Biology of Humans
14. The Respiratory System
In the previous chapters, we learned about the cirsulatory system and cardiovascular disease. We learned that the circulatory system transports oxygen to the cells and carbon dioxide to the lungs. In this chapter, we learn about the roll played by the respiratory system in obtaining oxygen and ridding the body of carbon dioxide. We follow the course of inhaled air to the lungs and describe the mechanics of breathing. We then consider the transport of oxygen and carbon dioxide between the lungs and the cells and examine the control of respiration. Finally, we discuss several disorders of the respiratory system.
Structures of the Respiratory System
Without oxygen, we would die within a few minutes. Why? To stay alive, our cells need energy, and oxygen plays an essential role in extracting energy from food molecules (see Chapter 3). We store the extracted energy by producing a molecule called ATP (adenosine triphosphate), which then releases the energy as needed to do the work of the cell. Our cells can make a little ATP without oxygen, but it is not enough to supply the body's energy needs. Cells can make 18 times more ATP if oxygen is present.
The same chemical reactions that require oxygen for the production of ATP produce carbon dioxide as a by-product. In solution—for example, in water or blood—carbon dioxide forms carbonic acid, which can be harmful to cells.
· Your respiratory system brings in oxygen-laden air and removes carbon dioxide from the body. A healthy respiratory system enhances the quality of life.
The function of the respiratory system is to provide the body with oxygen and to dispose of carbon dioxide, an exchange that also regulates the acidity of body fluids. Four processes play a part in respiration (Figure 14.1).
• Breathing (also called ventilating). Bringing oxygen-rich air into the lungs and moving air laden with carbon dioxide out of the lungs.
• External respiration. The exchange of oxygen and carbon dioxide between the lungs and the blood. Oxygen moves from the lungs into the blood, and carbon dioxide moves from the blood into the lungs.
• Gas transport. Transport of oxygen from the lungs to the cells and of carbon dioxide from the cells to the lungs.
• Internal respiration. The exchange of oxygen and carbon dioxide between the blood and tissue cells. Oxygen moves from the blood to the cells, where it is used in cellular respiration to produce ATP and carbon dioxide. Carbon dioxide produced by the cells moves into the blood.

FIGURE 14.1. An overview of respiration
We begin our exploration of how humans obtain oxygen and dispose of carbon dioxide by following the path of air from the nose to the lungs. The structures the air passes along the way are identified and described in Figure 14.2 and Table 14.1 on page 270. The path the air travels is summarized in Figure 14.3. The respiratory system is generally divided into upper and lower regions. The nose (nasal cavities) and pharynx make up the upper respiratory system. The lower respiratory system consists of the larynx, epiglottis, trachea, bronchi, bronchioles, and lungs.
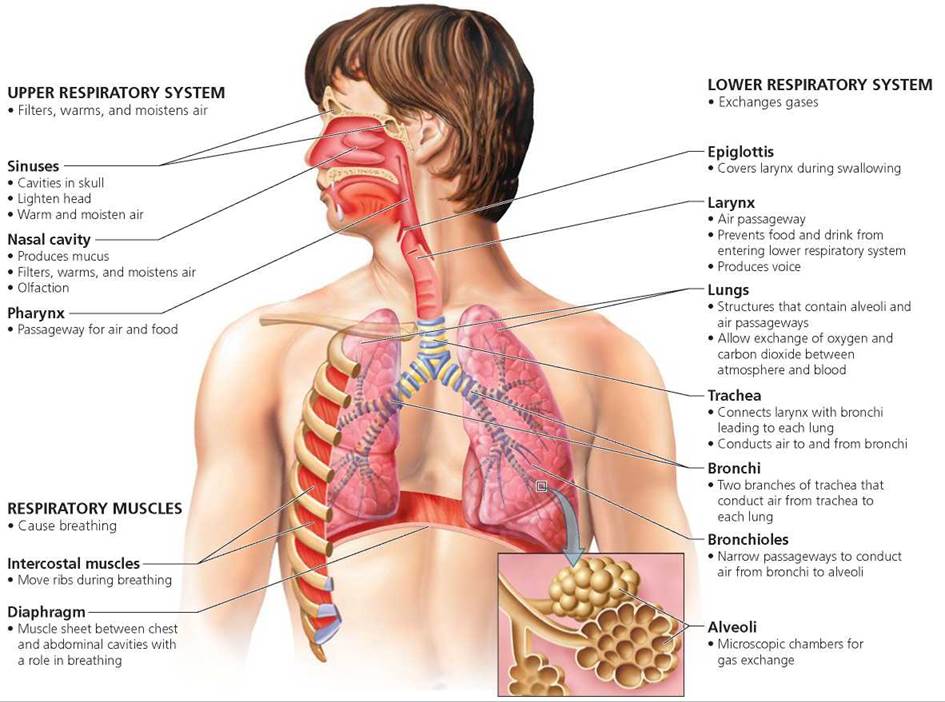
FIGURE 14.2. The respiratory system
Trace the path of oxygen from air entering the nose to the structures in the lungs where oxygen enters the blood supply.
