens; contains the ciliary muscles |
Controls shape of lens; secretes aqueous humor |
Iris |
Colored part of the eye |
Regulates the amount of light entering the eye through the pupil |
Pupil |
Opening at the center of the iris |
Opening for incoming light |
Inner layer |
||
Retina |
Layer of tissue that contains the photoreceptors (rods and cones); also contains bipolar and ganglion cells involved in retinal processing |
Receives light and generates neural messages |
Rods |
Photoreceptor |
Responsible for black-and-white vision and vision in dim light |
Cones |
Photoreceptor |
Responsible for color vision and visual acuity |
Fovea |
Small pit in the retina that has a high concentration of cones |
Provides detailed color vision |
Other structures of the eye |
||
Lens |
Transparent, semispherical body of tissue behind the iris and pupil |
Fine focusing of light onto retina |
Aqueous humor |
Clear fluid found between the cornea and the lens |
Refracts light and helps maintain shape of the eyeball |
Vitreous humor |
Gelatinous substance found within the chamber behind the lens |
Refracts light and helps maintain shape of the eyeball |
Optic nerve |
Group of axons from the eye to the brain |
Transmits impulses from the retina to the brain |
If the drainage of aqueous humor is blocked, the pressure within the eye may increase to dangerous levels. This condition, called glaucoma, is the second most common cause of blindness (after cataracts, which are discussed shortly). The accumulating aqueous humor pushes the lens partially into the posterior cavity of the eye, increasing the pressure there and compressing the retina and optic nerve. This pressure, in turn, collapses the tiny blood vessels that nourish the photoreceptors and the fibers of the optic nerve. Deprived of nutrients and oxygen, the photoreceptors and nerve fibers begin to die, and vision fades. Unfortunately, glaucoma is progressive but painless, making detection difficult. Late signs include blurred vision, headaches, and seeing halos around objects. Many people do not realize they have a problem until some vision has been lost.
Focusing and Sharp Vision
Sharp, clear vision requires that the light rays entering the eye converge so that their focal point, the point where they are in focus, is on the retina. The structures of the eye accomplish this focusing by bending the light rays to the necessary degree.
Most bending of light occurs as the light passes through the curved surface of the cornea. Because of the way that the curved cornea bends the light rays, the image created on the retina is upside down and backward. The cornea has a fixed shape, so it always bends light to the same degree and cannot make the adjustments needed to focus on objects at varying distances.
The lens, on the other hand, is elastic and can change shape to focus on both near and distant objects. Picture the lens as an underinflated round balloon. If you pull on the sides of such a balloon, it flattens. When you release its sides, the balloon assumes its usual, rounder shape. Similar pulling and releasing changes the shape of the lens. Figure 9.5 shows that a rounder, thicker lens bends light to a greater degree, enabling the eye to focus on objects that are near. Changing the shape of the lens to change the bending of light is called accommodation.
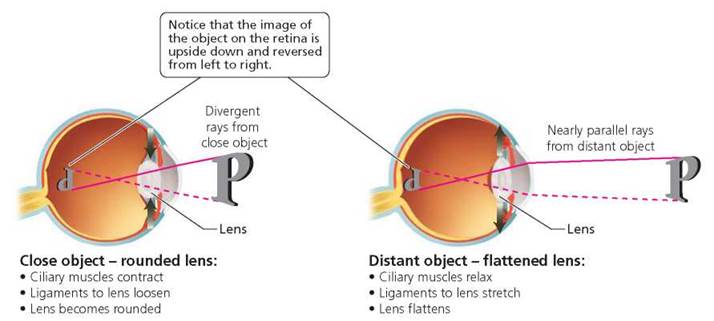
FIGURE 9.5. The lens changes shape so the eye can view objects at different distances.
These changes in lens shape are controlled by the ciliary muscle, which is attached to the lens by ligaments. Because the ciliary muscle is circular, its diameter becomes smaller when it contracts, much like pursed lips do. This contraction relaxes the tension on the ligaments, freeing the lens to assume the rounded shape needed to focus on nearby objects. Relaxation of the ciliary muscle increases the diameter of the ciliary muscle, increasing the tension on the ligaments and the lens. Consequently, the lens flattens and focuses light from more distant objects on the retina. As we age, the lens becomes less elastic and does not round up to focus on nearby objects as easily. This is why we hold the newspaper farther away as we become older.
Cataracts. A cataract is a cloudiness or opaqueness in the lens, usually a result of aging. Typically, the lens takes on a yellowish hue that blocks light on its way to the retina. In the beginning, cataracts may cause a person to see the world through a haze that can limit activities and cause automobile accidents, early retirement, and dangerous falls. As the lens becomes increasingly opaque, the fog thickens. Indeed, cataracts are the leading cause of blindness worldwide. Cataracts can be treated by surgically removing the clouded lens and replacing it with an artificial lens.
Cataracts are the most common eye problem affecting men and women older than 50. However, there are some things that everyone can do to minimize the risk of developing cataracts. Wear sunglasses in bright sunlight because exposure to ultraviolet radiation and bright light can cause cataracts. Cigarette smoke also causes cataracts, so minimize your exposure.
Focusing problems. The three most common visual problems that occur in individuals of all ages are all problems in focusing. These include farsightedness, nearsightedness, and astigmatism. With each of these focusing problems, normal vision can usually be restored with corrective lenses. Roughly 60% of Americans are farsighted (Table 9.2). In farsightedness, distant objects are seen more clearly than nearby ones because the eyeball is too short or the lens is too thin, causing images of nearer objects to be focused behind the retina. Although distant objects can be seen clearly, the lens cannot become round enough to bend the light sufficiently to focus on nearby objects. Corrective lenses that are thicker in the middle than at the edges (convex) cause the light rays to converge a bit before they enter the eye. The lens can then focus the image on the retina.
TABLE 9.2. Focusing Problems of the Eye
Problem |
Description |
Cause |
Correction |
Farsightedness |
See distant objects more clearly than nearby objects |
Eyeball too short or lens too thin; lens cannot become round enough |
Convex lens; increases corneal curvature |
Nearsightedness |
See nearby objects more clearly than distant objects |
Eyeball too long or lens too thick; lens cannot flatten enough |
Concave lens; decreases corneal curvature |
Astigmatism |
Visual image is distorted |
Irregularities in curvature of cornea or lens |
Lenses that correct for the asymmetrical bending of light |
About 30% of the American population is nearsighted; that is, they can see nearby objects more clearly than those far away. Nearsightedness (myopia) occurs when the eyeball is elongated or when the lens is too thick. This condition causes the image to focus in front of the retina. Nearsighted people see nearby objects clearly because the lens becomes round enough to focus the image on the retina. However, the lens simply cannot flatten enough to bring the focused image of distant objects to the retina, and so those objects appear blurred. Lenses that are thinner in the middle than at the edges (concave) can correct nearsightedness. These lenses cause the light rays to diverge slightly before entering the eye.
Although genetics undoubtedly plays a role in the development of nearsightedness, frequent close work, such as reading or working at a computer, is also a cause. When you do a lot of close work, the frequent contractions of the ciliary muscles that change the shape of the lens increase the pressure within the eye. This pressure can cause the eye to stretch and elongate, resulting in nearsightedness. Eye specialists recommend that you look up from the page or away from the computer screen at frequent intervals—particularly if nearsightedness runs in your family.
Irregularities in the curvature of the cornea or lens will cause distortion of the image because they cause the light rays to converge unevenly. This condition is called astigmatism. Vision can almost always be restored to normal by corrective lenses that compensate for the asymmetrical bending of light rays (Figure 9.6).
