Biology of Humans
10a. Diabetes Mellitus
In Chapter 10 we described how two hormones secreted by the pancreas—insulin and glucagon—act antagonistically to regulate the level of glucose in the blood to help maintain homeostasis. Insulin lowers blood glucose levels and glucagon raises blood glucose levels. In this chapter, we consider diabetes mellitus, a group of diseases characterized by problems in insulin production or insulin function. We introduce this group of diseases, describing the different types of diabetes mellitus, and their symptoms, complications, and treatments.
General Characterization and Overall Prevalence
We recognize four basic forms of diabetes mellitus: type 1, type 2, gestational, and "other specific types." Together, types 1 and 2 account for more than 95% of all diagnosed cases. All four forms are characterized by problems in glucose regulation. Glucose is a carbohydrate, specifically a monosaccharide (Chapter 2). Glucose is the main source of fuel for our cells, and we use it to make ATP (Chapter 3). We get glucose directly from the food we eat. After we have eaten a meal, our digestive system breaks down macromolecules, such as complex carbohydrates (polysaccharides), into their simpler components, such as glucose. Glucose is then absorbed into the bloodstream for transport to cells. In response to high levels of glucose in the blood, the pancreas secretes insulin. Insulin promotes the movement of glucose into target cells by stimulating increases in the number of glucose transport proteins in target cell membranes. These proteins then transport glucose into cells by facilitated diffusion (Chapter 3). By stimulating the movement of glucose from the blood into cells, insulin lowers blood glucose levels. As mentioned, all forms of diabetes mellitus are characterized by defects in the production or function of insulin. If there is not enough insulin, or if target cells do not adequately respond to insulin, glucose cannot move from the bloodstream into cells. As a result, glucose reaches abnormally high levels in the blood. We will see that many of the long-term health complications faced by people with diabetes mellitus result from chronic exposure to high levels of blood glucose.
· At present, type 1 diabetes cannot be prevented or cured. Type 2 diabetes, however, can be prevented or delayed by making key lifestyle changes.
Diabetes mellitus is a major cause of death and disability worldwide. In the United States, diabetes was the seventh leading cause of death listed on death certificates in 2006. One year earlier, diabetes appeared on more than 230,000 death certificates as having contributed to deaths listed under other causes, such as cardiovascular disease. Deaths from diabetes are likely much higher than these numbers indicate. Indeed, several studies have shown that numbers gleaned from death certificates seriously underestimate the prevalence of diabetes among those who have died. About 23.6 million Americans alive today (about 7.8% of the population) have diabetes, and annual treatment costs are estimated at $113 billion. In the next 25 years, the total number of Americans with diabetes is predicted to double and the annual costs to nearly triple. Much of the predicted increase in number of cases concerns type 2 diabetes, a form associated with a lifestyle of overeating and inactivity (see the following discussion).
Type 1 and Type 2 Diabetes
Now that we understand the basics of diabetes mellitus and its general prevalence in the population, let's examine the different forms of diabetes. We begin with type 1 and type 2. These two diseases differ from one another in many ways, but they also have some things in common, so we will consider them together and point out their similarities and differences (reviewed in Table 10a.1).