Nasal cavity, pharynx, trachea, bronchi, bronchioles, alveoli
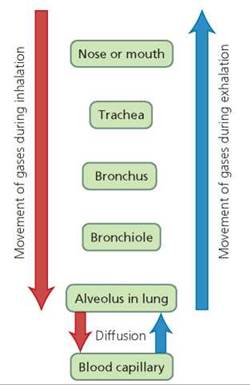
FIGURE 14.3. The path of air during inhalation and exhalation
TABLE 14.1. Review of Structures of the Respiratory System
|
Structure |
Description |
Function |
|
Upper respiratory system |
||
|
Nasal cavity |
Cavity within the nose, divided into right and left halves by nasal septum; has three shelflike bones |
Filters and conditions (moistens and warms incoming air); olfaction (sense of smell) |
|
Sinuses |
Large, air-filled spaces in the bones of the face |
Lessen the weight of the head; warm and moisten inhaled air |
|
Pharynx (throat) |
Chamber connecting nasal cavities to esophagus and larynx |
Common passageway for air, food, and drink |
|
Lower respiratory system |
||
|
Larynx |
Cartilaginous, boxlike structure between the pharynx and trachea that contains the vocal cords and the glottis |
Allows air but not other materials passage to the lower respiratory system; source of the voice |
|
Epiglottis |
Flap of tissue reinforced with cartilage |
Covers the glottis during swallowing |
|
Trachea |
Tube reinforced with C-shaped rings of cartilage that leads from the larynx to the bronchi |
The main airway; conducts air from larynx to bronchi |
|
Bronchi (primary) |
Two large branches of the trachea reinforced with cartilage |
Conduct air from trachea to each lung |
|
Bronchioles |
Narrow passageways leading from bronchi to alveoli |
Conduct air to alveoli; adjust airflow in lungs |
|
Lungs |
Two lobed, elastic structures within the thoracic (chest) cavity containing surfaces for gas exchange |
Exchange oxygen and carbon dioxide between blood and air |
|
Alveoli |
Microscopic sacs within lungs, bordered by extensive capillary network |
Provide immense, internal surface area for gas exchange |
Nose
However large someone's nose might seem from the outside, the inside is not as roomy as you might imagine. One reason is that a thin partition of cartilage and bone called the nasal septum divides the inside of the nose into two nasal cavities. In addition, much of the space within the nasal cavities is taken up by three convoluted, shelflike bones. These bones increase the surface area inside the nasal cavities and divide each cavity into three narrow passageways through which the air flows. Moist mucous membrane covers the entire inner surface of the nasal cavities.
We all know what a nose looks like, but what does a nose do? Your nose has three important functions.
• Filtration and cleansing. The nose helps clear particles from the air that moves through its passages in a variety of ways. Hairs inside the nose filter out the largest particles. In addition, certain cells in the membrane lining the surface of the nasal cavities and air tubules produce mucus, a sticky substance that catches dust particles.
Cilia, tiny projections extending from the membranous lining, then sweep the mucus, trapped dirt particles, and bacteria toward the throat. The trapped particles can then either be swallowed and subsequently destroyed by digestive enzymes or coughed up. Particles that do not become trapped in the nasal cavities or the air tubules are deposited in the lungs. Many of the particles deposited in the lungs are engulfed and removed by macrophages, large irregularly shaped cells that wander across the surfaces of the lungs. However, if too many particles are inhaled or if the mechanisms for removing them fail, the particles may accumulate in the lungs and cover some of the surfaces for gas exchange, reducing their efficiency and setting the stage for infection (Figure 14.4).