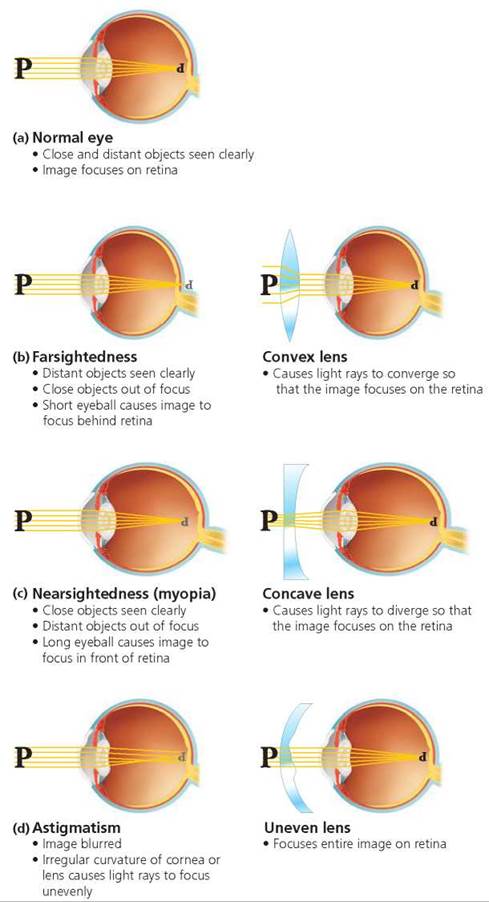
FIGURE 9.6. Focusing problems such as farsightedness, nearsightedness, and astigmatism are caused when the image of an object is not focused on the retina. These vision problems can be corrected with the use of specific lenses.
Many people who are tired of depending on glasses or contact lenses have opted to undergo laser eye surgery. This procedure is popularly known as LASIK, which stands for laser-assisted in situ keratomileusis. LASIK permanently changes the shape of the cornea. The procedure involves cutting a flap in the cornea, using pulses from a computer- controlled laser to reshape the middle layer of the cornea, and then replacing the flap. This treatment is used to correct for nearsightedness, farsightedness, and astigmatism.
Another procedure for reshaping the cornea is LASEK (laser-assisted subepithelial keratomileusis). It differs from LASIK in that the surgeon creates a flap in the epithelium only, instead of in the entire cornea, eliminating some of the complications caused by the deeper corneal flaps. LASEK is used mostly for people who are poor candidates for LASIK because their corneas are thin or flat. In yet another procedure, photorefractive keratectomy (PRK), a surgeon uses short bursts of a laser beam to shave a microscopic layer of cells off the corneal surface and flatten it. A computer calculates and controls the laser exposure.
Light and Pigment Molecules
The eye contains a whopping 70% of all the sensory receptors in the body. The function of the eye's receptors, both rods and cones, is to respond to light by sending neural messages to the brain, where they are translated into images of our surroundings.
So how does vision work? First, light waves in the visible spectrum (the spectrum of wavelengths our eyes can detect) strike an object. At least some wavelengths are reflected off the object to the eye, where they are focused by the cornea and lens onto the retina and absorbed by photopigment molecules in the photoreceptors. When light strikes a photopigment, it causes the photopigment molecule's components to split apart. This change causes a series of reactions that reduce the photoreceptor's release of inhibitory neurotransmitter. The neurotransmitter normally inhibits the cells involved in processing the information (discussed shortly); and so, by leading to reduced neurotransmitter levels, light increases the activity of these processing cells. The optic nerve carries these nerve signals from the retina to the thalamus of the brain, where some processing of the information occurs. The information is then sent to the visual cortex, located at the back of the brain, where a perception of the world outside takes shape.
The processing of electrical signals from the rods and cones begins before the signals leave the retina. The messages are first sent to bipolar cells in the retina. These cells are rare examples of neurons that have only two processes, an axon and a single dendrite, extending from opposite sides of the cell body. Bipolar neurons direct the information to interneurons called ganglion cells (Figure 9.7). Together, bipolar cells and ganglion cells convert the input from the retina into patterns, such as edges and spots.
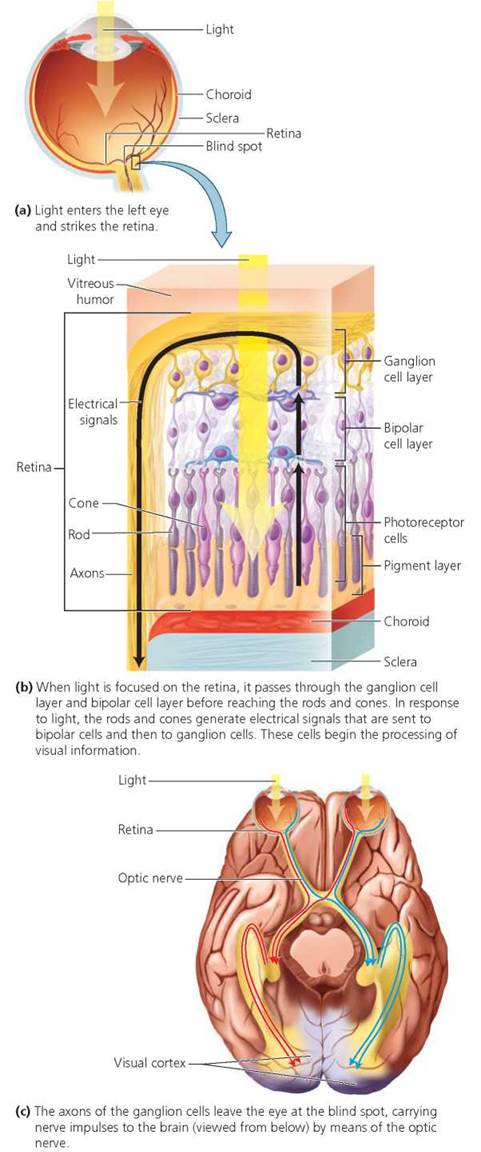
FIGURE 9.7. Neural pathways of the retina convert light to nerve signals.
Rods: Vision in Dim Light
The rods are more numerous than the cones and are the photoreceptors responsible for black-and-white vision (Figure 9.8).
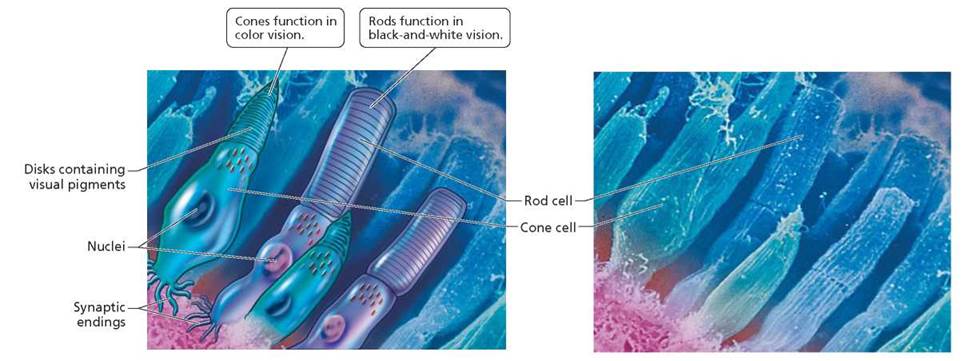
FIGURE 9.8. Rods and cones, the photoreceptors in the retina, are named for their shapes. Their function is to generate neural messages in response to light. The outer portion of each photoreceptor is packed with membrane-bound disks that contain pigment molecules.
Rods are exceedingly sensitive to light and are capable of responding to light measuring one 10-billionth of a watt—the equivalent of a match burning 50 mi (80.5 km) away on a clear, pitch-dark night! (Of course, the ideal environmental conditions necessary to actually see a burning match at such a distance are impossible to attain.) The rods allow us to see in dimly lit rooms and in pale moonlight. By detecting changes in light intensity across the visual field, rods contribute to the perception of movements.
The pigment in rods, called rhodopsin, is packaged in membrane-bound disks that are stacked like coins in the outer segment of the rod. Light strikes a rod, splits the rhodopsin, and triggers events that reduce the permeability of the plasma membrane to sodium ions. This reaction eventually leads to changes in the activity of bipolar cells and ganglion cells. In the dark, rhodopsin is resynthesized. The reason you have difficulty seeing when you first walk into a dark room from a brightly lit area is that the rhodopsin in your photoreceptors has been split. As rhodopsin is resynthesized, your vision becomes sharper.