TABLE 10a.1. A Comparison of Type 1 and Type 2 Diabetes Mellitus
Characteristic |
Type 1 |
Type 2 |
Percentage of all diagnosed cases of diabetes |
5-10% |
90-95% |
Previous names |
Juvenile-onset diabetes Insulin-dependent diabetes |
Adult-onset diabetes Non-insulin-dependent diabetes |
Typical age of onset |
< 25 years |
> 40 years, but now appearing at younger ages |
Cause |
Autoimmune reaction destroys the beta cells of the pancreas |
Body cells become resistant to insulin |
Risk factors |
Family history Viral infection |
Family history Obesity Inactivity Member of a high risk population |
Percentage of patients requiring insulin |
100% |
~40% |
Development of ketoacidosis |
Likely if undiagnosed or if treatment is compromised |
Rare |
Treatment |
Insulin; management of diet; exercise |
Some need insulin; some take oral antidiabetic medications; management of diet; exercise |
Prognosis |
Cannot be prevented |
Can be delayed or prevented |
Characterization and Risk Factors
Type 1 diabetes used to be known as insulin-dependent diabetes because taking insulin is always part of treatment. It also was called juvenile-onset diabetes, because it usually develops in people younger than 25 years of age. Type 1 represents about 5% to 10% of all diagnosed cases of diabetes. In this autoimmune disorder, a person's own immune system attacks the cells of the pancreas (called beta cells) responsible for insulin production. A virus may trigger the attack. Some research indicates that infection of beta cells by enteroviruses (common viruses known to cause mild cold symptoms) may trigger the autoimmune response and development of type 1 diabetes. Having a family history of type 1 diabetes is considered a risk factor for development of the disease. Thus, a person has a genetic predisposition for type 1 diabetes, and then an environmental factor, such as a virus, triggers the autoimmune response. Given the destruction of beta cells, people with type 1 diabetes must have insulin delivered by injection or pump (see the discussion on treatments).
Type 2 diabetes used to be known as non-insulin-dependent diabetes because taking insulin is not a requirement of treatment. This name was dropped because about 40% of people with this disease need insulin injections. It was formerly called adult-onset diabetes as well, because it usually develops after age 40, although it recently has begun showing up in younger people who are overweight and sedentary. It is also associated with high blood pressure. Type 2 diabetes accounts for 90% to 95% of diabetes cases. It is characterized by insulin resistance, a condition in which the body's cells fail to adequately respond to insulin.
Obesity is a primary culprit in type 2 diabetes, but the reasons are not fully understood at the molecular level. It appears that increased adipose (fat) tissue interferes with glucose metabolism. One line of research implicates free fatty acids released by fat cells when they break down triglycerides (a type of lipid; see Chapter 2). These free fatty acids travel in the bloodstream, and cells take them up as a source of fuel. Some cells can more easily metabolize free fatty acids than glucose. As a result, they use free fatty acids in preference to glucose, thus disrupting glucose metabolism. Other lines of research implicate other molecules released by adipose tissue, such as hormones and inflammation-promoting proteins. Their links to insulin resistance are the focus of active research.
Exercise uses glucose and makes cells more sensitive to insulin, so failure to exercise (inactivity) is another risk factor for type 2 diabetes. Because we tend to gain weight and exercise less as we age, the risk for developing type 2 diabetes increases with age, especially after 45. Having a parent or sibling with type 2 diabetes places a person at risk for developing it. This could be due to genetic or environmental factors. Additionally, the following populations are disproportionately affected by type 2 diabetes: African Americans, Hispanic/Latino Americans, American Indians, Alaska Natives, Native Hawaiians, and some Asian Americans (Figure 10a.1). In summary, research indicates that type 2 diabetes results from several interacting factors, including obesity, insulin resistance, and failure of the beta cells of the pancreas to fully compensate for the decreased responsiveness to insulin.
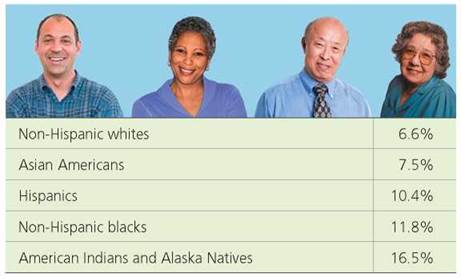
FIGURE 10a.1. Percentages of people with diabetes by race and ethnicity, 2004-2006. These age-adjusted data are from the 2007 National Diabetes Fact Sheet, which is jointly produced by the Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), American Diabetes Association (ADA), and other organizations. These data represent the most recent information available on the prevalence of diabetes by race and ethnicity.
http://www.cdc.gov/Features/dsDiabetes
Symptoms and Complications
Physical symptoms of type 1 diabetes include increased thirst, frequent urination, dry mouth, extreme hunger, unexplained weight loss, fatigue, blurry vision, and sores that are slow to heal. Frequent infections of the gums, skin, bladder, and vagina also occur. A person with type 2 diabetes may not have any of these physical symptoms, or may have some of the symptoms listed for type 1 diabetes.