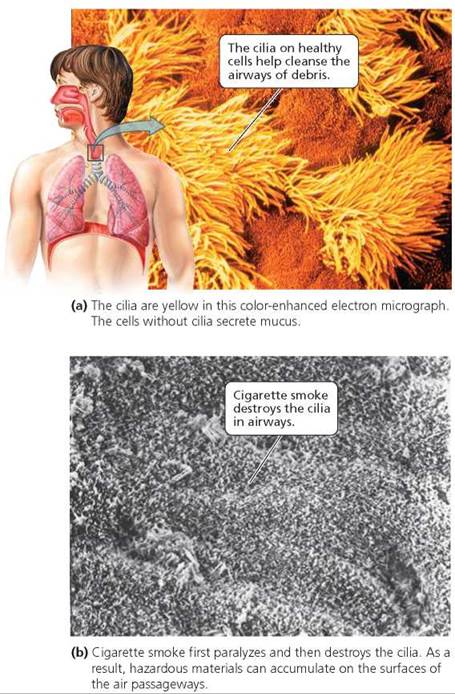
FIGURE 14.4. The respiratory passageways are lined with clumps of short hairlike structures, called cilia, interspersed between mucus-secreting cells.
Conditioning the air. The nose also warms and moistens the inhaled air before it reaches the delicate lung tissues. The blood in the extensive capillary system of the mucous membrane lining the nasal cavity warms and moistens incoming air. The profuse bleeding that follows a punch to the nose is evidence of the rich supply of blood in these membranes. Warming the air before it reaches the lungs is extremely important in cold climates because frigid air can kill the delicate cells of the lung. Moistening the inhaled air is also essential because oxygen cannot cross dry membranes. Mucus helps moisten the incoming air so that lung surfaces do not dry out. Olfaction. Our sense of smell is due to the olfactory receptors located on the mucous membranes high in the nasal cavities behind the nose. The sense of smell is discussed in Chapter 9.
Stop and think
Very cold temperatures can slow the action of the cilia in the nasal cavities. Why does the loss of ciliary action sometimes cause a runny nose on a very cold day?
Sinuses
Connected to the nasal cavities are large air-filled spaces in the bones of the face. These spaces are called the sinuses. Because having these air spaces means less of the head is composed of heavy bone, one advantage of the sinuses is to make the head lighter. The sinuses also help warm and moisten the air we breathe because they, too, are lined with mucous membranes and some incoming air does pass through them. In addition, the sinuses are part of the resonating chamber that affects the quality of the voice. When you have a cold, your voice becomes muffled because the mucous membranes of the sinuses swell and produce excess fluid.
Because the air spaces of the sinuses are connected with those of the nasal cavities, any excess mucus and fluids drain from the sinuses into the nasal cavities. However, when the mucous membranes of the sinuses become inflamed, as they do in sinusitis (-itis, inflammation of), the swelling can block the connection between the nasal cavities and the sinuses, preventing the sinuses from draining the mucous fluid they produce. The pressure caused by the accumulation of fluids in the sinuses causes pain over one or both eyes or in the cheeks or jaws; this condition is usually called a sinus headache. Sinusitis may be caused by the virus responsible for a cold or by a subsequent bacterial infection. Decongestant nasal sprays reduce the swelling in the tubes that connect the sinuses with the nasal cavity, allowing the sinuses to drain more easily—but such sprays should be used only as directed, because they can lead to dependency.
Pharynx
The pharynx, commonly called the throat, is the space behind the nose and mouth. It is a passageway for air, food, and drink. Small, narrow passages, called the auditory (Eustachian) tubes, connect the upper region of the pharynx with the middle ear. These passages help equalize the air pressure in the middle ear with that of the pharynx.
Larynx
After moving through the pharynx, the air next passes through the larynx, which is commonly called the voice box or Adam's apple. The larynx is a boxlike structure composed primarily of cartilage (Figure 14.5).