Cones: Color Vision
The cones are the photoreceptors responsible for color vision. Unlike the rods, the cones produce sharp images, because each cone usually sends information to only one bipolar cell for processing.
What makes you see red? Red, or any other color, is determined by wavelengths of light. White light, such as that emitted by an ordinary lightbulb or the sun, consists of all wavelengths. (Rainbows are created when the various wavelengths of white light are separated as they pass through tiny droplets of water in the air.) When light strikes an object, some of the wavelengths may be absorbed and others reflected; we see the wavelengths that are reflected. Thus, an apple looks red because it reflects mostly red light and absorbs most of the other wavelengths.
We see color because we have three types of cones, called blue, green, and red. The cones are named for the wavelengths they absorb best, not for their color. When light is absorbed, the cone is stimulated. Actually, each type of cone absorbs a range of wavelengths, and the ranges overlap quite a bit. As a result, colored light stimulates each type of cone to a different extent. For instance, when we look at a bowl of fruit, light reflected by a red apple stimulates red cones, light reflected by a ripe yellow banana stimulates both red and green cones, and light reflected from blueberries stimulates both blue and green cones. The brain then interprets color according to how strongly each type of cone is stimulated.
Stop and think
Most bipolar cells receive input from several rods but from only one cone in the fovea. How might this difference explain why rods permit us to see at lower light intensities than do cones? How might it explain why the sharpest images are formed when the object is focused on the fovea?
Color blindness is a condition in which certain colors cannot be distinguished from each other. Most people who are color blind see some colors, but they tend to confuse certain colors with others. Thus, a standard test for color blindness is to show the individual a color plate with dots of two colors (Figure 9.9). Dots of one color indicate a number. A person who is color blind cannot distinguish the number. A lack, or a reduced number, of one of the types of cones causes the confusion. A person who lacks red cones sees deep reds as black. In contrast, a person who lacks green cones sees deep reds but cannot distinguish between reds, oranges, and yellows. Absence of blue cones is extremely rare.
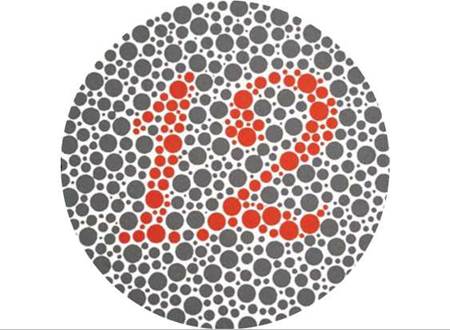
FIGURE 9.9. A standard test for color blindness. A person who lacks one of the three types of cones would not be able to distinguish the number 12 in the center of this circle.
People who are color blind generally function normally in everyday life. They compensate for the inability to distinguish certain colors by using other cues, such as intensity, shape, or position. Ironically, red and green—the universal traffic colors for stop and go—are the most commonly confused colors. However, it is usually possible to pick out the brightest of the lights in a traffic signal, and all traffic signals are arranged the same way—red on top and green on the bottom. Schoolchildren are regularly tested for color blindness so that both students and teachers are aware of the condition. Color blindness may cause difficulty with class work, such as reading maps or graphs that are presented in color. If a teacher is aware of the condition, steps can be taken to avoid frustration and confusion for the student.
Hearing
From a social perspective, hearing is perhaps the most important of our senses because speech plays such an important role in the communication that binds society. Hearing can also make us aware of things in the external world that we cannot see—telling us of a car approaching from behind as we jog, for instance. Hearing can also add to our understanding of events that we can see, as when a mother determines by the sound of the cry whether her baby is hungry or in pain. And hearing can enrich the quality of our lives, as when we listen to music or hear waves crashing on the shore.
In every instance, what we hear are sound waves produced by vibration. Vibrating objects, such as guitar strings, the surface of the stereo speaker, or vocal cords, move rapidly back and forth. The vibrations push repeatedly against the surrounding air, creating sound waves, as shown in Figure 9.10. The loudness of sound is determined by the amplitude of the sound wave, represented graphically as the distance between the top of peaks and the bottom of troughs. The pitch is determined by the frequency, the number of cycles (repetitions of the wave) per second. The more cycles there are, the higher the pitch.

FIGURE 9.10. A sound wave and the effects of amplitude (height) and frequency (cycles per second)
Form and Function of the Ear
The ear has three main parts—the outer ear, the middle ear, and the inner ear—as shown in Figure 9.11. The outer ear functions as a receiver. The part of the outer ear visible on the head consists of a fleshy funnel called the pinna. The pinna gathers the sound and channels it into the external auditory canal, which leads from the pinna to the eardrum. The pinna also accentuates the frequencies of the most important speech sounds, making speech easier to pick out from background noise. The pinna's shape and placement at either side of the head help us determine the direction a sound comes from.
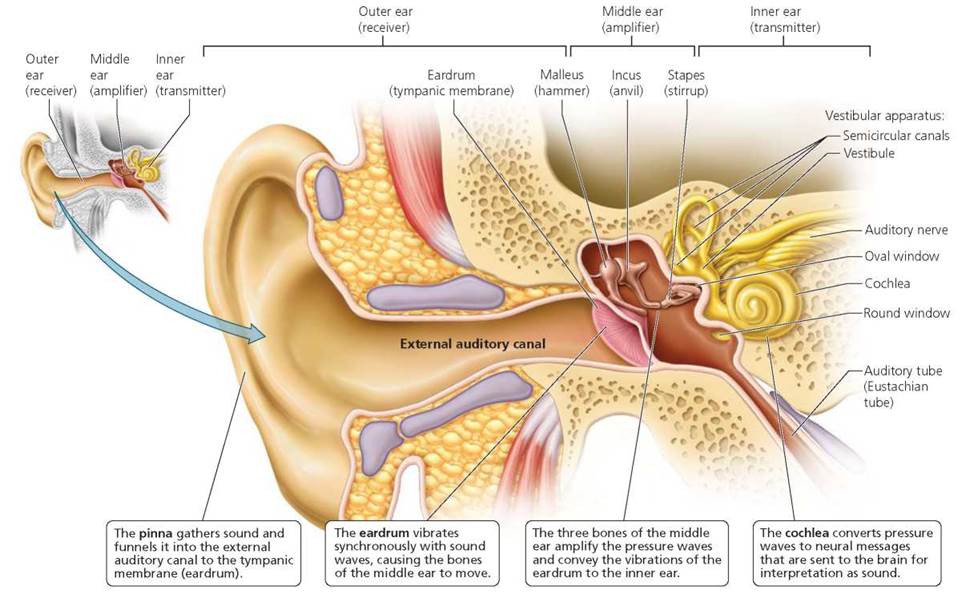
FIGURE 9.11. Structure of the ear. The human ear has three parts: the outer ear (the receiver), the middle ear (the amplifier), and the inner ear (the transmitter).
The tissue that separates the outer ear from the middle ear is the eardrum, or tympanic membrane. It is as thin as a sheet of paper and as taut as the head of a tambourine. When sound waves strike the eardrum, it vibrates at the same frequency as the sound waves and transfers these vibrations to the middle ear.
Stop and think
As we age, the tissues of the eardrum thicken and become less flexible. How do these changes partially explain why sensitivity to high-frequency sounds is usually lost as we grow older?
The middle ear serves as an amplifier. It consists of an air- filled cavity within a bone of the skull and is spanned by the three smallest bones of the body: the malleus (hammer), incus (anvil), and stapes (stirrup)—named to indicate their respective shapes. Together, these bones function as a system of levers to convey the airborne sound waves from the eardrum to the oval window, a sheet of tissue that forms the threshold of the inner ear. The malleus is attached to the inner surface of the eardrum. Therefore, the vibrations of the eardrum in response to sound cause the malleus to rock back and forth. The rocking of the malleus, in turn, causes the incus and then the stapes to move. The base of the stapes fits into the oval window.