Diabetes has serious complications. Some complications are acute, which means they develop over a relatively short period of time. Acute complications of diabetes include high blood glucose (hyperglycemia) and low blood glucose (hypoglycemia). High blood glucose is treated by taking insulin (see the following discussion). Taking too much insulin may cause blood glucose to drop to dangerously low levels. Initial symptoms of low blood glucose include anxiety, sweating, hunger, weakness, and disorientation. Because brain cells fail to function properly when starved of glucose, these initial symptoms may be followed by convulsions and unconsciousness. Consequences associated with severe depletion of blood glucose are known collectively as insulin shock. Insulin shock can prove fatal unless blood glucose levels are raised.
Diabetics also may experience acute, life-threatening, biochemical imbalances. These imbalances are much more common in type 1 diabetics than in type 2 diabetics. One such imbalance is diabetic ketoacidosis (DKA). When insulin is unavailable to stimulate the movement of glucose from the blood into cells, the cells become starved of energy. These cells turn to breaking down lipids. Increased breakdown of lipids results in increases in free fatty acids in the blood. The liver metabolizes these fatty acids, producing ketones as a byproduct. Because ketones are acids, they dissociate in solution and release hydrogen ions (Chapter 2). If produced in excess, ketones can overwhelm the body's buffering abilities and cause blood pH to drop. If left untreated, such decreases in blood pH can disrupt normal body functions and cause coma, abnormal heart rhythms, and death. Common triggers of DKA include insufficient home insulin therapy (for example, missed insulin treatments), illnesses or infections (for example, pneumonia or urinary tract infections), stress, physical or emotional trauma, and abuse of alcohol or drugs.
Symptoms of DKA usually develop over a few hours and may include nausea, vomiting, excessive thirst and urination, shortness of breath, weakness, fatigue, and confusion. Sometimes DKA leads to a diagnosis of type 1 diabetes because the symptoms are severe enough that they prompt an undiagnosed person to seek medical attention. Even diagnosed diabetics may fail to recognize DKA because some of its symptoms are typical of other illnesses, such as the flu or foodborne infections (Chapter 2a). To help diabetics recognize this potentially fatal condition, there is a specific over-the-counter test for ketones in urine (ketones in the blood eventually appear in urine, where they can be easily detected with a test strip). Inability to lower blood glucose levels through home insulin therapy is another key feature of DKA. Blood glucose rises because the liver produces glucose in response to the energy crisis (liver cells can make glucose from noncarbohydrates, such as amino acids), but the glucose cannot move into the cells of the body without insulin. People with blood glucose levels consistently higher than 300 mg/dl (milligrams per deciliter), ketones in their urine, and other symptoms of ketoacidosis should seek immediate medical attention. (For reference, normal blood glucose levels are between 70 and 150 mg/dl; over the course of a day, levels fluctuate within this range in response to factors such as size and nutritional composition of meals, exercise, etc.)
Treatment for DKA requires hospitalization and includes intravenous insulin therapy (because home insulin therapy has been unable to lower blood glucose) and fluid replacement (needed to restore body fluids lost through vomiting and excessive urination). Also, because insufficient insulin is associated with decreases in electrolytes (minerals in the blood, such as sodium, potassium, and chloride, that carry an electrical charge), these, too, must be replenished to ensure proper functioning of nerve and muscle cells, including those of the heart.