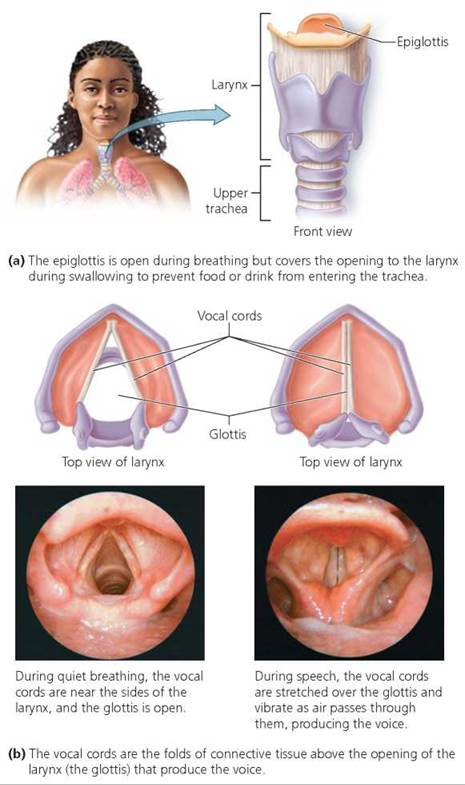
FIGURE 14.5. The larynx, commonly called the voice box or Adam's apple, is an adjustable entryway to the trachea and the source of the voice.
The larynx has two main functions. It is a traffic director for materials passing through the structures in the neck, allowing air, but not other materials, to enter the lower respiratory system. The larynx is also the source of the voice. Let's consider these two functions in more detail.
1. A selective entrance to the lower respiratory system.
The larynx provides a selective opening to the trachea (windpipe) and lower respiratory system: It can be opened to allow air to pass into the lungs and closed to prevent other matter, such as food, from entering the lungs. Because the esophagus (the tube leading to the stomach) is behind the larynx, food and drink must pass over the opening to the larynx to reach the digestive system. If solid material such as food were to enter the lower respiratory system, it could lodge in one of the tubes conducting air to the lungs and prevent air flow. Fluid entering the lungs is equally dangerous because it can cover the respiratory surfaces, decreasing the area available for gas exchange. Normally, foreign material is prevented from entering the lower respiratory system during swallowing because the larynx rises and causes a flap of cartilage called the epiglottis to move downward and form a lid over the glottis, the opening in the larynx through which air passes. You can feel the larynx moving if you put your fingers on your Adam's apple while swallowing. Because of this movement, you cannot breathe and swallow at the same time. (Try it!)
If food or drink accidentally enters the trachea, we usually cough and expel it. However, if food lodges in the trachea, it may block air flow. The Heimlich maneuver can be used to remove the blockage and restore air flow (Figure 14.6).
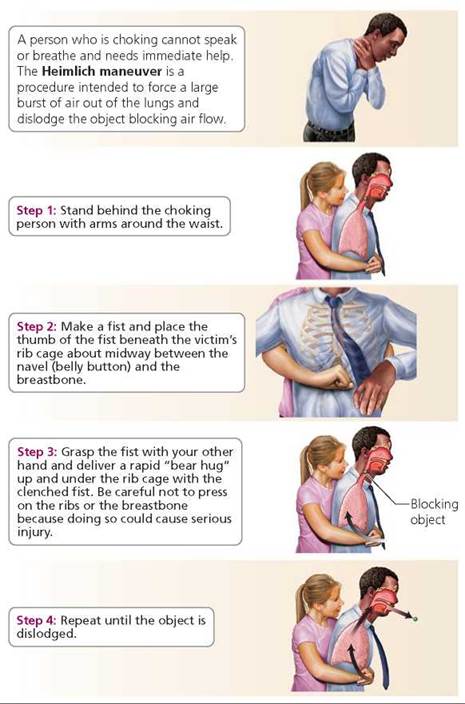
FIGURE 14.6. The Heimlich maneuver can be performed on a choking person who is standing or sitting. If a choking victim is lying on the ground, the same lifesaving pressure changes can be generated by pushing inward and upward on the upper part of the victim’s abdomen. If you begin to choke and there is no one to perform the Heimlich maneuver on you, it may be possible to dislodge the obstruction in your trachea by throwing your upper abdominal region against a table, chair, or other stationary object.