The force of the eardrum's vibrations is amplified 22 times in the middle ear. The magnification of force is necessary to transfer the vibrations to the fluid of the inner ear. The amplification occurs because the eardrum is larger than the oval window. This size difference concentrates the pressure against the oval window.
The air pressure must be nearly equal on both sides of the eardrum for the eardrum to vibrate properly. If the pressure is not equal, the eardrum will bulge inward or outward and will be held in that position, causing pain and difficulty hearing. For instance, when a person ascends quickly to a high altitude, the atmospheric pressure is lower than the pressure in the middle ear, and the eardrum bulges outward. Unequal pressure usually is alleviated by the auditory tube (also known as the Eustachian tube), a canal that connects the middle ear cavity with the upper region of the throat. Most of the time, the auditory tube is closed and flattened. However, swallowing or yawning opens it briefly, allowing the pressure in the middle ear cavity to equalize with the air pressure outside the ear. The sensation of pressure suddenly equalizing is described as the ear "popping." It can occur whenever the pressure on the external eardrum changes quickly, as when you ride up or down in an elevator, take off or land in an airplane, or go scuba diving.
The inner ear is a transmitter. It generates neural messages in response to pressure waves caused by sound waves, and it sends the messages to the brain for interpretation. The inner ear contains two sensory organs, only one of which, the cochlea (kok'-le-ah), is concerned with hearing. The other sensory organ, the vestibular apparatus, is concerned with sensations of body position and movement and will be discussed in the next section.
The cochlea is about the size of a pea, and it can be considered the true seat of hearing. It is a bony tube about 35 mm (1.4 in) long that is coiled about two-and-a-half times and looks somewhat like the shell of a snail, as you can see in Figure 9.12. (Cochlea is from the Latin for "snail.") The wider end of the tube, where the snail's head would be, has two membrane-covered openings. The upper opening is the oval window, into which the stapes fits. The lower opening, called the round window, serves to relieve the pressure created by the movements of the oval window.
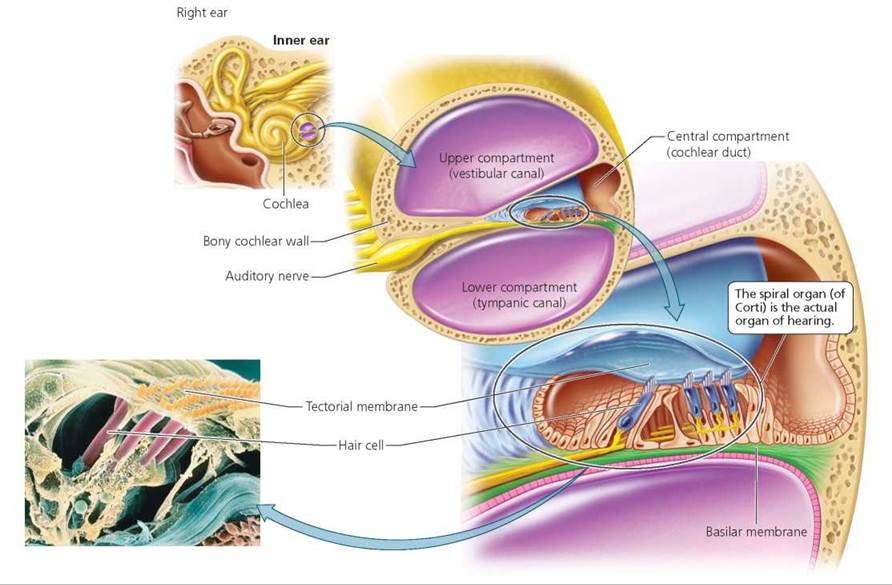
FIGURE 9.12. The cochlea houses the spiral organ (of Corti). The spiral organ consists of the hair cells and the overhanging gelatinous tectorial membrane. The spiral organ rests on the basilar membrane. The hairs are the receptors for hearing. In the micrograph, the hair cells are colored pink and their “hairs" are colored yellow.
The internal structure of the cochlea is easier to understand if we imagine the cochlea uncoiled so that it forms a long straight tube. We would then see that two membranes divide the interior of the cochlea into three longitudinal compartments, each filled with fluid. The central compartment (the cochlear duct) ends blindly, like the finger on a glove, and does not extend completely to the end of the cochlea's internal tube. As a result, the upper and lower compartments (the vestibular canal and the tympanic canal) are connected at the end of the tube nearest to the tip of the coil. The basilar membrane is the floor of the central compartment. The spiral organ (of Corti), the portion of the cochlea most directly responsible for the sense of hearing, is supported on the basilar membrane (Figure 9.13). The spiral organ consists of the hair cells and the overhanging tectorial membrane. Each hair cell has about 100 "hairs," slender projections from its upper surface that project into the tectorial membrane. The hair cells are arranged on the basilar membrane in rows that resemble miniature picket fences.
When the stapes moves to and fro against the oval window, it sets up corresponding movements—pressure waves—in the fluid of the inner ear (Figure 9.13). Those pressure waves are then transmitted from the fluid of the cochlea's upper compartment to the fluid of the lower compartment, because the compartments are continuous. The movements of the fluid cause the basilar membrane to swing up and down; this swinging, in turn, causes the projections on the hair cells to be pressed against the tectorial membrane. The bending of the hairs ultimately alters the rate of nerve impulses in the auditory (cochlear) nerve, which arises within the cochlea and carries sound information to the brain. The structures of the ear and their functions are summarized in Table 9.3.
TABLE 9.3. Review of the Structures of the Ear and Their Functions
Structure |
Description |
Function |
Outer ear |
||
Pinna |
Fleshy, funnel-shaped part of the ear protruding from the side of the head |
Collects and directs sound waves |
External auditory canal |
Canal between pinna and tympanic membrane |
Directs sound to the middle ear |
Middle ear |
||
Eardrum (tympanic membrane) |
Membrane spanning the end of the external auditory canal |
Vibrates in response to sound waves |
Malleus (hammer), incus (anvil), and stapes (stirrup) |
Three tiny bones of the middle ear |
Amplify the vibrations of the tympanic membrane and transmit vibrations to inner ear |
Auditory tube (Eustachian tube) |
A tube that connects the middle ear with the throat |
Allows equalization of pressure in middle ear with external air pressure |
Inner ear |
||
Cochlea |
Fluid-filled, bony, snail-shaped chamber |
Houses spiral organ (of Corti) and has openings called oval window and round window |
Spiral organ (of Corti) |
Contains hair cells |
The organ of hearing |
Oval window |
Membrane between the middle and inner ear that the stapes presses against |
Transmits the movements of the stapes to the fluid in the inner ear |
Round window |
Membrane at the end of the lower canal in cochlea |
Relieves pressure created by the movements of the oval window |
Vestibular apparatus |
Fluid-filled chambers and canals |
Monitors position and movement of the head |
Vestibule (utricle and saccule) |
Two fluid-filled chambers |
Maintains static equilibrium (body and head stationary, information on position of head) |
Semicircular canals |
Three fluid-filled chambers oriented at right angles to one another |
Maintain dynamic equilibrium (body or head moving) |
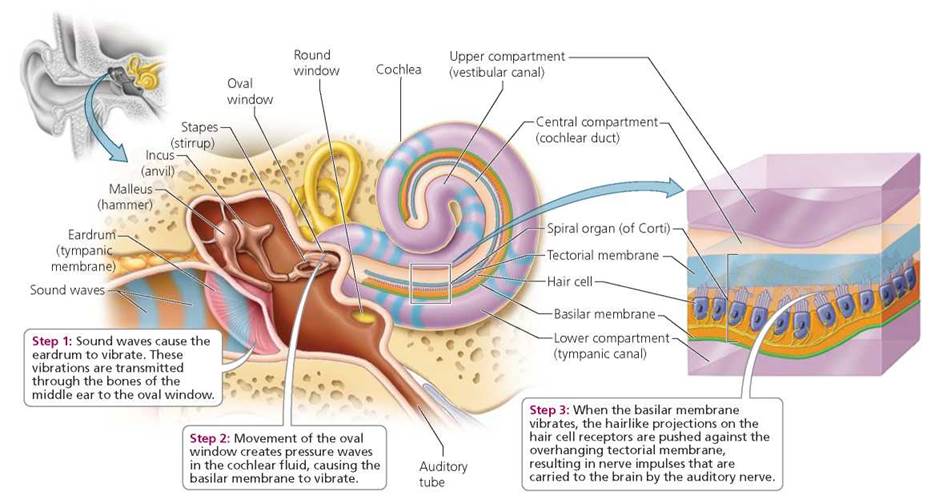
FIGURE 9.13. The sequence of events from sound vibration to a nerve impulse begins when sound enters the external auditory canal.