Other complications of diabetes take years or decades to develop. Over time, high blood glucose is especially damaging to blood vessels, so diabetes can seriously impact the cardiovascular system (heart and blood vessels; Chapter 12). Diabetics are at increased risk for high blood pressure and atherosclerosis, which is the buildup of fatty deposits in the arteries that can lead to heart attack and stroke. Damage to blood vessels affects more than the cardiovascular system. Because blood brings oxygen and nutrients to all cells of the body and removes wastes from them, damage to blood vessels can affect many different tissues, organs, and organ systems. One organ system at risk is the urinary system. High blood glucose can damage the millions of tiny clusters of blood vessels (known as glomeruli) that filter blood in the kidneys. Damage to these vessels can cause kidney failure, necessitating either a kidney transplant or hemodialysis (use of artificial devices to cleanse the blood, Chapter 16). High blood glucose also affects the nervous system and sense organs (Chapters 8 and 9). Many diabetics eventually experience impaired sensation in the hands and feet, when the tiny blood vessels that supply nerves become damaged. Poor circulation and problems with nerves in the lower legs may necessitate amputation of the lower limbs. This is a very common outcome: Diabetics account for more than half of nontraumatic lower limb amputations in the United States. High blood glucose also can damage tiny blood vessels in the retina of the eye; these vessels hemorrhage (rupture) and proliferate abnormally, eventually causing blindness. Other complications that may develop over time include gum disease and skin infections. Finally, diabetics are at increased risk for developing depression. This may reflect, in part, the daily challenges associated with managing this chronic disease (see the following discussion).
Diagnosis
Given the very serious acute and long-term complications, it is important to diagnose and treat diabetes early. In the case of type 2 diabetes, the goal is to prevent it when possible (type 2 diabetes can be prevented or delayed; type 1 diabetes cannot be actively prevented at this time). Several diagnostic blood tests are available. One, called the fasting blood glucose test, involves the collection of a blood sample after an overnight fast. For this test, a blood glucose level of 70 mg/dl to 99 mg/dl is considered normal; a value of 126 mg/dl or higher on two separate tests indicates diabetes. Readings of 100 mg/dl to 125 mg/dl indicate prediabetes, a condition in which blood glucose levels are higher than normal but not high enough for a diagnosis of type 2 diabetes. Another test, the random (nonfasting) blood glucose test, assesses glucose in blood collected at a random time. Diabetes is suggested when a random blood glucose level of 200 mg/dl or higher is found. (Note: The American Diabetes Association provides these blood sugar levels as general guidelines.)
In June 2009, a panel of international experts recommended that testing for type 1 and type 2 diabetes include the glycated hemoglobin A1c test. This blood test indicates a person's average blood glucose level for the past 2 or 3 months. Hemoglobin is the oxygen-carrying pigment found in red blood cells. This test measures the percentage of hemoglobin molecules that have glucose attached. Basically, within red blood cells, glucose reacts with hemoglobin to form glycated hemoglobin. Once a hemoglobin molecule is glycated, it remains that way for the life of the red blood cell (most red blood cells live about 120 days). Thus, the percentage of glycated hemoglobin molecules indicates the average blood glucose level for the past few months. People with diabetes have a higher percentage of glycated hemoglobin than those without diabetes. Specifically, diabetes is indicated by glycated hemoglobin values of 6.5% or higher on two separate tests; for comparison, people without diabetes have readings of 4% to 6%. Prediabetes is indicated by glycated hemoglobin values of 6% to 6.5%.
Treatments
Treatment of type 1 and type 2 diabetes has several components. First, it is essential to maintain a diet that emphasizes foods that are high in nutrition and low in fat and calories (Chapter 15a). Many physicians advise diabetic patients to consult a registered dietician who can help them develop healthy and consistent meal plans. Second, physical activity is critical to lowering levels of blood glucose and increasing sensitivity to insulin. After consulting with their physician to make sure that an exercise program is safe, patients should aim for 30 minutes of aerobic exercise, such as walking or swimming, most days of the week. Healthy meal plans and exercise also are recommended for people diagnosed with prediabetes.
