Biology of Humans
10. The Endocrine System
In Chapters 7, 8, and 9 we learned about the nervous system, which is used for rapid communication. In this chapter, we learn about the endocrine system, which is used for more leisurely communication. Recall that the nervous system sends its messages across synaptic clefts. The endocrine system, in contrast, sends its messages in the bloodstream. We consider the major endocrine glands and the hormones they secrete. These hormones initiate both long-term changes, such as growth and development, and more short-term changes, such as the fight-or-flight response. Because the nervous and endocrine systems share the common function of regulating and coordinating the activities of all body systems, some consider these two systems to be one—and some call it the neuroendocrine system.
Locally Acting Chemical Messengers
Our bodies contain two types of glands: exocrine glands (see Chapter 4) and endocrine glands. Endocrine glands (Figure 10.1) are made of secretory cells that release their products, called hormones. Hormones move from the cells that produced them to the fluid just outside the cells (extracellular fluid), where they diffuse directly into the bloodstream. The endocrine system consists of endocrine glands and of organs that contain some endocrine tissue; these organs have other functions besides hormone secretion. The major endocrine glands are the pituitary gland, thyroid gland, parathyroid glands, adrenal glands, and pineal gland. Organs with some endocrine tissue include the hypothalamus, thymus, pancreas, ovaries, testes, heart, and placenta. Organs of the digestive and urinary systems, such as the stomach, small intestine, and kidneys, also have endocrine tissue.
· The endocrine system produces hormones, substances often described as the chemical messengers of the body. The messages they carry are varied but vital, and include effects on body height, level of alertness, energy production, and fluid balance.
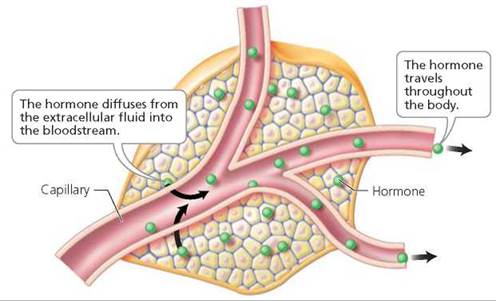
FIGURE 10.1. An endocrine gland. Cells of endocrine glands release their products, called hormones, into the extracellular fluid. The hormones then diffuse into the bloodstream to be transported throughout the body.
Look closely at the structure of the endocrine gland. How does it differ from the structure of an exocrine gland, such as an oil gland?
Endocrine glands lack ducts. Rather than secreting their products into ducts that open to a surface, endocrine glands secrete hormones to the fluid just outside their cells, and from there the hormone moves into the bloodstream.
Our discussion focuses on the major endocrine glands (Figure 10.2). As we describe individual glands, keep in mind that the main function of the endocrine system—like that of the nervous system—is to regulate and coordinate other body systems and thereby maintain homeostasis. We also examine three organs with endocrine tissue: hypothalamus, thymus, and pancreas. The other organs containing endocrine tissue are discussed in the chapters that cover the organs' other functions. For example, the kidneys are discussed in Chapter 16, which covers the urinary system, and the ovaries and testes are discussed in Chapter 17, which covers the reproductive systems.
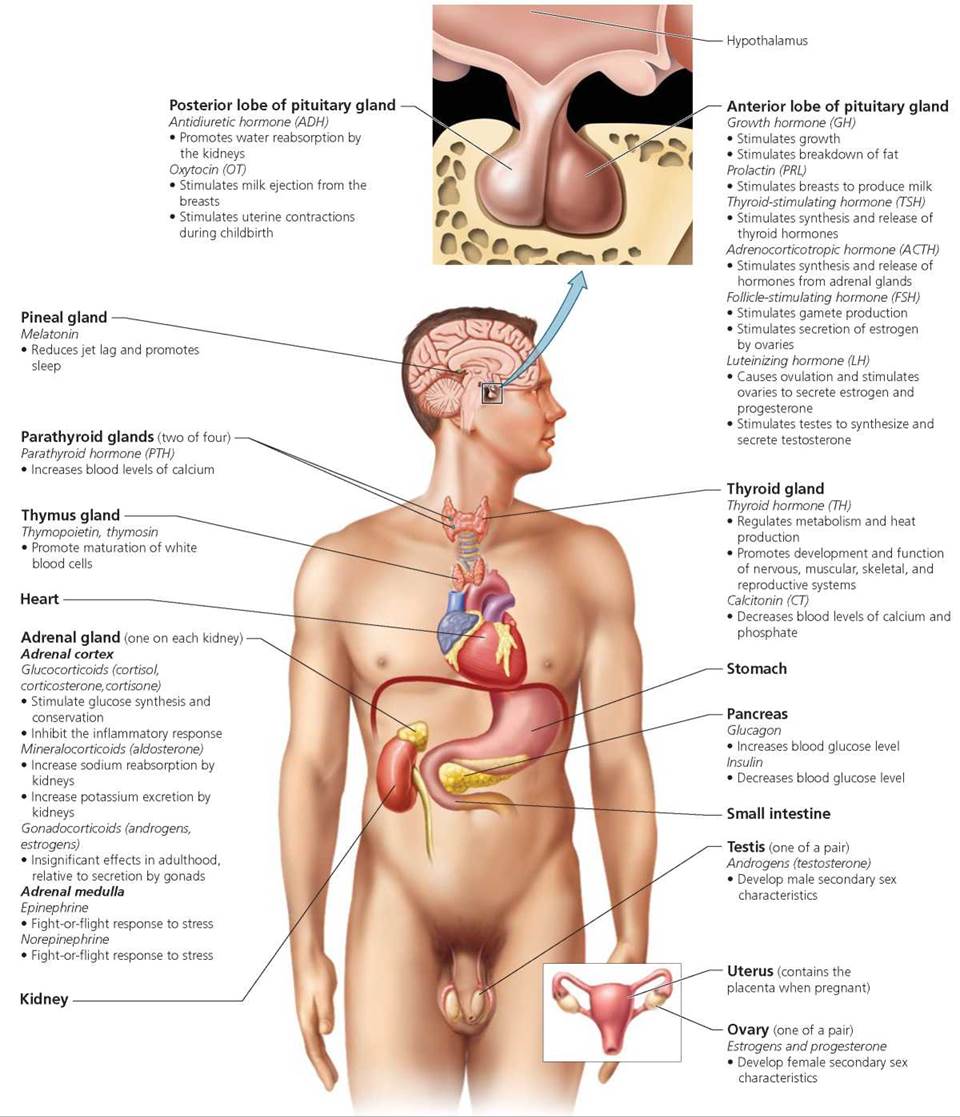
FIGURE 10.2. The endocrine system. The endocrine system is made up of endocrine glands and of organs that contain some endocrine tissue. Here, the hormones and their functions are listed under the endocrine gland or organ that produces them. (Note that hormones secreted by organs for which hormone secretion is a secondary function—the heart, stomach, small intestine, kidneys, testes, ovaries, and uterus with placenta—are discussed in chapters that cover the organs’ other functions.)
Hormones as Chemical Messengers
Hormones are the chemical messengers of the endocrine system. They are released in very small amounts by the cells of endocrine glands and tissues and enter the bloodstream to travel throughout the body. Although hormones come into contact with virtually all cells, most affect only a particular type of cell, called a target cell. Target cells have receptors, protein molecules that recognize and bind to specific hormones. Once a hormone binds to its specific receptor, this hormone-receptor complex begins to exert its effects on the cell. Because cells other than target cells lack the correct receptors, they are unaffected by the hormone.
The mechanisms by which hormones influence target cells depend on the chemical makeup of the hormone. Hormones are classified as being either lipid soluble or water soluble. Lipid- soluble hormones include steroid hormones, a group of closely related hormones derived from cholesterol. The ovaries, testes, and adrenal glands are the main organs that secrete steroid hormones. Lipid-soluble hormones move easily through any cell's plasma membrane because it is a lipid bilayer (see Figure 10.3 on page 176). Once inside a target cell, a steroid hormone combines with receptor molecules either in the cytoplasm or in the nucleus (only target cells have the proper receptors for a given hormone). If binding occurs in the cytoplasm, then the hormone-receptor complex moves into the nucleus of the cell. In the nucleus, the complex attaches to DNA and activates certain genes. Ultimately, such activation leads the target cell to synthesize specific proteins. (The precise steps involved in protein synthesis are described in Chapter 21.) These proteins may include enzymes that stimulate or inhibit particular metabolic pathways.
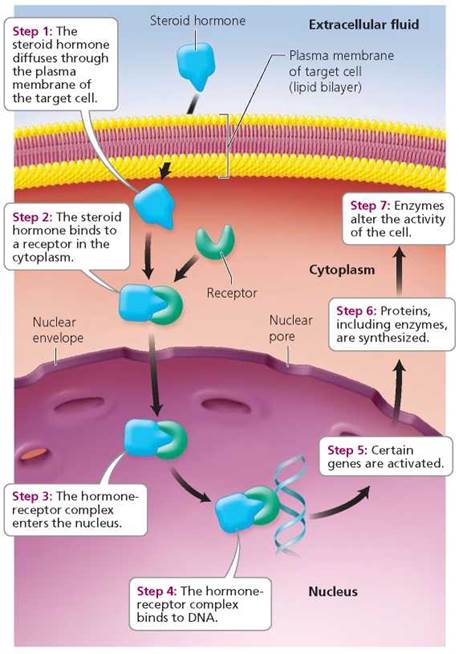
FIGURE 10.3. Mode of action of some lipid-soluble (steroid) hormones. Here, the hormone binds to its receptor in the cytoplasm. In other cases, binding occurs in the nucleus.