2. Production of voice. The voice is generated in the larynx by the vibration of the vocal cords, two thick strands of tissue stretched over the opening of the glottis (see Figure 14.5). When you speak, muscles stretch the vocal cords across the air passageway, narrowing the opening of the glottis. Air passing between the stretched vocal cords causes them to vibrate and produce a sound, just as the edges of the neck of an inflated balloon vibrate and make noise if you stretch the balloon's neck while allowing air to escape. The vibrations of the vocal cords set up sound waves in the air spaces of the nose, mouth, and pharynx. This resonation is largely responsible for the tonal quality of your voice.
The pitch of the voice depends on the tension of the vocal cords. When the cords are stretched, becoming thinner and tighter, the pitch of the sound when they vibrate is higher. You can demonstrate the relationship between thickness and pitch for yourself by plucking a rubber band stretched between your thumb and forefinger. The more the rubber band is stretched, the higher the pitch of the twang.
When you suffer from laryngitis, an inflammation of the larynx, the vocal cords become swollen and thick. As a result, they cannot vibrate freely, and the voice becomes deeper and huskier. When the vocal cords are very inflamed, a person can hardly speak at all because the cords cannot vibrate in that condition.
Trachea
The trachea, or windpipe, is a tube that conducts air between the outside of the body and the lungs. It is held open by rings of cartilage that give it the general appearance of a vacuum cleaner hose. These rings of cartilage are C-shaped; the open ends of the rings face the side of the trachea next to the esophagus, which allows the esophagus to expand and compress the trachea when a large mass of food is swallowed. You can feel these rings of cartilage in your neck, just below the larynx.
The support rings are necessary in the trachea and its branches to prevent these airways from collapsing during each breath when the rapid flow of air into the lungs creates a drop in pressure. Air (or fluid) passing rapidly over a surface causes a lower pressure, experienced as a "pull," on that surface. Maybe you have noticed that when you get into the shower and turn on the water, the shower curtain is drawn in toward you. The curtain moves inward because the moving water lowers the air pressure, just as the rapid movement of air through the respiratory tubules does. If the trachea were not supported open by cartilage rings, the rapid flow of air during breathing would cause it to collapse or flatten.
Bronchial Tree
The trachea divides into two air tubes called primary bronchi; each bronchus (singular) conducts air from the trachea to one of the lungs. The bronchi branch repeatedly within the lungs, forming progressively smaller air tubes. The smallest bronchi divide to form yet smaller tubules called bronchioles, which finally terminate in alveoli, sacs with surfaces specialized for gas exchange (discussed shortly).
The repeated branching of air tubules in the lung is reminiscent of a branching tree. In fact, the resemblance is so close that the system of air tubules is often called the bronchial tree (Figure 14.7). All the bronchi are held open by cartilage, just as occurs in the trachea. However, the amount of cartilage decreases with the diameter of the tube. The bronchioles have no cartilage, but their walls contain smooth muscle, which is controlled by the autonomic nervous system so that airflow can be adjusted to suit metabolic needs (see Chapter 8).

FIGURE 14.7. A resin cast of the bronchial tree of the lungs. In the body, this branching system of air tubules is hollow and serves as a passageway for the movement of air between the atmosphere and the alveoli, where gas exchange takes place.
Although the contraction of the muscle in bronchial walls is usually closely attuned to the body's needs, sometimes the bronchial muscles go into spasms that severely obstruct the flow of air. Such is the case with asthma, a chronic condition characterized by recurring attacks of wheezing and difficulty breathing. The difficult breathing is worsened by persistent inflammation of the airways. An allergy to substances such as pollen, dog or cat dander (skin particles), and the feces of tiny mites in household dust often trigger asthma attacks. However, a cold or respiratory infection, certain drugs, inhaling irritating substances, vigorous exercise, and psychological stress can also cause an attack. Some attacks start for no apparent reason. Certain inhalants prescribed to treat asthma attacks work by relaxing the bronchial muscles. Other inhalants contain steroids that reduce the inflammation of the air tubules that occurs in asthma.