Monitoring blood glucose levels is key to treating type 1 and type 2 diabetes. Depending on the particular treatment plan, glucose levels may need to be checked several times a day, or less frequently. Target glucose levels also depend on the particular treatment plan. Diabetics use glucometers for selftesting blood glucose levels (Figure 10a.2). A glucometer measures the amount of glucose in a drop of blood obtained after a diabetic pricks his or her finger with a lancet. Physicians may recommend glycated hemoglobin A1c testing every few months to assess overall success of the treatment plan (a typical target is having an A1c reading below 7%).
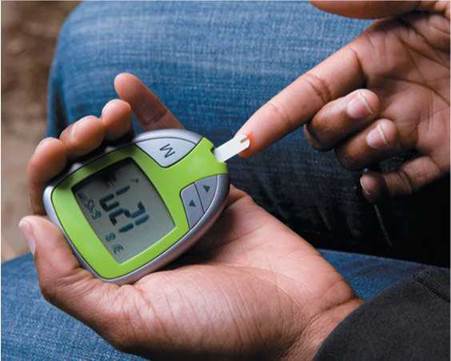
FIGURE 10a.2. A diabetic uses a glucometer to measure the amount of glucose in a drop of blood.
Patients with type 1 diabetes require insulin to survive. Some patients with type 2 diabetes also need insulin. Insulin cannot be taken by mouth because stomach enzymes break it down. Insulin must be injected. This can be accomplished using a needle, syringe, and vial of insulin; an insulin pen (a device that resembles a pen except that the cartridge is filled with insulin rather than ink); or an insulin pump (Figure 10a.3). An insulin pump weighs 3 oz to 4 oz and is typically rectangular in shape, with measurements of 8 x 5 x 2.5 cm (approximately 3 x 2 x 1 in). The pump is worn outside the body. Inside the pump is a reservoir of insulin. A tube connects this reservoir to a catheter inserted under the skin of the abdomen. The device does not measure glucose levels. Instead, it is programmed to dispense specific amounts of insulin, which can be adjusted according to meals, activity, and so on.
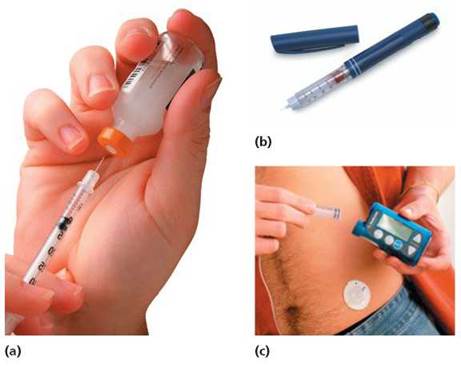
FIGURE 10a.3. There are several methods for self-administration of insulin. (a) Some diabetics use a syringe, fine needle, and vial of insulin, (b) Other diabetics use an insulin pen, which contains a cartridge of insulin. (c) Still other diabetics use an insulin pump, which has a reservoir of insulin inside. A tube connects the reservoir to a catheter inserted under the skin of the abdomen.
Type 2 diabetics and prediabetics at high risk of developing type 2 diabetes may be prescribed oral antidiabetic medications (most type 1 diabetics do not take oral antidiabetic medications). Some of these medications make tissues more sensitive to insulin, and some inhibit production and release of glucose from the liver. Finally, diabetics may take medications to prevent or treat certain long-term complications of diabetes. For example, they may take low-dose aspirin therapy and cholesterol-lowering drugs to help prevent cardiovascular disease.
Medical management of diabetes is clearly a timeconsuming but necessary endeavor for patients. Management can also impose a significant financial burden, especially for diabetics who are uninsured or underinsured.