Water-soluble hormones, such as protein or peptide hormones, cannot pass through the lipid bilayer of the plasma membrane and therefore cannot enter target cells themselves. Instead, the hormone—which in this situation is called the first messenger—binds to a receptor on the plasma membrane of the target cell. This binding activates a molecule—called the second messenger—in the cytoplasm. Second messengers are molecules within the cell that influence the activity of enzymes, and ultimately the activity of the cell, to produce the effect of the hormone. Cyclic adenosine monophosphate (cAMP) is a common second messenger (illustrated in Figure 10.4 on page 176). As an example of how cAMP functions in its role as a second messenger, we consider the effects of the water-soluble hormone epinephrine on a liver cell. Binding of epinephrine to a receptor on the plasma membrane of a liver cell (the target cell) prompts the conversion of ATP to cAMP within the cell. Cyclic adenosine monophosphate then activates an enzyme within the cell (a protein kinase), which in turn activates another enzyme, and so on. The end result of this enzyme cascade is the activation of an enzyme that catalyzes the breakdown of glycogen to glucose within the liver cell. Thus, whereas lipid-soluble hormones stimulate the synthesis of proteins by a cell, water-soluble hormones like epinephrine activate proteins that are already present in the cell. And water-soluble hormones do this without ever entering the cell.
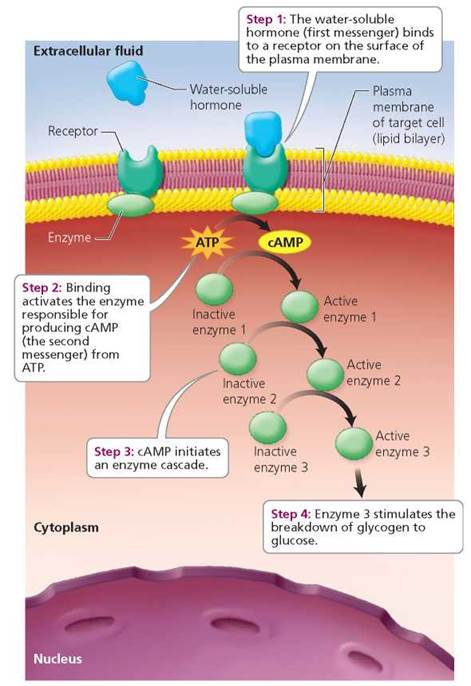
FIGURE 10.4 Mode of action of some water-soluble hormones: the second messenger system of cAMP
We have presented the traditional dichotomy of steroid versus peptide hormones and their different mechanisms of action, but things are never so simple. For example, we describe steroid hormones as binding to receptors inside the cell and modifying gene expression and protein synthesis. These processes may take several hours or days to produce a response. In recent years, steroid hormones have been found to produce more rapid responses, on the order of seconds or a few minutes. Although not fully characterized, steroid effects that occur this rapidly probably do not involve modifications to gene expression and protein synthesis. Also, in these instances, steroid hormones seem to be interacting with membrane receptors rather than receptors inside the cell.
Feedback Mechanisms and Secretion of Hormones
Now that we have seen how hormones work at the cellular level, let's turn our attention to the factors that stimulate and regulate the release of hormones from endocrine glands. Stimuli that cause endocrine glands to manufacture and release hormones include other hormones, signals from the nervous system, and changes in the levels of certain ions (such as calcium, Ca2+) or nutrients (such as glucose) in the blood.
Recall from Chapter 4 that homeostasis keeps the body's internal environment relatively constant. Such constancy most often is achieved through negative feedback mechanisms, which, as we also saw in Chapter 4, are homeostatic mechanisms in which the outcome of a process feeds back to the system, shutting the process down. Negative feedback mechanisms regulate the secretion of most hormones. Typically, a gland releases a hormone, and then rising blood levels of that hormone inhibit its further release. In an alternative form of negative feedback, some endocrine glands are sensitive to the particular condition they regulate rather than to the level of the hormone they produce. For example, the pancreas secretes the hormone insulin in response to high levels of glucose in the blood. Insulin prompts the liver to store glucose, which in turn causes the blood level of glucose to decline. The pancreas senses the low glucose in the blood and stops secreting insulin.
Secretion of hormones is sometimes regulated by positive feedback mechanisms, in which the outcome of a process feeds back to the system and stimulates the process to continue. For example, during childbirth, the pituitary gland releases the hormone oxytocin (OT), which stimulates the uterus to contract.
Uterine contractions then stimulate release of more oxytocin, which stimulates even more contractions (Figure 10.5). The feedback is described as positive because it acts to stimulate, rather than to inhibit, the release of oxytocin. Eventually, some change breaks the positive feedback cycle. In the case of childbirth, expulsion of the baby and placenta terminates the feedback cycle. When we discuss the various glands and their hormones in the sections that follow, we also describe the feedback mechanisms by which they are regulated.
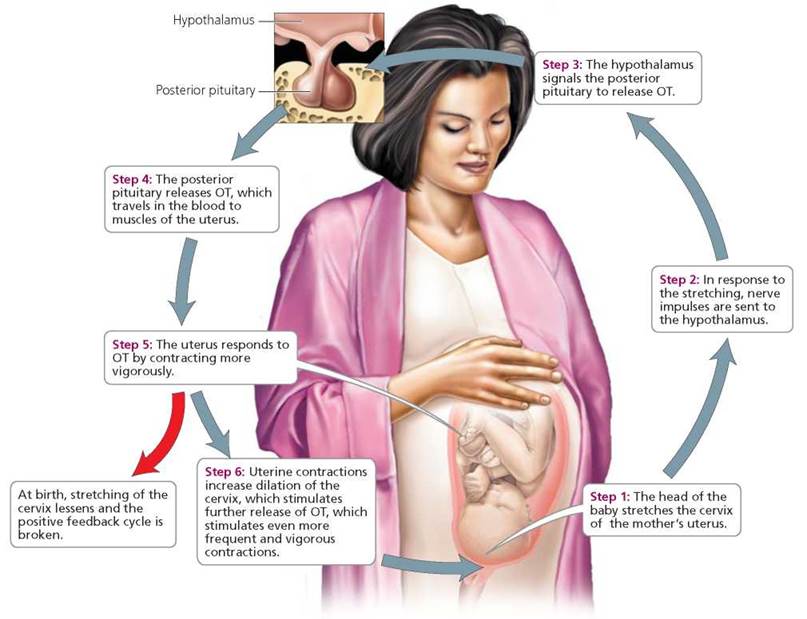
FIGURE 10.5. The positive feedback cycle by which OT stimulates uterine contractions during childbirth
Interactions between Hormones
Interactions between hormones may be antagonistic, synergistic, or permissive. When the effect of one hormone opposes that of another hormone, the interaction is described as antagonistic. For an example of an antagonistic interaction, consider glucagon and insulin, two hormones secreted by the pancreas. Whereas glucagon increases the level of glucose in the blood, insulin decreases the level of glucose in the blood. During synergistic interactions, the response of a tissue to a combination of two hormones is much greater than its response to either individual hormone. For example, epinephrine (from the adrenal glands) and glucagon both prompt the liver to release glucose to the blood. When the two hormones act together, the amount of glucose released by the liver is greater than the combined amount released by each hormone acting alone. During permissive interactions, one hormone must be present for another hormone to exert its effects. For example, thyroid hormone must be present for the hormone aldosterone to stimulate reabsorption of sodium within the tubules of the kidneys.
Next we look at the individual endocrine glands, describing the location and general structure, hormones, and hormonal effects of each. We also consider disorders associated with each gland and its hormones.
Hypothalamus and Pituitary Gland
The pituitary gland is the size of a pea and is suspended from the base of the brain by a short stalk (see Figure 10.2). The stalk connects the pituitary gland to the hypothalamus, the area of the brain that regulates physiological responses like body temperature, sleeping, and water balance. The pituitary gland consists of two lobes: the anterior lobe and the posterior lobe. These lobes differ in size and in their relationship with the hypothalamus. The two lobes release different hormones.
The anterior lobe is the larger one. A network of capillaries runs from the base of the hypothalamus through the stalk of the pituitary. The capillaries connect to veins that lead into more capillaries in the anterior lobe of the pituitary gland (Figure 10.6). This circulatory connection allows hormones of the hypothalamus to control the secretion of hormones from the anterior lobe of the pituitary. Specialized neurons in the hypothalamus synthesize and secrete hormones that travel by way of the bloodstream to the anterior lobe. These specialized neurons are called neurosecretory cells because they generate and transmit nerve impulses and make and secrete hormones. In effect, these cells function as neurons and as endocrine cells, providing a good example of the close relationship between the nervous and endocrine systems. Once these hormones from the hypothalamus reach the anterior pituitary, they stimulate or inhibit hormone secretion. Substances produced by the hypothalamus that stimulate hormone secretion by the anterior pituitary are called releasing hormones. Those that inhibit hormone secretion by the anterior pituitary are called inhibiting hormones. The anterior pituitary responds to releasing and inhibiting hormones from the hypothalamus by modifying its own synthesis and secretion of six hormones. These hormones are growth hormone (GH), prolactin (PRL), thyroid-stimulating hormone (TSH), adrenocorticotropic hormone (ACTH), follicle-stimulating hormone (FSH), and luteinizing hormone (LH).