Alveoli
Each bronchiole ends either with an enlargement called an alveolus (plural, alveoli) or, more commonly, with a grapelike cluster of alveoli. Each alveolus is a thin-walled, rounded chamber surrounded by a dense network of capillaries (Figure 14.8). Oxygen diffuses from the alveoli into the blood, which delivers the oxygen to cells. Carbon dioxide produced by the cells diffuses from the blood into the alveolar air to be exhaled.
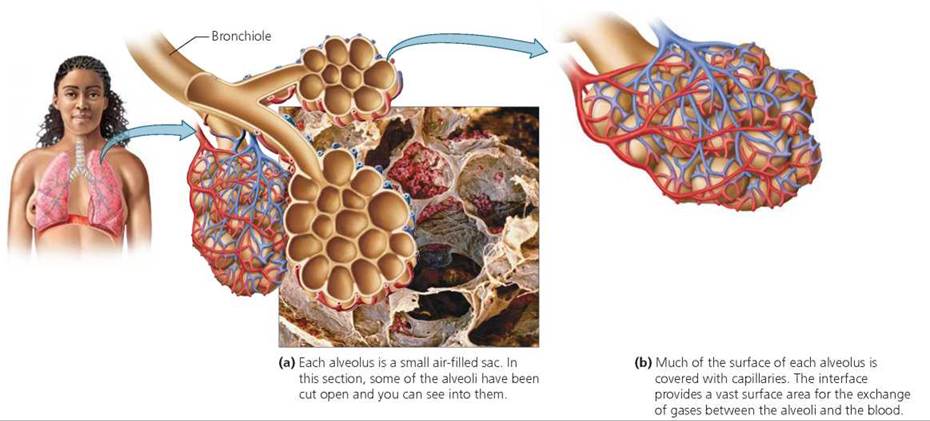
FIGURE 14.8. Alveoli in the lungs create a huge surface area where oxygen and carbon dioxide are exchanged between the lungs and the blood. Oxygen diffuses from the alveoli into the blood, and carbon dioxide diffuses from the blood to the alveoli.
Most of the lung tissue is composed of alveoli, making the structure of the lung much more like foam rubber than like a balloon, the image sometimes used to describe a lung. The surface area inside a simple, hollow balloon the same size as our lungs would be roughly 0.01 m2 (about 0.2 yd2). However, each of our lungs contains approximately 300 million alveoli, whose total surface area is about 70 to 80 m2 (about 84 to 96 yd2). In other words, the alveoli increase the surface area of the lung about 8500 times.
For the alveoli to function properly as a surface for gas exchange, they must be kept open. Phospholipid molecules called surfactant, which coat the alveoli, act to keep them open. Moist membranes, such as those of the alveolar walls, are attracted to one another because of an attraction between water molecules called surface tension. If this attraction were not disrupted by surfactant, it would pull the alveolar walls together, collapsing the air chambers.
Surfactant production usually begins during the eighth month of fetal life, so enough surfactant is present to keep the alveoli open when the newborn takes his or her first breath. Unfortunately, some premature babies have not yet produced enough surfactant to overcome the attractions between the alveolar walls. As a result, their alveoli collapse after each breath. This condition, called respiratory distress syndrome (RDS), makes breathing difficult for the premature newborn. Some newborns with RDS die as a result. However, many are saved by the use of mechanical respirators and artificial surfactant to keep them alive until their lungs mature.
Stop and think
Pneumonia is a lung infection that results in an accumulation of fluid and dead white blood cells in the alveoli. Why might this result in lower blood levels of oxygen?
Mechanism of Breathing
Air moves between the atmosphere and the lungs in response to pressure gradients. It moves into the lungs when the pressure in the atmosphere is greater than the pressure in the lungs, and it moves out when the pressure in the lungs is greater than the pressure in the atmosphere.
The pressure changes in the lungs are created by changes in the volume of the thoracic cavity, a relationship explained by the characteristics of the pleural membrane. Each lung is enclosed in a double-layered sac of pleural membrane. One layer of membrane adheres to the wall of the thoracic cavity; the other adheres to the lung. Fluid between the layers of membrane lubricates the membrane layers and holds them together by surface tension. As a result, a change in the volume of the thoracic cavity causes a similar change in the volume of the lungs. Let's consider how the changes in the size of the thoracic cavity are brought about.