Lifestyle Changes and Key Recommendations after Diagnosis
A diagnosis of type 1 or type 2 diabetes necessitates many lifestyle changes. These changes include checking blood glucose regularly, taking insulin or oral medication, exercising, planning and eating healthy meals, and being prepared for health emergencies. Successful diabetes management requires a strong commitment from patients. Many patients begin by establishing a relationship with a diabetic educator. Diabetic educators help patients develop daily routines regarding diet, exercise, glucose monitoring, and administration of insulin. They also help when new questions or problems arise in the course of treatment. If a diabetic smokes cigarettes, then quitting is essential because smoking also negatively impacts the cardiovascular system (Chapter 12a). Indeed, smokers who have diabetes are three times more likely to die of cardiovascular disease than are nonsmokers with diabetes. Also, if someone with diabetes chooses to consume alcohol, then it should occur on an occasional basis, with food, and only when his or her diabetes and blood glucose are well controlled. In moderation, alcohol can raise blood glucose. In excess, alcohol can cause blood glucose to drop to dangerously low levels. Stress typically causes higher blood glucose levels and thus is especially problematic for diabetics. Stress also can make it difficult to maintain the daily routines that are critical to managing diabetes. For both of these reasons, diabetics are advised to reduce or eliminate stress whenever possible. It also is recommended that diabetics manage unavoidable stress through relaxation techniques, exercise, and enjoyable activities.
Health care professionals encourage their diabetic patients to follow some key recommendations. One is to wear a diabetic identification tag or bracelet (Figure 10a.4). Such identification can immediately inform medical personnel or others of the existing health condition. This can be critical if a diabetic is unable to communicate, as in the case of insulin shock or very young children who may be unable to describe their condition. Also, anyone who uses insulin should have an emergency kit that contains glucagon. Recall that glucagon is the pancreatic hormone that acts in opposition to insulin to raise blood glucose. If a diabetic loses consciousness due to severely low blood glucose, then a family member or friend can inject glucagon to raise glucose levels. Diabetics who use insulin will often encounter less dramatic episodes of low blood glucose that still require care. For such episodes, a diabetic can drink orange juice or consume glucose tablets to quickly raise blood glucose to acceptable levels. Finally, given all of the long-term complications of diabetes, it is important for diabetics to have regular physical, dental, and eye exams.
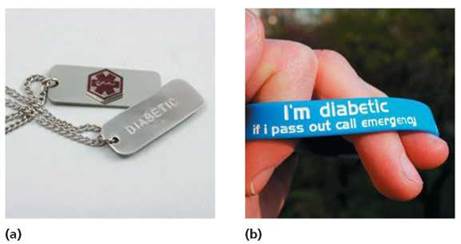
FIGURE 10a.4. It is recommended that diabetics wear a medical ID, so they get appropriate care if they are unable to communicate: (a) medical identification necklace for a diabetic; (b) medical identification bracelet for a diabetic.
Prognoses
At this time, type 1 diabetes cannot be prevented and there is no cure. Nevertheless, strict control of blood glucose can dramatically delay or prevent the cardiovascular, kidney, nerve, and eye complications associated with this disease. Scientists are working to identify genes and environmental factors (e.g., viruses, toxins, and diet) that contribute to type 1 diabetes. Such knowledge may help us understand how to prevent or reverse the autoimmune destruction of insulin-producing cells in the pancreas. Other approaches include transplants of either a whole pancreas or pancreatic islets (clusters of cells that include the beta cells). Drawbacks of transplants include a shortage of available donors and the need for recipients to take immunosuppressive drugs to prevent rejection (these drugs have harmful side effects). Other options being explored are more controversial, and include transplanting pancreatic cells from animals, such as pigs, or from human fetuses made available from terminated pregnancies. Finally, researchers are working to develop an artificial pancreas. This device would monitor blood glucose levels and deliver appropriate amounts of insulin at the right times.
Type 2 diabetes can be prevented or delayed through lifestyle interventions, specifically weight loss and exercise. Without these lifestyle changes, prediabetes can progress to type 2 diabetes in as little as 10 years. Through strict control of blood glucose and blood pressure, patients with type 2 diabetes can reduce their risks of developing long-term complications. Scientists are looking for susceptibility genes for type 2 diabetes. They also are striving to better understand the molecular link between obesity and development of insulin resistance.
What would you do?