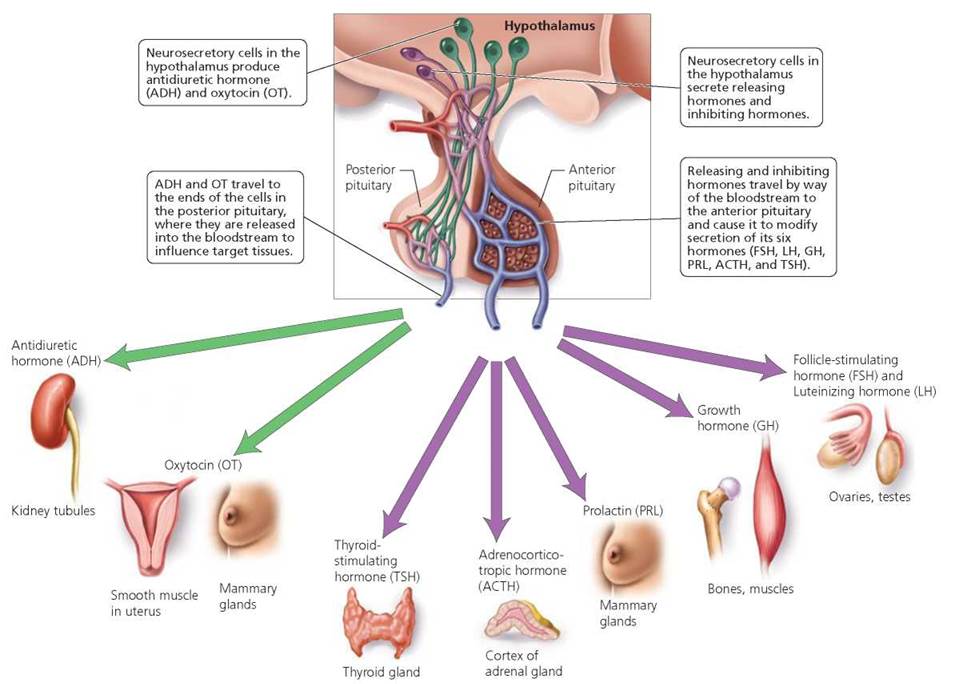
FIGURE 10.6. The two lobes of the pituitary gland and the hormones they secrete
The posterior lobe of the pituitary is very small, just larger than the head of a pin. It consists of neural tissue that releases hormones. In contrast to the circulatory connection between the hypothalamus and the anterior lobe, the connection between the hypothalamus and the posterior lobe is a neural one. As shown in Figure 10.6, neurosecretory cells from the hypothalamus project directly into the posterior lobe. These neurosecretory cells produce oxytocin (OT) and antidiuretic hormone (ADH). OT and ADH move down the axons to the axon terminals of these cells, which are located in the posterior pituitary. OT and ADH are stored in the posterior pituitary until their release into the bloodstream.
Anterior Lobe
As noted, the anterior lobe of the pituitary produces and secretes six major hormones. We begin with growth hormone (GH), the primary function of which is to stimulate growth through increases in cell size and rates of cell division. The target cells of GH are quite diverse. Cells of bone, muscle, and cartilage are most susceptible to GH, but cells of other tissues are affected as well. Growth hormone also plays a role in glucose conservation by making fats more available as a source of fuel.
Two hormones of the hypothalamus regulate the synthesis and release of GH. Growth hormone-releasing hormone (GHRH) stimulates the release of GH. Growth hormone- inhibiting hormone (GHIH) inhibits the release of GH. Through the actions of these two hormones, levels of GH in the body are normally maintained within an appropriate range. However, excesses or deficiencies of the hormone can dramatically affect growth. For example, abnormally high production of GH in childhood, when the bones are still capable of growing in length, results in gigantism, a condition characterized by rapid growth and eventual attainment of heights up to 8 or 9 feet (Figure 10.7). Increased production of GH in adulthood, when the bones can thicken but not lengthen, causes acromegaly (literally, "enlarged extremities"). Acromegaly is characterized by enlargement of the tongue and a gradual thickening of the bones of the hands, feet, and face (Figure 10.8). Both conditions are associated with decreased life expectancy. The excesses of GH that cause such conditions as gigantism and acromegaly may be caused by a tumor of the anterior pituitary. Tumors can be treated with surgery, radiation, or drugs that reduce GH secretion and tumor size. Insufficient production of GH in childhood results in pituitary dwarfism. Typically, pituitary dwarfs are sterile and attain a maximum height of about 4 feet (Figure 10.9). Administering GH in childhood can treat pituitary dwarfism but not other forms of dwarfism.
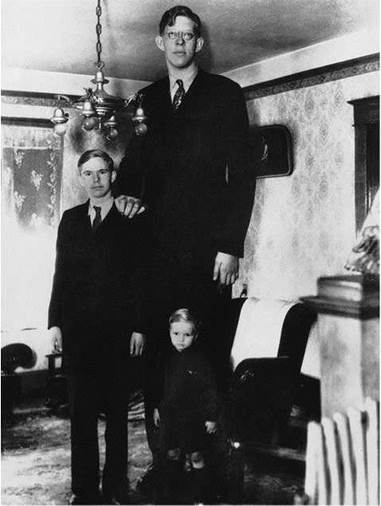
FIGURE 10.7. Robert Wadlow, a pituitary giant, was born in 1918 at a normal size but developed a pituitary tumor as a young child. The tumor caused increased production of GH. Robert never stopped growing until his death at 22 years of age, by which time he had reached a height of 8 feet 11 inches.
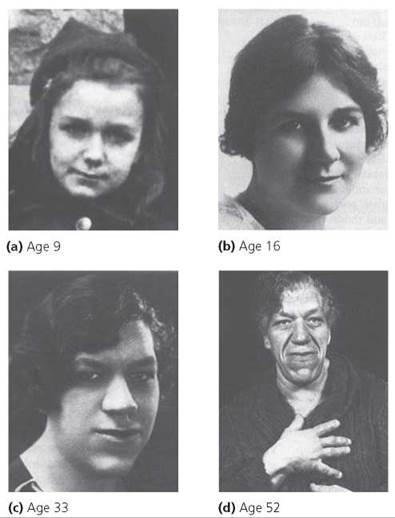
FIGURE 10.8. Acromegaly. Excess secretion of GH in adulthood, when the bones can thicken but not lengthen, causes acromegaly, a gradual thickening of the bones of the hands, feet, and face. The disorder was not apparent in this female at ages 9 or 16, but it became apparent by age 33. The symptoms were even more obvious at age 52.
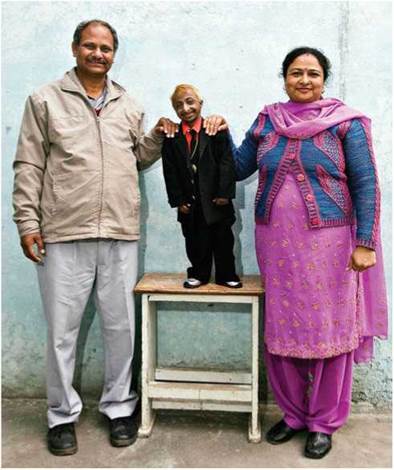
FIGURE 10.9. Pituitary dwarfism is caused by insufficient GH in childhood.
In the past, the use of GH for the treatment of medical conditions (such as pituitary dwarfism) was extremely limited because GH was scarce, given that the hormone had to be extracted from the pituitary glands of cadavers. Beginning in the late 1970s, however, GH could be made in the laboratory. With this greater availability came research on its potential uses in the treatment of aging in adults and below-average height in children. We examine these new uses of GH in the Ethical Issue essay, Hormone Therapy.
Prolactin (PRL), another hormone secreted by the anterior lobe of the pituitary gland, stimulates the mammary glands to produce milk. (Oxytocin, a hormone secreted from the posterior pituitary, causes the ducts of the mammary glands to eject milk, as discussed later in the chapter.) PRL interferes with female sex hormones, which explains why most mothers fail to have regular menstrual cycles while nursing their newborn. (Lactation should not, however, be relied upon as a method for birth control, because the suppression of female hormones and ovulation lessens as mothers breast-feed their growing infants less frequently.)
Growth of a pituitary tumor may cause excess secretion of PRL, which may cause infertility in females, along with production of milk when birth has not occurred. In males, PRL appears to be involved in the production of mature sperm in the testes, but its precise role is not yet clear. Nevertheless, production of too much PRL, as might occur with a pituitary tumor, can cause sterility and impotence in men. Some hormones from the hypothalamus stimulate and others inhibit production and secretion of PRL.
The remaining hormones produced by the anterior lobe of the pituitary gland influence other endocrine glands. A hormone produced by one endocrine gland or organ that influences another endocrine gland is called a tropic hormone. Two such hormones secreted by the anterior lobe of the pituitary are thyroid-stimulating hormone and adrenocorticotropic hormone. Thyroid-stimulating hormone (TSH) acts on the thyroid gland in the neck to stimulate synthesis and release of thyroid hormones. Adrenocorticotropic hormone (ACTH), also called corticotropin, controls the synthesis and secretion of glucocorticoid hormones from the outer portion (cortex) of the adrenal glands (see Figure 10.2).
Two other tropic hormones secreted by the anterior lobe of the pituitary gland influence the gonads (ovaries in the female and testes in the male). Follicle-stimulating hormone (FSH) promotes development of egg cells and secretion of the hormone estrogen from the ovaries in females. Luteinizing hormone (LH) causes ovulation, the release of a future egg cell by the ovary in females. LH also stimulates the ovaries to secrete estrogen and progesterone. These two hormones prepare the uterus for implantation of a fertilized ovum and the breasts for production of milk. In males, FSH promotes maturation of sperm, while LH stimulates cells within the testes to produce and secrete the hormone testosterone.