Loudness and Pitch of Sound
The louder the sound, the greater the pressure changes in the fluid of the inner ear and, therefore, the stronger the bending of the basilar membrane. Because hair cells have different thresholds of stimulation, more vigorous vibrations in the basilar membrane stimulate more hair cells. In addition, each hair cell bends more with more vigorous vibrations of the basilar membrane, which increases the number of nerve impulses. The brain interprets the increased number of impulses as louder sound.
How does the ear determine the pitch of a sound? Different regions of the basilar membrane vibrate in response to sounds of different pitch. In a sense, the cochlea is like a spiral piano keyboard. The basilar membrane varies in width and flexibility along its length. Near the oval window, the basilar membrane is narrow and stiff. Like the shorter strings on a piano, this region vibrates maximally in response to high- frequency sound, such as a whistle. At the tip of the tube in the cochlea, the basilar membrane is wider and floppier. Low- frequency sounds, such as a bass drum, cause maximum vibrations in this region of the basilar membrane. Thus, sounds of different pitches activate hair cells at different places along the basilar membrane. The brain then interprets input from hair cells in different regions as sounds of different pitch.
Hearing Loss
An estimated 28 million Americans have some degree of hearing loss, and 2 million of them are completely deaf. Hearing loss that is severe enough to interfere with social and job- related communication is among the most common chronic neural impairments in the United States.
There are two types of hearing loss: conductive loss and sensorineural loss. Conductive loss results when an obstruction anywhere along the route prevents sounds from being conducted through the external auditory canal to the eardrum and over the bones of the middle ear to the inner ear. The external auditory canal can become clogged with wax or other foreign matter. In this case, inserting cotton-tipped swabs usually aggravates the situation by further clogging the canal and should therefore be avoided. Other possible causes for conductive hearing loss are thickening of the eardrum, which might occur with chronic infection, or perforation of the eardrum, which might occur as a result of trauma. Excess fluid in the middle ear, which often occurs with middle ear infections, can prevent movement of the eardrum and cause temporary conductive hearing loss.
Sensorineural deafness is caused by damage to the hair cells or to the nerve supply of the inner ear. A common cause is gradual loss of hair cells throughout life. Some of the loss is simply due to aging. After age 20, the loss of hair cells causes us to lose about 1 Hz of our total perceptive range of 20,000 Hz every day. However, much of the damage to hair cells is caused by exposure to loud noise (see the Environmental Issue essay, Noise Pollution). Neural damage can also be caused by infections, including mumps, rubella (German measles), syphilis, and meningitis. In addition, drugs such as those used for treating tuberculosis and certain cancers can cause neural damage.
Hearing can be damaged by exposure to noise that is loud enough to make conversation difficult. The louder a sound, the shorter the exposure time necessary to damage the ear. Even a brief, explosively loud sound is capable of damaging hair cells. More commonly, however, hearing loss results from prolonged exposure to volumes over 85 dB. At 110 dB, the average rock concert or stereo headset at full blast can damage your ears in as little as 30 minutes. If sounds seem muffled to you or if your ears are ringing after you leave a noisy area, you probably sustained some damage to your ears.
A surprising number of young people also have impaired hearing. The culprit is most likely noise—probably in the form of music. How can you protect yourself? Don't listen to loud music. Keep it tuned low enough that you can still hear other sounds. If you are listening with earphones, no one else should be able to hear the sound from them. When you cannot avoid loud noise, as when you are mowing the lawn, vacuuming, or attending a rock concert, wear earplugs to protect your hearing. You can buy them at most drugstores, sporting goods stores, and music stores.
One of the first signs of sensorineural damage is the inability to hear high-frequency sounds. Because consonants, which are needed to decipher most words, have higher frequencies than do vowels, speech becomes difficult to understand. So beware if you find yourself asking, "Could you repeat that?"
The most effective way to deal with hearing loss is with a hearing aid. The basic job of a hearing aid is to amplify sound. One type of hearing aid presents amplified sound to the eardrum. Another type uses a vibrator or stimulator placed in the bone of the skull behind the ear. Sound is then conducted through the bones of the skull to the inner ear.
Hearing aids often are unable to help profoundly deaf people, but cochlear implants can pierce the silence for some of them. A cochlear implant does not amplify sounds like a hearing aid does; instead, it compensates for parts of the inner ear that are not functioning properly. A cochlear implant consists of an array of electrodes that transforms sound into electrical signals that are delivered to the nerve cells near the cochlea. The implant is surgically inserted into the cochlea through the round window. A cochlear implant allows some people who were severely hearing impaired or totally deaf to converse with someone in person or on the phone. By providing exposure to sounds during the time when language is developing, cochlear implants also help deaf children learn to speak well.
What would you do?
Many deaf people consider themselves to be a cultural group, not a group with a medical problem. Some people argue, for instance, that communication is the real challenge faced by the deaf and that the solution should therefore be a social, not a medical, one. If medical technology is available, should we use it to “fix” conditions such as deafness? If you had a child who was born deaf, would you want a cochlear implant for that child? Why or why not? (Assume that the child is not yet able to make that decision for him- or herself.)
Ear Infections
An external ear infection is an infection in the ear canal. Swimmer's ear, the most common such infection, is precipitated by water trapped in the canal, which creates an environment favorable for bacterial growth. The first symptom of swimmer's ear is itching, usually followed by pain that can become intense and constant. Chewing food or touching the earlobe sharpens the pain. The usual treatment consists of antibiotic ear drops, heat, and pain medication. To prevent swimmer's ear, always be sure to drain any remaining water from the ear canal after swimming or bathing—if necessary, by shaking the head.
Middle ear infections usually result from infections of the nose and throat that work their way through the auditory tubes connecting the throat and middle ear. At least half of all children get an ear infection at some time; some children get four or five ear infections a year. Middle ear infections are more common in children than in adults because the auditory tubes curve and tilt downward in adults. In children, the tubes are nearly horizontal, allowing infectious organisms to travel through them more easily. The signs of a middle ear infection are a stabbing earache, impaired hearing, and a feeling of fullness in the ear, often accompanied by fever. A middle ear infection usually is treated with an antibiotic.
Environmental Issue
Noise Pollution
It is difficult to escape the din of modern life—noise from airports, city streets, loud appliances, iPODS. Noise pollution threatens your hearing and your health. Exposure to excessive noise is to blame for the hearing loss of one-third of all hearing-impaired people. Loud noise damages the hairs on the hair cells of the inner ear. When the hairs are exposed to too much noise, they wear down, lose their flexibility, and can fuse together (Figure 9.A). Unfortunately, there is no way to undo the damage; you cannot grow spare parts for your ears.
The loudness of noise is measured in decibels (dB). The decibel scale is logarithmic. An increase of 10 dB generally makes a given sound twice as loud. The decibel ratings and effects of some familiar sounds are given in Table 9.a. Most people judge sounds over 60 dB to be intrusive, over 80 dB to be annoying, and over 100 dB to be extremely bothersome. The federal Occupational Safety and Health Administration (OSHA) has set 85 dB as the safety limit for 8 hours of exposure. The threshold for physical pain is 140 dB.