One experimental treatment for people recently diagnosed with type 1 diabetes involves the following: (1) removing stems cells from the patient's blood using a blood-filtering machine; (2) administering powerful chemotherapy drugs over several days to knock-out the patient's immune system; and (3) giving the patient an injection of their stem cells to reset their immune system. After the treatment, most of the 23 patients that volunteered for the clinical trial experienced some time (on average, 31 months) when they did not need to take insulin. In other words, their beta cells seemed to function better after the treatment. Monitoring trial participants continues, but early results suggest that the stem cell treatment is not a lifelong cure. Early results also indicate that there are some risks. The treatment requires a 2- to 3-week hospital stay, and patients are vulnerable to infections while their immune system recovers. Many of the treatments that show promise for treating type 1 diabetes involve small clinical trials, such as the one described here. If you were diagnosed with type 1 diabetes, would you volunteer for such a trial? What would you want to know before volunteering?
Gestational Diabetes
When a pregnant woman develops diabetes mellitus it is called gestational diabetes. This condition occurs in about 7% of pregnancies each year. It is more prevalent in certain populations, including African Americans, Hispanic/Latino Americans, and American Indians. Gestational diabetes usually begins in the second half of pregnancy, and it is characterized by progressive insulin resistance. The placenta is the organ that supplies the growing fetus with nutrients and oxygen and carries away wastes and carbon dioxide (Chapter 18). The placenta also produces hormones, some of which make the mother's cells more resistant to insulin. Normally, the mother's pancreas responds by producing more insulin to overcome this resistance. Sometimes, however, her production of insulin is insufficient, and gestational diabetes results. The disease is progressive because the placenta initially increases in size as pregnancy proceeds. This means that production of placental hormones, including those that cause insulin resistance, also increases. In addition, increases in adipose tissue during pregnancy contribute to development of insulin resistance. Risk factors for developing gestational diabetes include family history (having a parent or sibling with type 2 diabetes), personal history (having gestational diabetes in a previous pregnancy), age over 25 years, being overweight before pregnancy, and being a member of a minority or ethnic group with high prevalence for gestational diabetes.
Gestational diabetes typically resolves after delivery because the placenta is expelled soon after the baby is born. Nevertheless, there can be serious health consequences for mother and baby during the pregnancy, at birth, and even thereafter. Some women with gestational diabetes develop preeclampsia during their pregnancy. This is a potentially life-threatening condition characterized by high blood pressure, excess protein in the urine, and fluid retention. The intimate circulatory connection between the mother and developing fetus means that gestational diabetes also has health consequences for the fetus. Recall that insulin resistance means that the mother's cells fail to adequately respond to insulin. This results in high levels of glucose in the blood of the mother. A major function of the placenta is to allow nutrients, such as glucose, to diffuse from the mother's blood into fetal blood. Thus, the extra glucose in maternal blood moves into fetal blood. Unlike glucose, insulin from the mother cannot cross the placenta to help lower blood glucose in the fetus. By about three months gestation, however, the pancreas of the fetus can respond to the high blood glucose, and it does so by producing insulin in excess. Because fetal insulin prompts the movement of glucose from the blood into fetal cells, its overproduction promotes excessive growth in the fetus. As a result, babies born to mothers with gestational diabetes often exhibit excessive birth weight, a condition called macrosomia (macro, large; soma, body). Macrosomia has been defined in several ways. One definition is having a birth weight that lies above the 90th percentile for a particular gestational age. A simpler definition is having a birth weight above about 9 pounds. In any case, excessive fetal growth is associated with difficult deliveries and may necessitate a cesarean section (procedure in which the baby and placenta are removed from the uterus through an incision in the abdominal wall and uterus). After birth, babies born to mothers with gestational diabetes may have low blood glucose (hypoglycemia) because their own production of insulin is so high. In addition to these immediate complications, such babies have an increased risk for developing obesity and type 2 diabetes in childhood and adulthood. Women who have had gestational diabetes are at risk for developing it in a subsequent pregnancy (chances are 33% to 50%) and of developing type 2 diabetes later in life.