Ethical Issue
Hormone Therapy
Medical treatment involving hormones is called hormone therapy. Depending on the particular hormone prescribed, the therapy may involve injections, pills, patches, or creams. For example, people with type 1 diabetes mellitus cannot produce the pancreatic hormone insulin. Thus, they need daily injections of insulin to survive. To treat other medical conditions, particular hormones may be blocked or removed. The hormone estrogen promotes the growth of some breast cancers. Thus, blocking the effects of estrogen or lowering estrogen levels may be part of a treatment plan for reducing the risk that breast cancer will return. Drugs, such as tamoxifen, can be used to block the effects of estrogen. Tamoxifen, taken daily as a pill, temporarily blocks the estrogen receptors on breast cancer cells. This action prevents estrogen from binding to the cells. In young women, the ovaries are the main source of estrogen. Thus, estrogen levels can be lowered in young women with breast cancer by surgically removing the ovaries. More commonly, drugs or synthetic hormones are used to shut down production of estrogen by the ovaries.
Using hormones to treat medical conditions such as diabetes or breast cancer is not controversial because the patient could die without medical intervention. However, some hormone therapies do provoke debate. For example, hormone therapy is sometimes used to treat declines in hormone secretion that occur as part of the normal aging process. Recall that growth hormone builds and maintains many tissues, including bone, muscle, and cartilage.
Production of growth hormone by the anterior pituitary gland declines as we age. This decline has prompted some otherwise healthy adults to take synthetic human growth hormone to slow aging. In the United States, human growth hormone requires a doctor's prescription. Nevertheless, it can be purchased in various forms from foreign sources or over the Internet. Relatively few studies have monitored healthy adults taking growth hormone. Results to date indicate that growth hormone injections can increase muscle mass and decrease body fat. The increased muscle mass, however, does not increase strength. In fact, researchers found that strength training with weights was more effective than growth hormone therapy. Side effects of taking growth hormone included muscle, nerve, and joint pain, and swelling of the hands and feet. Elevated blood levels of glucose and cholesterol also have been reported.
Using synthetic growth hormone to treat idiopathic short stature (ISS) in children is quite controversial. ISS is formally defined as short stature without a known cause. It is informally described as “short, but otherwise normal.” Studies monitoring children with ISS who were administered growth hormone typically find that such therapy can yield an additional 1.5 to 3 inches of adult height, although results for individual children vary considerably. So far, the data on ISS patients treated with growth hormone indicate that the treatment is safe. Nevertheless, parents and pediatricians remain concerned about the possible adverse effects that can happen long after the original use of a drug. Opponents of using growth hormone to treat ISS believe it is wrong to give a powerful hormone to healthy children for an essentially cosmetic reason. Rather than administering growth hormone to such children, opponents suggest working to increase societal acceptance of persons who are short. Opponents also point out that growth hormone therapy is invasive, requiring daily injections for several years. Also, growth hormone therapy for ISS is costly. Recent estimates indicate that each inch of height gained costs $35,000 to $52,000.
In the United States, growth hormone is approved for treating certain medical conditions, such as the muscle wasting that occurs with HIV/AIDS. In 2003, the Food and Drug Administration (FDA) approved the use of growth hormone to treat ISS in children whose heights are well below the average for their age and sex. The eligibility criteria established by the FDA made treatment with growth hormone possible for the shortest 1.2% of children. Growth hormone is not approved as an antiaging treatment.
Questions to Consider
• Are you in favor of taking synthetic hormones to replace hormones in our bodies that are naturally declining? Would you advise your parents or grandparents to take growth hormone to slow aging? Why or why not?
• Do you think that human growth hormone should be used to “treat” non-life-threatening conditions such as ISS in children? What would you do if you were the parent of a healthy child who was destined to be very short? What if your child were a pituitary dwarf; would you approve the use of human growth hormone then?
Posterior Lobe
The posterior pituitary does not produce any hormones of its own. However, neurosecretory cells of the hypothalamus manufacture antidiuretic hormone and oxytocin. These hormones travel down the axons of the neurosecretory cells into axon terminals in the posterior pituitary, where they are stored until their release to the bloodstream.
The main function of antidiuretic hormone (ADH) is to conserve body water by decreasing urine output. ADH accomplishes this task by prompting the kidneys to remove water from the fluid destined to become urine. The water is then returned to the blood. Alcohol temporarily inhibits secretion of ADH, causing increased urination following alcohol consumption. The increased output of urine causes dehydration and the resultant headache and dry mouth typical of many hangovers. ADH is also called vasopressin. This name comes from its role in constricting blood vessels and raising blood pressure, particularly during times of severe blood loss.
A deficiency of ADH may result from damage to either the posterior pituitary or the area of the hypothalamus responsible for the hormone's manufacture. Such a deficiency results in diabetes insipidus, a condition characterized by excessive urine production and resultant dehydration. Mild cases may not require treatment. Severe cases may cause extreme fluid loss, and death through dehydration can result. Treatment usually includes administration of synthetic ADH in a nasal spray. Diabetes insipidus (diabetes, overflow; insipidus, tasteless) should not be confused with diabetes mellitus (mel, honey). The latter is a condition in which large amounts of glucose are lost in the urine as a result of an insulin deficiency. Both conditions, however, are characterized by increased production of urine. (We briefly discuss diabetes mellitus later, when we describe the hormones of the pancreas. We describe it in more detail in Chapter 10a.)
Oxytocin (OT) is the second hormone produced in the hypothalamus and released by the posterior pituitary. The name oxytocin (oxy, quick; tokos, childbirth) reveals one of its two main functions: stimulating the uterine contractions of childbirth. As described earlier, the control of OT during labor is an example of a positive feedback mechanism (see Figure 10.5). Pitocin is a synthetic form of OT sometimes administered to induce and speed labor.
The second major function of oxytocin is to stimulate milk ejection from the mammary glands. Milk ejection occurs in response to the sucking stimulus of an infant (Figure 10.10). Recall that prolactin secreted by the anterior pituitary stimulates the mammary glands to produce, but not to eject, milk. Men also secrete OT, and there is some evidence that this hormone facilitates the transport of sperm in the male reproductive tract.
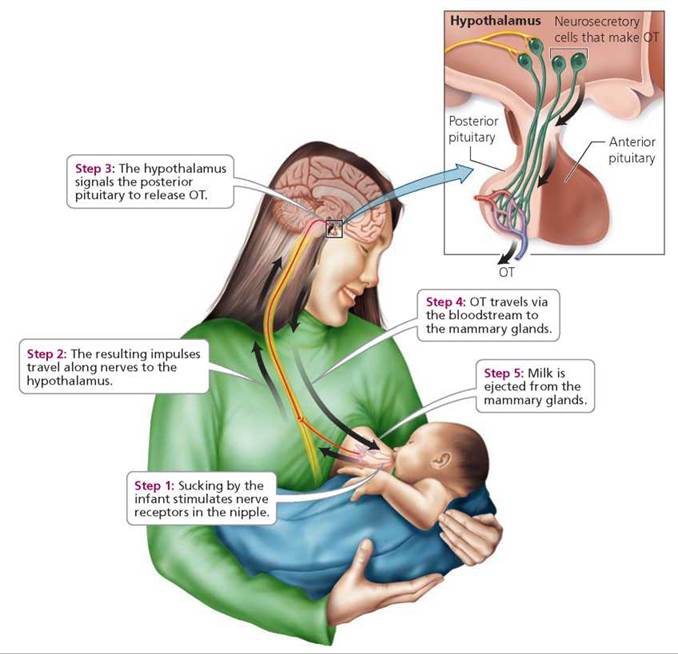
FIGURE 10.10. The steps by which OT stimulates milk ejection from the mammary glands
Stop and think
Women who have just given birth are often encouraged to nurse their babies as soon as possible after delivery. How might an infant's suckling promote completion of, and recovery from, the birth process? Consider that the placenta (afterbirth) must still be expelled after the birth of the baby and that the uterus must return to an approximation of its prepregnancy form.
Thyroid Gland
The thyroid gland is a shield-shaped, deep red structure in the front of the neck, as shown in Figure 10.11a. (The color stems from its exceptional blood supply.) Within the thyroid are small, spherical chambers called follicles (Figure 10.11b). Cells line the walls of the follicles and produce thyroglobulin, the substance from which thyroxine (T4) and triiodothyronine (T3) are made. These two very similar hormones have different numbers of iodine molecules; as indicated by their abbreviations, thyroxine has four iodine molecules and triiodothyronine has three. Thyroxine is usually produced in greater quantity than triiodothyronine, and most thyroxine is eventually converted to triiodothyronine. Because these two hormones are so similar, we will simply refer to them as thyroid hormone (TH). Other endocrine cells in the thyroid, called parafollicular cells (because they occur near the follicles), secrete the hormone calcitonin (Figure 10.11b).
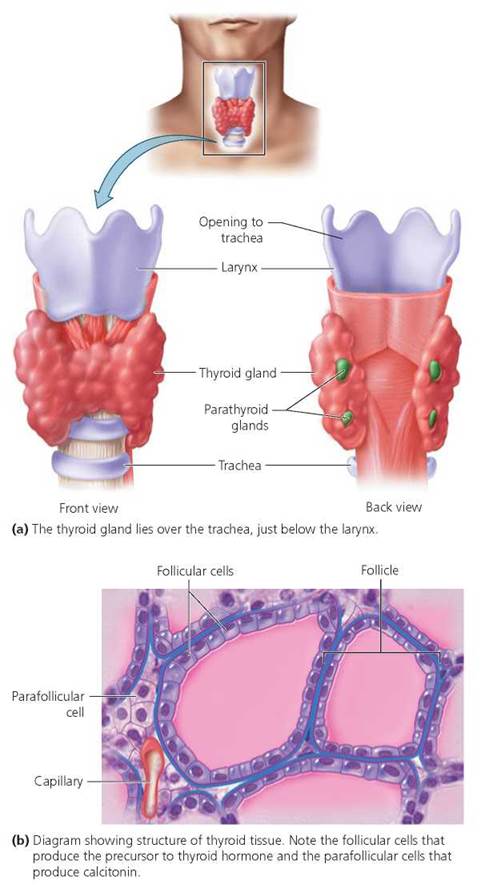
FIGURE 10.11. Location and structure of the thyroid gland and parathyroid glands
Nearly all body cells are target cells for TH. Therefore, it is not surprising that the hormone has broad effects. TH regulates the body's metabolic rate and production of heat. It also maintains blood pressure and promotes normal development and functioning of several organ systems. TH affects cellular metabolism by stimulating protein synthesis, the breakdown of lipids, and the use of glucose for production of ATP (Chapter 2). The pituitary gland and hypothalamus control the release of TH. Falling levels of TH in the blood prompt the hypothalamus to secrete a releasing hormone. The releasing hormone stimulates the anterior pituitary to secrete TSH, which, in turn, causes the thyroid to release more TH.