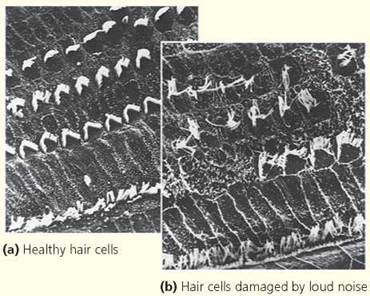
FIGURE 9.A. The hair cells of the inner ear can be permanently damaged by loud noise.
TABLE 9.a. Loudness of Familiar Sounds
Sound Source |
Loudness (dB) |
Effect from Prolonged Exposure |
Jet plane at takeoff |
150 |
Eardrum rupture |
Rock-and-roll band (at maximum volume) |
130 |
Irreversible damage |
Jet plane at 152 m (500 ft) |
110 |
Loss of hearing |
Electric blender |
90 |
Annoying |
Traffic noise |
70 |
Intrusive |
Quiet neighborhood (daytime) |
50 |
|
Soft background music |
40 |
Quiet |
Whisper |
20 |
Very quiet |
|
0 |
Threshold of hearing |
Questions to Consider
• Do you think that local governments should have more regulations to control noise pollution?
• Do you think there should be regulations about how loud the music at a concert can be played?
Balance and the Vestibular Apparatus of the Inner Ear
The vestibular apparatus, a fluid-filled maze of chambers and canals within the inner ear, is responsible for monitoring the position and movement of the head. The receptors in the vestibular apparatus are hair cells similar to those in the cochlea.
Head movements or changes in velocity cause the hairs on these cells to bend, sending messages to the brain. The brain uses this input to maintain balance.
The vestibular apparatus consists of the semicircular canals and the vestibule. The semicircular canals are three canals in each ear that contain sensory receptors and help us stay balanced as we move. They monitor any sudden movements of the head, including those caused by acceleration and deceleration, to help us maintain our equilibrium when the body or head is moving (see "dynamic equilibrium" in Figure 9.14). At the base of each semicircular canal is an enlarged region called the ampulla. Within the ampulla is a tuft of hair cells. The hairlike projections from these cells are embedded in a pointed "cap" of stiff, pliable, gelatinous material called the cupula. When you move your head, fluid in the canal lags a little behind, causing the cupula to bend the hair cells and stimulate them.
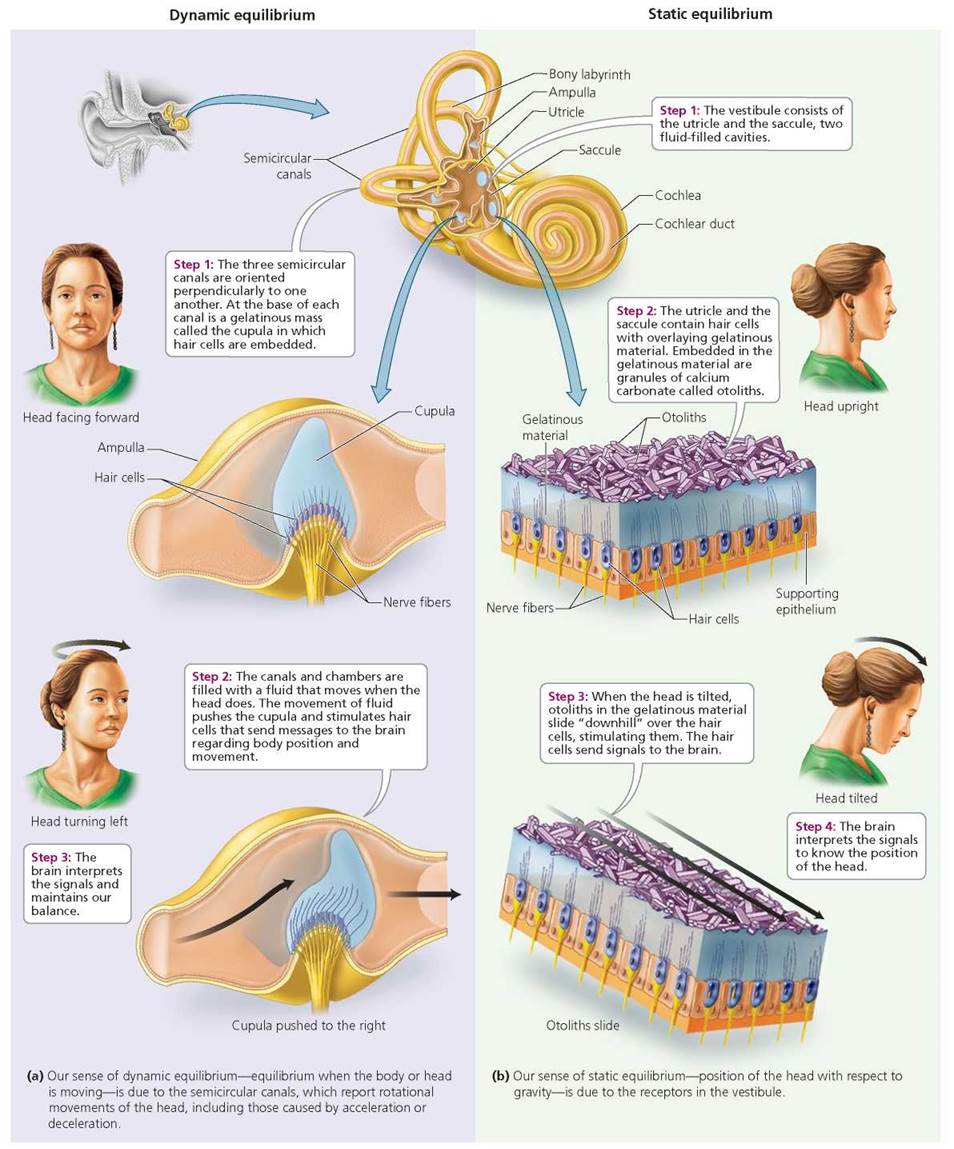
FIGURE 9.14. Dynamic and static equilibrium
The three semicircular canals in each ear are oriented at right angles to one another. Head movements cause the fluid in the canals to move in the direction opposite the direction of movement, in the same way that sudden acceleration slams passengers back against the car seat. Whereas nodding your head to say yes will cause the fluid in the canals parallel to the sides of the head to swirl, shaking it from side to side to say no will cause fluid in the canals parallel to the horizon to move. Tilting your head to look under the bed will cause fluid in the canals that are parallel to your face to move back and forth. Even the most complex movement can be analyzed in terms of motion in three planes.
Stop and think
When you stop moving, there is a time lag before the fluid in the semicircular canals stops swirling. How does this time lag account for the sensation of dizziness after you have been twirling around for a while?
The vestibule, the other part of the vestibular apparatus, is important for static equilibrium—the maintenance of balance when we are not moving. The vestibule consists of the utricle and the saccule, two fluid-filled cavities that literally let us know which end is up (Figure 9.14). These cavities tell the brain the position of the head with respect to gravity when the body is not moving. They also respond to acceleration and deceleration, but not to rotational changes as the semicircular canals do. Both the utricle and the saccule contain hair cells overlaid with a gelatinous material in which small chalklike granules of calcium carbonate are embedded. These granules, called otoliths, make the gelatin heavier than the surrounding material and thus make it slide over the hair cells whenever the head is moved. The movement of the gelatin stimulates the hair cells, which send messages to the brain, and the brain interprets the messages to determine the position of the head relative to gravity.
The utricle and saccule sense different types of movement. The utricle senses the forward tilting of the head, as well as forward motion, because its hair cells are on the floor of the chamber and oriented vertically when the head is upright. In contrast, the hair cells of the saccule are on the wall of the chamber, oriented horizontally when the head is upright. They respond when you move vertically, as when you jump up and down.