Women with gestational diabetes may not experience any physical symptoms or may experience some or all of the symptoms of type 1 and type 2 diabetes. Fortunately, screening for gestational diabetes is usually a part of routine prenatal care. Between 24 and 28 weeks of pregnancy (earlier if a woman is considered at high risk), an expectant mother takes a glucose challenge test in which she drinks a glucose solution and then has blood drawn 1 hour later. If blood glucose is above a certain level (usually 140 mg/dl), then another test is scheduled to confirm gestational diabetes. In this second test, the woman fasts overnight. In the morning, she has blood drawn, after which she drinks a more concentrated glucose solution, and has her blood glucose checked every hour for 3 hours. At least two of the four values (fasting; 1 hour post challenge; 2 hours post challenge; 3 hours post challenge) must be abnormal for the test to be considered positive for gestational diabetes. If gestational diabetes is confirmed, then she works with her physician to develop a treatment plan, which typically includes testing blood glucose levels, eating a healthy diet, and engaging in regular physical activity. If diet and exercise are insufficient to control blood glucose, then some women may need to take insulin or medication. Finally, because women diagnosed with gestational diabetes are at increased risk for developing gestational diabetes in subsequent pregnancies and type 2 diabetes later in life, it is important that they continue to have their blood screened for diabetes and that they make all efforts to prevent development of the disease. The American Diabetes Association recommends an annual fasting blood glucose test.
Stop and think
Is gestational diabetes more similar to type 1 diabetes or type 2 diabetes with respect to causes, risk factors, and treatments?
Other Specific Types of Diabetes
"Other specific types" of diabetes represent only 1% to 2% of all diagnosed cases. These types include insulin deficiencies resulting from damage to the pancreas from disease, infection, drugs, or trauma. As an example, consider the case of Tre F. Porfirio (Figure 10a.5). This 21-year-old serviceman was shot three times in the back by an insurgent in Afghanistan on November 21, 2009. The bullets damaged large portions of Porfirio's gastrointestinal tract, necessitating the removal of his gallbladder, portions of his small and large intestines, and a large section of his pancreas. Following these surgeries at combat hospitals, Porfirio was flown back to the United States for further treatment. Surgeons at the Walter Reed Army Medical Center in Washington, D.C., determined that the part of his pancreas that remained would have to be removed, because it was leaking digestive enzymes. (Recall that in addition to having endocrine cells that produce hormones, the pancreas has exocrine cells that produce digestive enzymes.) Complete removal of the pancreas would eliminate all insulin-producing cells and render Porfirio a severe diabetic. To prevent this, surgeons at Walter Reed removed the remaining section of his pancreas and shipped it to the Diabetes Research Institute at the University of Miami Miller School of Medicine. At the institute, a team of doctors extracted and purified thousands of islets from the pancreas. The islets were then sent to Walter Reed, where they were injected into Porfirio's liver on November 26, 2009. The islets became established in the liver and began producing insulin. It will be necessary for Porfirio to take enzyme pills with meals for the rest of his life (to replace the exocrine function of his pancreas). Nevertheless, his physicians are hopeful that the injected islets cells will provide him with some ability to regulate his blood glucose levels. Tre Porfirio's case is believed to be the first pancreatic autotransplantation (the transplantation of tissues from one part of the body to another within the same individual) following a traumatic injury.

FIGURE 10a.5. Serviceman Tre F. Porfirio received an autotransplant of pancreatic islets cells after his pancreas was removed following traumatic injury. The islet cells from his pancreas were successfully transplanted into his liver, where they began to produce insulin.
Stop and think
Would part of Tre Porfirio's treatment likely include immunosuppressive drugs to prevent rejection? Why or why not?
Looking ahead
In Chapter 10a, we discussed diabetes mellitus, a group of diseases primarily diagnosed through checking levels of glucose in the blood. Blood transports substances other than glucose and has functions beyond transport. In Chapter 11, we take a closer look at blood, and consider its functions and composition, as well as some disorders of red and white blood cells.