Iodine is needed for production of TH. A diet deficient in iodine can produce a simple goiter, that is, an enlarged thyroid gland (Figure 10.12a). When intake of iodine is inadequate, the level of TH is low, and the low level of TH in turn triggers secretion of TSH. TSH stimulates the thyroid gland to increase production of thyroglobulin. The lack of iodine prevents formation of TH from the accumulating thyroglob- ulin. In response to continued low levels of TH, the pituitary continues to release increasing amounts of TSH, which cause the thyroid to enlarge in a futile effort to filter more iodine from the blood. In the past, goiters were quite common, especially in parts of the Midwestern United States (dubbed the Goiter Belt), where iodine-poor soil and little access to iodine-rich shellfish led to diets deficient in iodine. The incidence of goiter in the United States dramatically decreased once iodine was added to most table salt beginning in the 1920s. Simple goiter can be treated by iodine supplements or administration of TH.
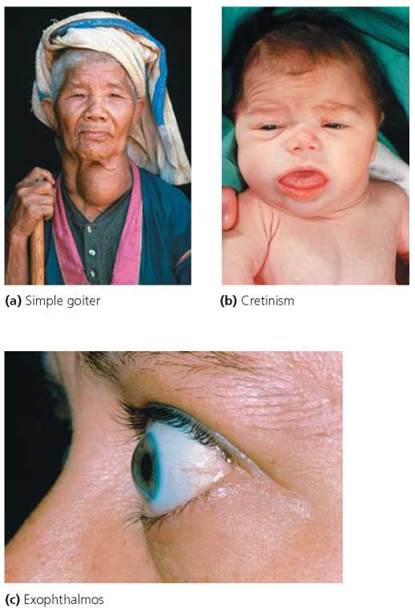
FIGURE 10.12. Disorders of the thyroid gland
Undersecretion of TH during fetal development or infancy causes cretinism, a condition characterized by dwarfism and delayed mental and sexual development (Figure 10.12b). If a pregnant woman produces sufficient TH, many of the symptoms of cretinism do not appear until after birth, when the deficient infant begins to rely solely on its own malfunctioning thyroid gland to supply the needed hormones. Oral doses of TH can prevent cretinism, so most infants in industrialized nations are now tested for proper thyroid function shortly after birth. In the United States, such testing reveals that incomplete development of the thyroid gland occurs in about 1 in every 3000 births. Undersecretion of TH in adulthood causes myxedema, a condition in which fluid accumulates in facial tissues. Other symptoms of TH undersecretion include decreases in alertness, body temperature, and heart rate. Oral administration of TH can prevent and treat these symptoms.
Oversecretion of TH causes Graves' disease, an autoimmune disorder in which a person's own immune system produces Y-shaped proteins called antibodies (discussed in Chapter 13) that in this case mimic the action of TSH. The antibodies stimulate the thyroid gland, causing it to enlarge and overproduce its hormones. Symptoms of Graves' disease include increased metabolic rate and heart rate, accompanied by sweating, nervousness, and weight loss. Many patients with Graves' disease also have exophthalmos, protruding eyes caused by the swelling of tissues in the eye orbits (Figure 10.12c). Graves' disease may be treated with drugs that block synthesis of thyroid hormones. Alternatively, thyroid tissue may be reduced through surgery or the administration of radioactive iodine. Because the thyroid gland accumulates iodine, ingestion of radioactive iodine (usually administered in capsules) selectively destroys thyroid tissue.
The calcitonin (CT) secreted by the parafollicular cells of the thyroid helps regulate the concentration of calcium in the blood to ensure the proper functioning of muscle cells and neurons. Calcium ions bind to the protein troponin, leading to changes in other muscle proteins and eventually causing muscle contraction (Chapter 6). In addition, calcium causes the release of neurotransmitters into the synaptic cleft and therefore is critical in the transmission of messages from one neuron to the next (Chapter 7). When the level of calcium in the blood is high, CT stimulates the absorption of calcium by bone and inhibits the breakdown of bone, thereby lowering the level of calcium in the blood. CT also lowers blood calcium by stimulating an initial increase in the excretion of calcium in the urine. When the level of calcium in the blood is low, the parathyroid glands, which we discuss next, are prompted to release their hormone.
Stop and think
Calcitonin is considered to be most important during childhood, and possibly important at certain times in adulthood, such as during the late stages of a pregnancy. Why might calcitonin be important at these particular times?
Parathyroid Glands
The parathyroid glands are four small, round masses at the back of the thyroid gland (Figure 10.11a, back view). These glands secrete parathyroid hormone (PTH), also called parathormone. As mentioned earlier, CT from the thyroid gland lowers the level of calcium in the blood. In contrast, PTH increases levels of calcium in the blood (see Chapter 5). Low levels of calcium in the blood stimulate the parathyroid glands to secrete PTH, which causes blood levels of calcium to rise. PTH exerts its effects by stimulating (1) bone-destroying cells called osteoclasts that release calcium from bone into the blood, (2) the kidneys to reabsorb more calcium from the filtrate (the fluid inside the nephrons of kidneys, some of which will become urine) and return it to the blood, and (3) the rate at which calcium is absorbed into the blood from the gastrointestinal tract. PTH also inhibits bone-forming cells called osteoblasts and thereby reduces the rate at which calcium is deposited in bone. The feedback system by which CT and PTH together regulate levels of calcium in the blood is summarized in Figure 10.13.
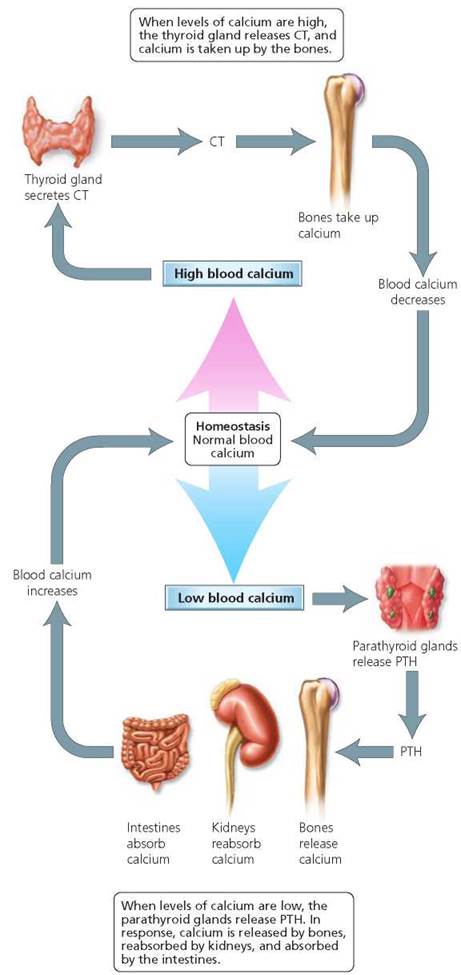
FIGURE 10.13. Regulation of calcium levels in the blood by CT from the thyroid gland (top) and by PTH from the parathyroid glands (bottom)
Surgery on the neck or thyroid gland may damage the parathyroid glands. The resultant decrease in PTH causes decreased blood calcium that in turn produces nervousness and irritability (low calcium is associated with hyperexcitability of the membranes of neurons) and muscle spasms (recall that calcium is also important in muscle contraction). In severe cases, death may result from spasms of the larynx and paralysis of the respiratory system. PTH is difficult to purify, so deficiencies are not usually treated by administering the hormone. Instead, calcium is given either in tablet form or through increased dietary intake.
A tumor of the parathyroid gland can cause excess secretion of PTH. Oversecretion of PTH pulls calcium from bone tissue, causing increased blood calcium and weakened bones. High levels of calcium in the blood may lead to kidney stones, calcium deposits in other soft tissue, and decreased activity of the nervous system.
Adrenal Glands
The body's two adrenal glands (ad, upon; renal, kidney), each about the size of an almond, are located at the tops of the kidneys. Each adrenal gland has an outer and an inner region. The outer region of the gland, the adrenal cortex, secretes more than 20 different lipid-soluble (steroid) hormones, generally divided into three groups: the gonadocorticoids, miner-alocorticoids, and glucocorticoids (Figure 10.14). The inner region, called the adrenal medulla, secretes two water-soluble hormones, epinephrine (also known as adrenaline) and norepinephrine (also known as noradrenaline).