Motion sickness—that dreadful feeling of dizziness and nausea that sometimes causes vomiting—is thought to be caused by a mismatch between sensory input from the vestibular apparatus and sensory input from the eyes. For example, you may be one of the many people who get carsick from reading in the car. When looking down at a book, your eyes tell your brain that your body is stationary. However, as the car changes speed, turns, and hits bumps in the road, your vestibular system is detecting motion. Similarly, seasickness results when the vestibular apparatus tells the brain that your head is rocking back and forth, but the deck under your feet looks level. The brain is somehow confused by the conflicting information, and the result is motion sickness. Staring at the horizon, so you can see that you are moving, can sometimes relieve the feeling. Over-the-counter drugs to prevent motion sickness, such as Dramamine, work by inhibiting the messages from the vestibular apparatus.
Smell and Taste
Smell is perhaps the least appreciated of our senses. You could easily get along without it, but life would not be as interesting. For one thing, about 80% of what we usually think of as the flavor of a food is really detected by our sense of smell. This relationship explains why food often tastes bland when the nose is congested.
You have millions of olfactory (smell) receptors located not in the nostrils but in a small patch of tissue the size of a postage stamp in the roof of each nasal cavity. These receptors are sensory neurons that branch into long olfactory hairs that project outward from the lining of the nasal cavity and are covered by a coat of mucus, which keeps them moist and is a solvent for odorous molecules. The hairs move, gently swirling the mucus. Olfactory receptors, by the way, are one of the few kinds of neuron known to be replaced during life— about every 60 days.
Odor molecules are carried into the nasal cavity in air, dissolve in the mucus, and bind to receptor sites on the hairs of the olfactory receptor cells, thereby stimulating the cells. If a threshold is reached, the message is carried to the two olfactory bulbs of the brain. The olfactory bulbs process the information from the olfactory receptors and pass it on to the limbic system and to the cerebral cortex (see Chapter 8), where it is interpreted. As you might recall, the limbic system is a center for emotions and memory. Thus, we rarely have neutral responses to odors. For example, the perfume industry makes a fortune from the association between scents and sexuality. Odors can also trigger a flood of long-forgotten memories. If your first kiss was near a blooming lilac bush, for instance, a simple sniff of lilac may take you back in time and place.
We have about 1000 types of olfactory receptors, with which we can distinguish about 10,000 odors. Each receptor responds to several odors. Thus, the brain relies on input from more than one type of receptor to identify an odor (Figure 9.15).
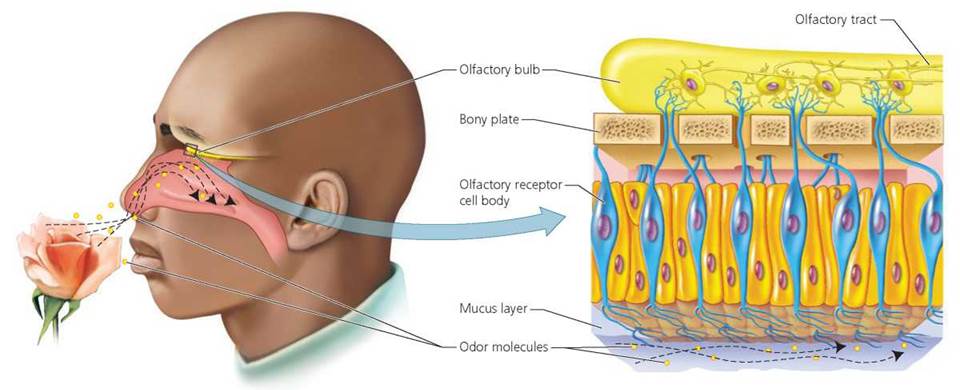
FIGURE 9.15. Our sense of smell resides In a small patch of tissue In the roof of each nasal cavity. Within each cavity are some 5 million olfactory receptors.
There are at least five primary tastes: sweet, salty, sour, bitter, and umami (oo-ma'-mee; savory flavor). These five tastes are enough to answer the important question about food or drink: Should we swallow it or spit it out? We are prompted to swallow if it tastes sweet, because sweetness implies a rich source of calories and thus energy. Salty tastes also prompt swallowing, because salts will replace those lost in perspiration. Sourness may pose a dilemma. Sour is the taste of unripe fruit that would have more food value later on. As fruit ripens, starches break down into sugars that create a sweet taste and mask the sourness. So it is often better to reject sour fruits and wait for them to ripen. However, some sour fruits, such as oranges, lemons, and tomatoes, are rich sources of vitamin C, an essential vitamin. Bitter is easy. We generally reject foods that taste bitter. Bitterness usually indicates that food is poisonous or spoiled. We swallow food if it tastes umami, because it indicates the food is high in protein.
The less widely known fifth taste, umami, is savory or brothy. Umami is derived from a Japanese word that means "delicious." The umami taste occurs when amino acids, especially glutamic acid, small proteins, and nucleotides (DNA and RNA) stimulate umami receptors. The brain interprets input from umami receptors, perhaps with simultaneous input from other receptors as the taste umami. To experience the flavor umami, boil a cup of water with a tablespoon of dried shitake mushrooms. Let it cool and take a sip. Other umami foods include chicken broth, beef broth, and parmesan cheese.
We have about 10,000 taste buds, the structures responsible for our sense of taste. Most taste buds are on the tongue, but some are scattered on the inner surface of the cheeks, on the roof of the mouth, and in the throat. Most taste buds on the tongue are located in papillae, those small bumps that give the tongue a slightly rough feeling. Each papilla contains 100 to 200 taste buds. The cells of a taste bud are completely replaced about every 10 days, so you need not worry about permanently losing your sense of taste when you burn your mouth eating overly hot pizza, as almost always happens.
A taste bud is the meeting point between chemicals dissolved in saliva and the sensory neurons that will convey information about them to the brain. Each taste bud is a lemon-shaped structure containing about 40 modified epithelial cells. Some of these cells are the taste cells that respond to chemicals; others are supporting cells (Figure 9.16). The taste cells have long taste hairs that project into a pore at the tip of the taste bud. These taste hairs bear the receptors for certain chemicals found in food. When dissolved in saliva, food molecules enter the pore and stimulate the taste hairs. Although taste cells are not neurons, they generate electrical signals that are then sent to sensory nerve cells wrapped around the taste cell.
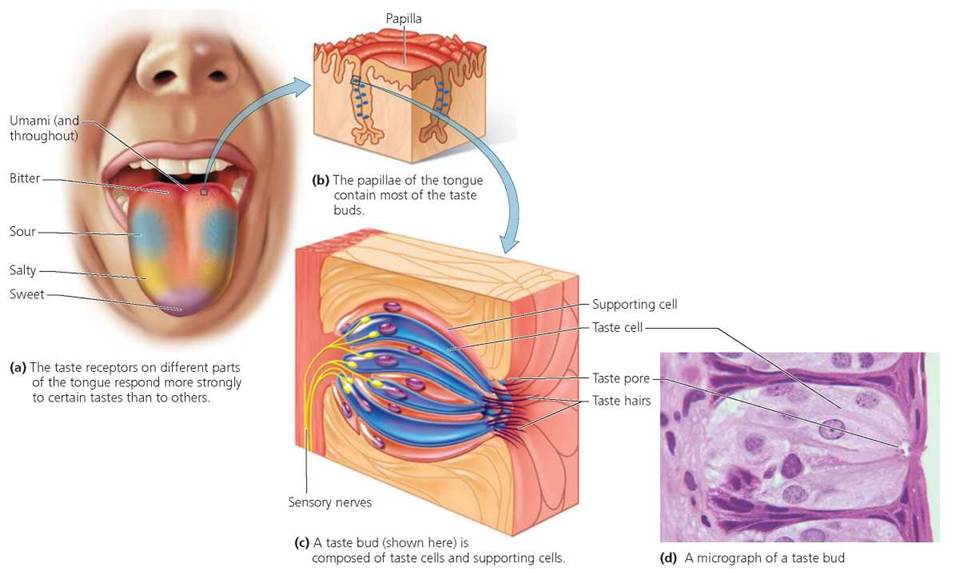
FIGURE 9.16. Taste buds
Each taste bud responds to all five basic tastes but is usually more sensitive to one or two of them than to the others. Because of the way the taste buds are distributed, different regions of the tongue have slightly different sensitivity to these tastes. In general, the tip of the tongue is most sensitive to sweet tastes, the back to bitter, and the sides to sour. Sensitivity to salty tastes is fairly evenly distributed on the tongue. Sensitivity to umami is thought to be distributed throughout the tongue, but it certainly exists at the back of the tongue.