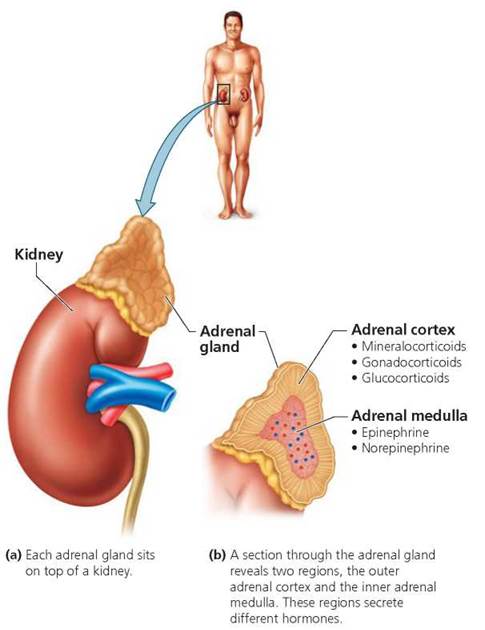
FIGURE 10.14. Location and structure of an adrenal gland
Adrenal Cortex
The gonadocorticoids are male and female sex hormones known as androgens and estrogens. In both males and females, the adrenal cortex secretes both androgens and estrogens. However, in normal adult males, androgen secretion by the testes far surpasses that by the adrenal cortex. Thus, the effects of adrenal androgens in adult males are probably insignificant. In females, the ovaries and placenta also produce estrogen, although during menopause, the ovaries decrease secretion of estrogen and eventually stop secreting it. The gonadocorticoids from the adrenal cortex may somewhat alleviate the effects of decreased ovarian estrogen in menopausal women. Menopause is discussed further in Chapter 17.
The mineralocorticoids secreted by the adrenal cortex affect mineral homeostasis and water balance. The primary mineralocorticoid is aldosterone, a hormone that acts on cells of the kidneys to increase reabsorption of sodium ions (Na+) into the blood. This reabsorption prevents depletion of Na+ and increases water retention. Aldosterone also acts on kidney cells to promote the excretion of potassium ions (K+) in urine. Addison's disease is a disorder caused by the undersecretion of aldosterone and the glucocorticoid cortisol (see the following discussion). This disease appears to be an autoimmune disorder in which the body's own immune system perceives cells of the adrenal cortex as foreign and destroys them. The resulting deficiency of adrenal hormones causes weight loss, fatigue, electrolyte imbalance, poor appetite, and poor resistance to stress. A peculiar bronzing of the skin also is associated with Addison's disease (Figure 10.15). Recall that the pituitary gland secretes ACTH, which stimulates the cortex of the adrenal glands to secrete its hormones. Thus, Addison's disease can also be caused by inadequate secretion of ACTH by the pituitary. Regardless of its cause, Addison's disease can be treated with hormone tablets.

FIGURE 10.15. John F Kennedy suffered from Addison’s disease, which is caused by undersecretion of cortisone and aldosterone from the adrenal cortex. JFK’s complexion showed the peculiar bronzing of the skin characteristic of Addison’s disease.
The glucocorticoids are hormones secreted by the adrenal cortex that affect glucose levels. Glucocorticoids act on the liver to promote the conversion of fat and protein to intermediate substances that are ultimately converted into glucose. The glucocorticoids also act on adipose tissue to prompt the breakdown of fats to fatty acids that are released into the bloodstream, where they are available for use by the body's cells. Glucocorticoids further conserve glucose by inhibiting its uptake by muscle and fat tissue.
Glucocorticoids also inhibit the inflammatory response; such inhibition can be beneficial when the body is faced with the swelling and intense irritation associated with skin rashes such as that caused by poison ivy. One way glucocorticoids inhibit inflammation is by slowing the movement of white blood cells to the site of injury. Another way is by reducing the likelihood that other cells will release chemicals that promote inflammation. Unfortunately, these activities of glucocorticoids inhibit wound healing. Steroid creams containing synthetic glucocorticoids are therefore intended to be applied only to the surface of the skin and to be used for superficial rashes only. These creams should not be applied to open wounds. Some examples of glucocorticoids are cortisol, corticosterone, and cortisone.
Cushing's syndrome results from prolonged exposure to high levels of the glucocorticoid cortisol. Body fat is redistributed, and fluid accumulates in the face (Figure 10.16). Additional symptoms include fatigue, high blood pressure, and elevated glucose levels. A tumor on either the adrenal cortex or the anterior pituitary may cause the oversecretion of cortisol that leads to Cushing's syndrome. (Recall that the anterior pituitary secretes ACTH, which stimulates the release of hormones from the adrenal cortex.) Tumors are treated with radiation, drugs, or surgery. Cushing's syndrome also may result from glucocorticoid hormone treatment for asthma, lupus, or rheumatoid arthritis. Treatment in medically induced cases of Cushing's syndrome typically entails a gradual reduction of the glucocorticoid dose, ideally to the lowest level necessary to control the existing disorder without prompting adverse affects.
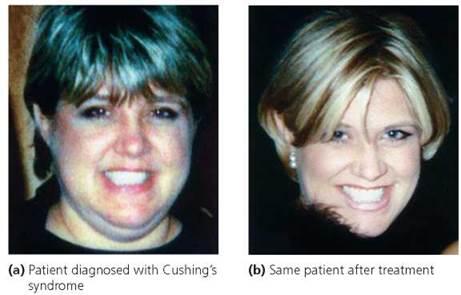
FIGURE 10.16. Cushing’s syndrome. Prolonged exposure to cortisol causes fluid to accumulate in the face. Most often, Cushing’s syndrome is caused by the administration of cortisol for allergies or inflammation.
Stop and think
High blood pressure can signal abnormal aldosterone secretion. Would high blood pressure be associated with the undersecretion or oversecretion of aldosterone?
Adrenal Medulla
As introduced earlier, the adrenal medulla produces epinephrine and norepinephrine. These hormones are critical in the fight-or-flight response, the reaction by the body's sympathetic nervous system to emergencies (Chapter 8). Imagine that you are walking home alone late at night and a stranger suddenly steps toward you from the bushes. Impulses received by your hypothalamus are sent by neurons to your adrenal medulla. These impulses cause cells in your adrenal medulla to increase output of epinephrine and norepinephrine. In response to these hormones, your heart rate, respiratory rate, and blood glucose levels rise. Blood vessels associated with the digestive tract constrict because digestion is not of prime importance during times of extreme stress. Vessels associated with skeletal and cardiac muscles dilate, allowing more blood, glucose, and oxygen to reach them. These substances also reach your brain in greater amounts, leading to the increased mental alertness needed for fleeing or fighting.
In contrast to the near instantaneous response of the sympathetic nervous system to a perceived threat, the hormonal response takes about 30 seconds to mount. This is because epinephrine and norepinephrine must be released by the adrenal medulla, travel in the bloodstream to all cells, bind to receptors on their target cells, and initiate changes in those cells. Even after the danger has passed, we feel the changes brought on by these hormones for a few additional minutes. Epinephrine and norepinephrine thus augment and prolong the response of the sympathetic nervous system to stress. The more leisurely onset and conclusion of the effects of epinephrine and norepinephrine highlight the differences between neural and hormonal systems of internal communication. We explore further how our bodies react to stress in the Health Issue essay, Hormonal Responses to Stress.
Pancreas
The pancreas is located in the abdomen just behind the stomach (Figure 10.17); it contains both endocrine and exocrine cells; the role of the exocrine cells of the pancreas in digestion will be discussed in Chapter 15. The endocrine cells occur in small clusters called pancreatic islets (or islets of Langerhans). These clusters contain three types of hormone-producing cells. One type produces the hormone glucagon; a second produces the hormone insulin; and a third produces the hormone somatostatin. Somatostatin is also secreted by the digestive tract, where it inhibits secretions of the stomach and small intestine, and by the hypothalamus, where it inhibits secretion of growth hormone. The somatostatin secreted by the pancreas may regulate the secretion of glucagon and insulin. However, the precise function of pancreatic somatostatin is not well understood, so we focus on glucagon and insulin.
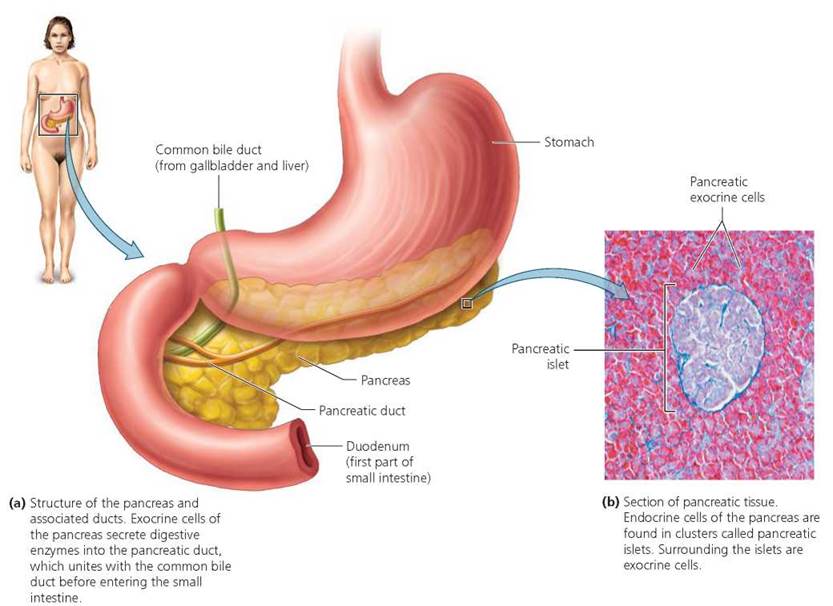
FIGURE 10.17. Location and structure of the pancreas
Between meals, as the level of blood sugar declines, the pancreas secretes glucagon. Glucagon increases the level of blood sugar. It does so by prompting cells of the liver to increase conversion of glycogen (the storage polysaccharide in animals) to glucose (a simple sugar, or monosaccharide). Glucagon also stimulates the liver to form glucose from lactic acid and amino acids. The liver releases the resultant glucose molecules into the bloodstream, causing a rise in blood sugar level.
After a meal, as the level of blood sugar rises with the absorption of sugars from the digestive tract, the pancreas secretes insulin. In contrast to glucagon, insulin decreases glucose in the blood; insulin and glucagon thus have opposite or antagonistic effects. Insulin decreases blood glucose in several ways. First, insulin stimulates transport of glucose into muscle cells, white blood cells, and connective tissue cells. Second, insulin inhibits the breakdown of glycogen to glucose. Third, insulin prevents conversion of amino and fatty acids to glucose. As a result of these actions, insulin promotes protein synthesis, fat storage, and the use of glucose for energy. Figure 10.18 summarizes the regulation of glucose in the blood by insulin and glucagon.
Diabetes mellitus is a group of metabolic disorders characterized by an abnormally high level of glucose in the blood. The high blood glucose levels are caused by problems with either insulin production or insulin function. We explore diabetes mellitus and the dramatic effects of insulin on our health in Chapter 10a.
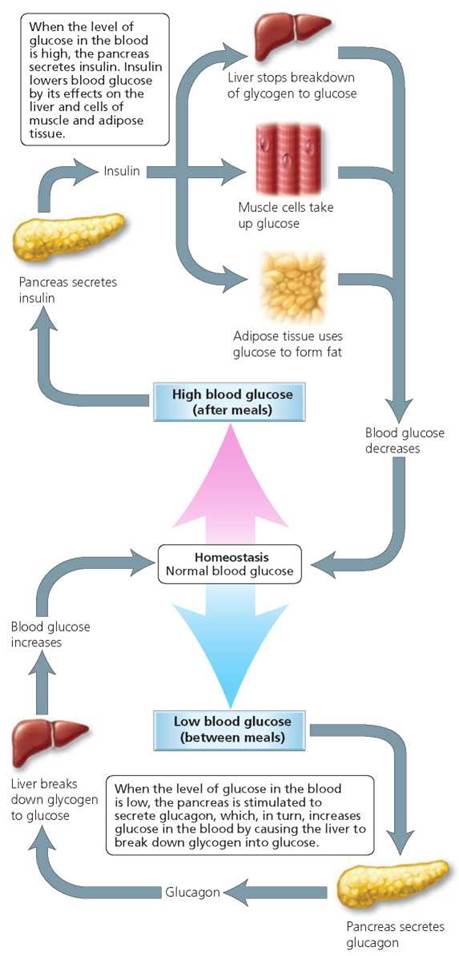
FIGURE 10.18. Regulation of glucose level in the blood by insulin (top) and glucagon (bottom), both of which are secreted by the pancreas
Health Issue
Hormonal Responses to Stress
Stress can be defined broadly as mental or physical tension. Rarely does a day go by that we do not experience stress. Awaiting the start of an exam, some personal performance, or an interview can be stressful. Our bodies usually can deal with everyday stresses and maintain the relative constancy of our internal environment. Sometimes, however, stress is extreme in its intensity and duration, and our coping mechanisms prove inadequate. At such times, stress triggers the hypothalamus to initiate the general adaptation syndrome (GAS), a series of physiological adjustments made by our bodies in response to extreme stress.
The GAS has three phases: alarm, resistance, and exhaustion. The alarm phase is popularly known as the fight-or-flight response. Recall that the fight-or-flight response is initiated by epinephrine from the adrenal medulla. The response immediately funnels huge amounts of glucose and oxygen to the organs most critical in responding to crisis.
Sometimes the adjustments of the alarm phase are sufficient to end or escape whatever is causing the stress. At other times, stress is so intense and long lasting that the individual enters the resistance phase. Changes wrought by the resistance phase are more long term than are those of the alarm phase. Also, rather than being stimulated by nerve impulses from the hypothalamus, the resistance phase is initiated by the release of hormones from the hypothalamus. The released hormones stimulate the anterior pituitary to secrete hormones. In turn, some of these newly secreted hormones stimulate other glands to secrete their hormones. Glucocorticoids from the adrenal cortex are the main hormones of the resistance phase. Two primary effects of glucocorticoids are to mobilize the body's protein and fat reserves and to conserve glucose for use by cells of the nervous system.
The resistance phase is sustained by the body's fat reserves. Once lipid reserves are exhausted, structural proteins are broken down to meet energy demands. Eventually, organs are unable to meet the heavy demands of the resistance phase, and they begin to fail. This is the exhaustion phase. Without immediate attention, death may result from collapse of one or more organ systems.
Stress, especially when it is prolonged and uncontrollable, can dramatically affect our health. It increases our susceptibility to infections and leads to disorders such as hypertension, irritable bowel syndrome, and asthma. Some studies have shown that stress puts people at greater risk for developing chronic diseases. Overall, prolonged stress appears to shorten one's life span.
Given the connection between stress and health, it is important to reduce the stress in our lives. Commonly used means to alleviate the effects of stress include regular exercise and relaxation techniques. A specialized relaxation technique is biofeedback. During a stress biofeedback session, a health care professional connects a patient to a machine that monitors one or more physiological indicators of stress, such as heart rate or muscle tension (Figure 10.A). The health care worker then discusses a stressful situation with the patient. The machine gives off signals when the conversation makes the patient exhibit physiological symptoms of stress. For example, increased tension in muscles might elicit a clicking sound from the machine. The patient can use the clicking sound as a signal of stress, and then practice decreasing the muscle tension that prompted the clicks through deep breathing and relaxation. Eventually, patients are able to recognize and cope with signs of stress without the help of the machine.
FIGURE 10.A. Biofeedback is one way that people can learn to recognize the symptoms of stress and how to cope with them.
Questions to Consider
• Why would Addison's disease, which destroys cells of the adrenal cortex, result in an inadequate stress response? Which phase or phases of the GAS would likely be most affected?
• What means of alleviating stress would you choose and why?
Thymus Gland
The thymus gland lies just behind the breastbone, on top of the heart (see Figure 10.2). It is more prominent in infants and children than in adults because it decreases in size as we age. The hormones it secretes, such as thymopoietin and thymosin, promote the maturation of white blood cells called T lymphocytes. Precursor cells from bone marrow travel by way of the bloodstream to the thymus gland where they mature into T lymphocytes, also known as T cells, to become part of the body's defense mechanisms (Chapter 13).
Pineal Gland
The pineal gland is a tiny gland at the center of the brain (see Figure 10.2). Its secretory cells produce the hormone melatonin. Levels of circulating melatonin are greater at night than during daylight hours, because of input the pineal gland receives from visual pathways. Neurons of the retina, stimulated by light entering the eye, send impulses to the hypothalamus and ultimately the pineal gland, where they inhibit secretion of melatonin.
Research in the past few decades has suggested diverse roles for melatonin. Melatonin may influence daily rhythms. Sleep and, for some people, seasonal changes in mood appear to be influenced by melatonin. Melatonin also may slow the aging process.
One disorder associated with too much melatonin is seasonal affective disorder (SAD). This form of depression is associated with winter, when short day length and a decreased exposure to light results in overproduction of melatonin. Too much melatonin causes symptoms such as lethargy, long periods of sleep, low spirits, and a craving for carbohydrates. The symptoms usually appear around October and end about April in the Northern Hemisphere. Three-quarters of persons who suffer from SAD are female. Treatment of SAD often includes repeated exposure to very bright light for about an hour each day. The intense light inhibits melatonin production.
What would you do?
Scientific evidence indicates that melatonin helps to alleviate jet lag. Studies have shown that melatonin taken by mouth on the day of travel and continued for several days has the following effects in about half the people who take it to fight jet lag: (1) reduced fatigue during the day, (2) reduced time to fall asleep at night, and (3) more rapid development of a normal sleep pattern. Such benefits are usually most evident during eastward travel that crosses more than four time zones. In the United States, melatonin is sold as a dietary supplement, not as a drug. Thus, the regulations of the FDA that apply to medications do not apply to melatonin. Medications must be proven safe and effective for their intended use before they are made available to consumers. Dietary supplements do not require approval by the FDA before reaching the consumer. Instead, it is the manufacturer's responsibility for ensuring that a dietary supplement is safe. If you were scheduled to fly from California to New York for an important interview, would you take melatonin to alleviate jet lag?
Locally Acting Chemical Messengers
Now that we have surveyed the endocrine glands and their hormones, let's consider another group of chemical messengers— those that act locally. Once secreted by a cell, these local signaling molecules act near the site of their release, on adjacent target cells, within seconds or milliseconds. Communication via local signaling molecules occurs much more rapidly than the communication carried out by hormones, which travel to distant sites within the body (recall that the flight-or-fight response may take 30 seconds to initiate physiological changes). Neurotransmitters, discussed in Chapter 7, are examples of chemicals that rapidly convey messages from one cell (a neuron) to a neighboring cell (often another neuron). Prostaglandins, growth factors, and nitric oxide (NO) are other examples of local signaling molecules.
Prostaglandins are lipid molecules continually released by the plasma membranes of most cells. Different types of cells secrete different prostaglandins. At least 16 different prostaglandin molecules function within the human body. These molecules have remarkably diverse effects, influencing blood clotting, regulation of body temperature, diameter of airways to the lungs, and the body's inflammatory response. Prostaglandins also affect the reproductive system. Menstrual cramps are thought to be caused by prostaglandins released by cells of the uterine lining. These prostaglandins act on the smooth muscle of the uterus, causing muscle contractions and cramping. Anti-inflammatory drugs, such as aspirin and ibuprofen, inhibit the synthesis of prostaglandins and thus may lessen the discomfort of menstrual cramps. Prostaglandins also are found in semen. Once in the female reproductive tract, prostaglandins in semen cause the smooth muscles of the uterus to contract, perhaps helping the sperm continue their journey.