Looking ahead
In the previous chapters we have seen how neurons and the nervous system function to create quick responses to stimuli. In the next chapter we will consider the endocrine system, which produces hormones that cause slower, more prolonged responses within the body.
Highlighting the Concepts
Sensory Receptors (pp. 152-153)
• Changes in external and internal environments stimulate sensory receptors, which in turn generate electrochemical messages that are converted to nerve impulses that are conducted to the brain.
Classes of Receptors (p. 153)
• There are five types of sensory receptors. Mechanoreceptors are responsible for touch, pressure, hearing, equilibrium, blood pressure, and body position. Thermoreceptors detect changes in temperature. Photoreceptors detect light. Chemoreceptors monitor chemical levels within the body and detect smells and tastes.
Pain receptors respond to strong stimuli that cause physical or chemical damage to tissues.
• Some sensory receptors are located near the body surface and respond to environmental changes. Other sensory receptors are located inside the body and monitor internal conditions.
The General Senses (pp. 153-155)
• Touch, pressure, and vibration are monitored by mechanoreceptors: Merkel's disks, Meissner's corpuscles, Pacinian corpuscles, and Ruffini corpuscles.
• Internal and external temperature is monitored by thermoreceptors, which are widely distributed throughout the body.
• Body and limb position is sensed by the mechanoreceptors called muscle spindles and Golgi tendon organs. Muscle spindles are specialized muscle fibers with sensory nerve endings wrapped around them, and Golgi tendon organs are highly branched nerve fibers in tendons.
• Pain receptors, located in almost every tissue of the body, respond to any strong stimulus that results in physical or chemical damage to tissues.
Vision (pp. 155-161)
• The wall of the eye has three layers. The sclera and the cornea make up the outer layer. The choroid, ciliary body, and iris make up the middle layer. The retina, which contains the photoreceptors (rods and cones), is the innermost layer.
• The cornea and the lens work together to focus images on the retina. A normal lens can accommodate (change in shape) to focus on near or distant objects.
• When pigment molecules in the rods or cones (photoreceptors) absorb light, a chemical change occurs in the pigment molecule. The resulting change in the permeability of the membrane of the photoreceptor generates a neural message that is carried by the optic nerve to the brain.
• Color vision depends on the cones. The three types of cones are named for the color of light they absorb best—green, red, or blue—and allow us to see colors.
Hearing (pp. 161-166)
• The ear is divided into three regions: the outer ear, the middle ear, and the inner ear. The outer ear, which functions as a receiver, consists of the pinna and the external auditory canal. The middle ear, which serves as an amplifier, consists of the tympanic membrane (eardrum), three small bones (malleus, incus, and stapes), and the auditory tube. The inner ear is a transmitter and consists of the cochlea and vestibular apparatus.
• Hearing is the sensing of sound waves caused by vibration. Sound enters the outer ear and vibrates the eardrum. These vibrations move the malleus, which moves the incus and the stapes. The stapes conveys these vibrations to the inner ear by means of the oval window.
• Pressure on either side of the eardrum is regulated by the auditory tube.
• The cochlea is a coiled tube enclosed in bone. Its interior is divided into three longitudinal tubes. The middle tube contains the spiral organ (of Corti), which is lined with hair cells and is the portion of the cochlea most responsible for hearing. Sensory hair cells extend from the basilar membrane, which forms the floor of the spiral organ. Vibrations in the oval window cause fluid in the cochlea to move. Movement of the fluid causes the basilar membrane to vibrate and push hair cells into the overlying tectorial membrane, bending hair cells and initiating nerve impulses.
Balance and the Vestibular Apparatus of the Inner Ear (pp. 166-168)
• Balance is controlled by the vestibular apparatus, which consists of the semicircular canals and the vestibule. The semicircular canals monitor sudden movements of the head. The vestibule is made of two components, the saccule and the utricle, which tell the brain the position of the head with respect to gravity.
Smell and Taste (pp. 168-170)
• Olfactory receptors are located in the nasal cavity. They are lined with cilia and coated with mucus. Odorous molecules dissolve in the mucus and bind to the receptors' hairs, stimulating the receptors. Information is passed to the olfactory bulbs and then to the limbic system and the cerebral cortex.
• Taste buds are responsible for our sense of taste. They are on the tongue, inside the cheeks, on the roof of the mouth, and in the throat. They sense the five primary tastes of sweet, salty, sour, bitter, and umami.
Reviewing the Concepts
1. Define sensory adaptation, and give an example. p. 153
2. What are the five classes of receptors? Which would give rise to the general senses? Which would give rise to special senses? p. 153
3. When stimulated, what do Merkel disks tell us? p. 154
4. What are the functions of the two distinct regions of the outer layer of the eye? p. 155
5. How is light focused on the retina? p. 155
6. How is light converted to a neural message? p. 159
7. How are sound waves produced? How are loudness and pitch determined? p. 161
8. What is the function of the eardrum (tympanic membrane)? p. 161
9. Why is it necessary for the force of the vibrations to be amplified in the middle ear? How is amplification accomplished? pp. 161-162
10. What are the effects of unequal air pressure on either side of the eardrum? How does the auditory tube help regulate air pressure? p. 162
11. How does the basilar membrane respond to pitch? p. 163
12. What are the two types of hearing loss? Explain how they differ. p. 165
13. What are the two structures for equilibrium in the inner ear? Explain the structure of each and how it detects body position and motion. pp. 166-168
14. What is believed to cause motion sickness? How can it be counteracted? p. 168
15. Where are the olfactory receptors located? Explain their structure as it is related to their function. p. 168
16. What are the structures responsible for taste? Where are they found? pp. 169-170
17. What are the five primary tastes? p. 168
18. Describe the structure of a taste bud. pp. 169-170
19. Pacinian corpuscles sense
a. pressure.
b. light touch.
c. warmth.
d. pain.
20. The spiral organ (of Corti) is important in sensing
a. body movement.
b. sound.
c. light.
d. degree of muscle contraction.
21. The greatest concentration of cones is found in the
a. sclera.
b. lens.
c. ciliary body.
d. fovea.
22. Noah is a 4-year-old boy who has a middle ear infection. The cause of the infection could be
a. bacteria that spread to the ear from a sore throat.
b. excessive wax buildup in the ear canal.
c. water that was trapped in the ear after bathing.
d. noise pollution.
23. The blind spot of the eye is
a. located in the cornea.
b. the region where the optic nerve leaves the eye.
c. the region of the eye where rods outnumber cones.
d. the region where the ciliary muscle attaches.
24. The receptors responsible for color vision are the _____.
25. The _____ of the eye changes shape to focus.
26. The snail-shaped structure concerned with hearing is the _____.
27. The semicircular canals help us _____.
Applying the Concepts
1. Molly needs glasses for driving but not for reading. What is the name for her visual problem? Describe the shape of the lens she needs to correct her vision.
2. Sarah has a viral infection that is causing vertigo (dizziness). In which part of the ear is the infection?
3. You are at a baseball game. After watching the ball fly into the stands for a home run, you turn to your friend sitting next to you to ask for some peanuts. What changes occur in your eyes for your friend's face to come into focus?
Becoming Information Literate
1. Computer visual syndrome (CVS) is a visual problem common among people who spend long hours in front of a computer. Use at least three reliable sources (books, journals, websites) to identify the causes, symptoms, treatment, and ways to avoid CVS. Cite your sources, and explain why you chose them.
2. Imagine that you are interested in gourmet cooking. Use at least three reliable sources (books, journals, websites) to learn more about the fifth taste, umami. It is not only a taste; it also enhances the other flavors of foods. What natural sources of umami might you add to a dish to enhance its flavor? What beverages might you serve with it to create a true taste delight? Cite your sources, and explain why you chose them.