Other chemical messenger molecules, called growth factors, are peptides or proteins that, when present in the fluid outside target cells, stimulate those cells to grow, develop, and multiply. For example, one growth factor causes precursor cells in the bone marrow to proliferate and differentiate into particular white blood cells. Another growth factor prompts endothelial cells to proliferate and organize into tubes that eventually form blood vessels (see Chapter 12).
The gas nitric oxide (NO) functions in the cellular communication that leads to the dilation of blood vessels. Basically, endothelial cells of the inner lining of blood vessels make and release NO, which signals the smooth muscles in the surrounding (middle) layer to relax, allowing the vessel to dilate. NO aids in peristalsis, the rhythmic waves of smooth muscle contraction and relaxation that push food along the digestive tract. NO also functions as a neurotransmitter, carrying messages from one neuron to the next. Histamine, another local signaling molecule, is discussed in Chapter 13.
Looking ahead
In Chapter 10 we learned about the hormones produced by endocrine glands and organs with some endocrine tissue. The pancreas is an organ with both endocrine and exocrine tissue. The endocrine cells make and secrete several hormones, among them insulin. In Chapter 10a we focus on diabetes mellitus, a group of diseases characterized by problems in insulin production or function. (The exocrine cells of the pancreas secrete digestive enzymes, which we describe in Chapter 15.)
Highlighting the Concepts
Functions and Mechanisms of Hormones (pp. 173-177)
• Endocrine glands lack ducts and release their products, hormones, into the spaces just outside cells. The hormones then diffuse into the bloodstream. Endocrine glands and organs that contain some endocrine tissue constitute the endocrine system, which regulates and coordinates other organ systems and helps maintain homeostasis.
• Hormones, the chemical messengers of the endocrine system, contact virtually all cells within the body. However, hormones affect only target cells, those cells with receptors that recognize and bind specific hormones.
• Steroid hormones are lipid soluble. Steroids cross through the plasma membrane of target cells and combine with a receptor molecule inside the cell, forming a hormone-receptor complex. In the nucleus, the complex directs synthesis of specific proteins, including enzymes that stimulate or inhibit particular metabolic pathways.
• Water-soluble hormones, many of which are peptides and proteins, cannot pass through the lipid bilayer of the plasma membrane. Thus, they exert their effects indirectly by activating second messenger systems. The hormone, considered the first messenger, binds to a receptor on the plasma membrane. This event activates a molecule in the cytoplasm, considered the second messenger, which carries the hormone's message inside the cell, changing the activity of enzymes and chemical reactions. Thus, whereas lipid-soluble hormones prompt the synthesis of proteins, water-soluble hormones activate existing proteins.
• Endocrine glands are stimulated to manufacture and release hormones by chemical changes in the blood, hormones released by other endocrine glands, and messages from the nervous system. Hormone secretion is usually regulated by negative feedback mechanisms but sometimes by positive feedback mechanisms. The interactions between hormones may be antagonistic, synergistic, or permissive.
Hypothalamus and Pituitary Gland (pp. 177-182)
• The pituitary gland has an anterior lobe and a posterior lobe. The anterior lobe is influenced by the hypothalamus through a circulatory connection. Neurosecretory cells in the hypothalamus release hormones that travel by way of the bloodstream to the anterior lobe, where they stimulate or inhibit release of hormones. The anterior pituitary releases six hormones (growth hormone, GH; prolactin, PRL; thyroid-stimulating hormone, TSH; adrenocorticotropic hormone, ACTH; follicle-stimulating hormone, FSH; and luteinizing hormone, LH). Four (TSH, ACTH, FSH, LH) of the six hormones are tropic hormones, meaning they influence other endocrine glands.
• In contrast to the circulatory connection between the hypothalamus and the anterior lobe of the pituitary gland, the connection between the hypothalamus and the posterior lobe is neural. Neurosecretory cells in the hypothalamus make oxytocin (OT) and antidiuretic hormone (ADH); these two hormones travel down the axons of the cells to axon terminals in the posterior lobe, where they are stored and released.
Thyroid Gland (pp. 182-183)
• The thyroid gland, at the front of the neck, produces thyroid hormone (TH) and calcitonin (CT). Thyroid hormone—which includes two very similar hormones, thyroxine (T4) and triiodothyronine (T3)—has broad effects, including regulating metabolic rate, heat production, and blood pressure. CT maintains low levels of calcium in the bloodstream.
Parathyroid Glands (pp. 183-184)
• The parathyroid glands, four small masses of tissue at the back of the thyroid gland, secrete parathyroid hormone (PTH, or parathormone), an antagonist to CT. As such, PTH is responsible for raising blood levels of calcium by stimulating the movement of calcium from bone and urine to the blood.
Adrenal Glands (pp. 184-186)
• Each of two adrenal glands sits on top of a kidney and has two regions. The adrenal cortex (outer region) secretes gonadocorticoids, mineralocorticoids, and glucocorticoids. The adrenal medulla (inner region) produces epinephrine (adrenaline) and norepinephrine (noradrenaline) that initiate the fight-or-flight response.
Pancreas (pp. 186-188)
• The pancreas secretes the hormones glucagon (increases glucose in the blood) and insulin (decreases glucose in the blood). Diabetes mellitus is a group of disorders characterized by problems with insulin production or function.
Thymus Gland (p. 188)
• The thymus gland lies on top of the heart and plays an important role in immunity. Its hormones influence the maturation of white blood cells called T lymphocytes.
Pineal Gland (p. 188)
• The pineal gland, at the center of the brain, secretes the hormone melatonin. Melatonin appears to be responsible for establishing biological rhythms and triggering sleep.
Locally Acting Chemical Messengers (pp. 188-189)
• Some local chemical messengers convey information between adjacent cells, evoking rapid responses in target cells. Examples of local signaling molecules include neurotransmitters, prostaglandins, growth factors, and nitric oxide.
Reviewing the Concepts
1. Given that hormones contact virtually all cells in the body, why are only certain cells affected by a particular hormone? p. 174
2. How do lipid-soluble (steroid) and water-soluble hormones differ in their mechanisms of action? pp. 174, 176
3. Compare negative and positive feedback mechanisms with regard to regulation of hormone secretion. Provide an example of each. pp. 174-177
4. How do the anterior and posterior lobes of the pituitary gland differ in size and relationship with the hypothalamus? pp. 177-181
5. List the hormones secreted by the anterior lobe of the pituitary and their functions. pp. 178-180
6. List the hormones released by the posterior lobe of the pituitary and their functions. pp. 180-181
7. What are the effects of thyroid hormone? p. 182
8. Describe the feedback system by which calcitonin and parathyroid hormone regulate levels of calcium in the blood. pp. 183-184
9. What are the major functions of the glucocorticoids, mineralo-corticoids, and gonadocorticoids secreted by the adrenal cortex? pp. 184-185
10. What is the fight-or-flight response? Which hormones are critical in initiating this response? p. 186
11. What hormones are secreted by the pancreas? What are their functions? pp. 186-188
12. Explain the differences between diabetes insipidus and diabetes mellitus. pp. 181, 187
13. What is the basic function of hormones secreted by the thymus gland? p. 188
14. What roles might melatonin play in the body? p. 188
15. How do local signaling molecules differ from true hormones? pp. 188-189
16. Which of the following does not characterize the anterior lobe of the pituitary gland?
a. Releases oxytocin and antidiuretic hormone
b. Circulatory connection to the hypothalamus
c. Larger of the two lobes
d. Secretes growth hormone and prolactin
17. A diet deficient in iodine may produce
a. cretinism.
b. Graves' disease.
c. Cushing's syndrome.
d. goiter.
18. Which of the following does not characterize the adrenal medulla?
a. Inner region of the adrenal gland
b. Secretes epinephrine and norepinephrine
c. Secretes glucocorticoids
d. Secretes hormones involved in fight-or-flight response
19. Which of the following does not occur in a healthy person's body after meals?
a. Secretion of insulin by the pancreas
b. Liver stops breakdown of glycogen
c. Secretion of glucagon by the pancreas
d. Muscle cells take up glucose
20. Overproduction of melatonin by the pineal gland may cause
a. seasonal affective disorder.
b. diabetes insipidus.
c. acromegaly.
d. Addison's disease.
21. The traditional dichotomy for hormone action postulates that _____ hormones combine with receptor molecules inside target cells, whereas hormones bind to receptors on the surface of target cells and activate second messengers.
22. Oversecretion of growth hormone in childhood causes _____. Oversecretion in adulthood causes _____.
23. The hormone _____ lowers blood levels of calcium; the hormone increases blood levels of calcium.
24. In males, androgens are produced by the testes and the _____.___________________________
25. The hormone _____ lowers glucose in the blood, whereas the hormone _____ increases glucose in the blood.
Applying the Concepts
1. Mary has an itchy rash on the surface of her skin, and Rick has cut his finger on glass. Would either person benefit from applying a steroid cream containing cortisone? Why? Why not?
2. Which internal system of communication—the endocrine system or nervous system—would be responsible for the growth spurt that occurs at puberty? Which system would control the quick withdrawal of your foot when you step on a tack?
3. It is winter in Massachusetts, and Theresa has felt "down" and lethargic since the fall. She has trouble getting out of bed in the morning, and once up, she craves carbohydrates. What might explain Theresa's symptoms? What might alleviate them, and why?
4. Velma tells her friend Carlos that he produces the female hormone estrogen. Is she correct? If yes, where is the estrogen produced in Carlos? Where is it produced in Velma?
Becoming Information Literate
Recall that undersecretion of thyroid hormone in adulthood causes myxedema and that oversecretion causes Graves' disease. Prepare a brochure in which you describe the symptoms and treatments of these two conditions. Use at least three reliable sources (books, journals, or websites). List each source you considered, and explain why you chose the three sources you used.