Inhalation
Air moves into the lungs when the size of the thoracic cavity increases; this increase causes the pressure in the lungs to drop below atmospheric pressure. The increase is due to the contraction of both the diaphragm, a broad sheet of muscle that separates the abdominal and thoracic cavities, and the muscles of the rib cage, called the intercostal muscles (costa, rib; Figure 14.9a). The air pressure in the lungs decreases, and air rushes into the lungs. This process is called inhalation, or inspiration. The intercostals lie between the ribs, so that when those muscles contract, they pull the rib cage upward and outward. By placing your hands on your rib cage while you inhale, you can feel the rib cage move up and out. Raising the rib cage increases the size of the thoracic cavity from the front to the back. Meanwhile, the contraction of the diaphragm lengthens the thoracic cavity from top to bottom. This lengthening occurs because the diaphragm is dome-shaped when relaxed, and it flattens when contracted, as shown in Figure 14.9a.
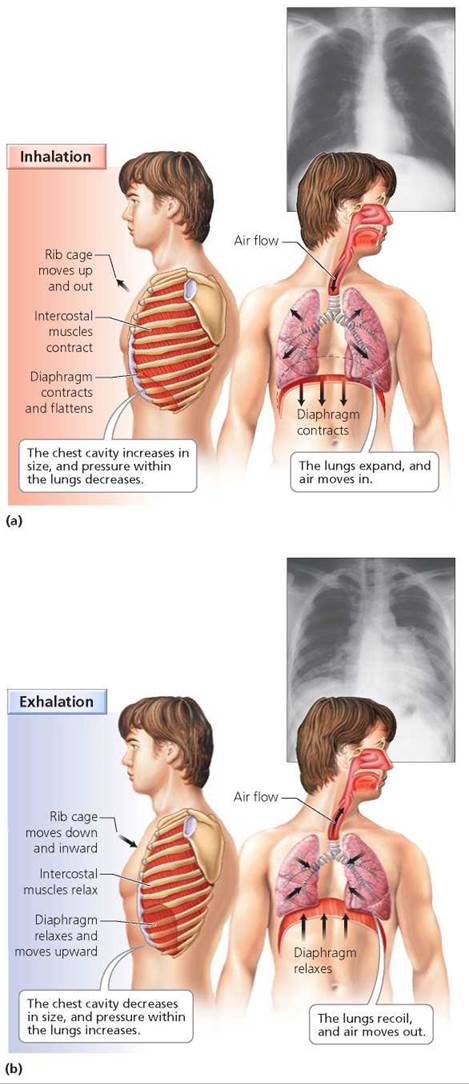
FIGURE 14.9. Changes in the volume of the thoracic cavity bring about inhalation and exhalation. The x-rays show the actual changes in lung volume during inhalation and exhalation.
Exhalation
The process of breathing out, called exhalation or expiration, is usually passive. In other words, it doesn't require work but occurs when the muscles of the rib cage and the diaphragm relax. The lungs are elastic; that is, after stretching they return to their former size. When the elastic tissues of the lung recoil, the rib cage falls back to its former lower position and the diaphragm bulges into the thoracic cavity (Figure 14.9b). The pressure within the lungs increases as the volume of the lungs decreases. When the pressure within the lungs exceeds atmospheric pressure, air moves out.
If it is necessary to exhale more air than usual, as in heavy breathing or coughing, other muscles assist the process. For example, there is another layer of muscles between the ribs. When the rib muscles in this layer contract, they pull the rib cage even further down and inward, increasing the pressure on the lungs. In addition, the muscles of the abdomen can be contracted. Abdominal contractions push the organs in the abdomen against the diaphragm, which causes it to bulge even further into the thorax.
Stop and think
In Victorian times, a woman often wore a corset containing whalebone that formed a band around her waist and lower chest. Corsets were laced tightly to create a wasplike waistline, and women who wore them frequently fainted. What is the most likely cause of these fainting spells?
The Volume of Air Moved Into or Out of the Lungs during Breathing
The volume of air moved during each breath varies from person to person, depending largely on the person's sex, age, and height. During quiet breathing, about 500 ml, or roughly 1 pint, of air moves in and out with each breath. The amount of air inhaled or exhaled during a normal breath is called the tidal volume (Figure 14.10).
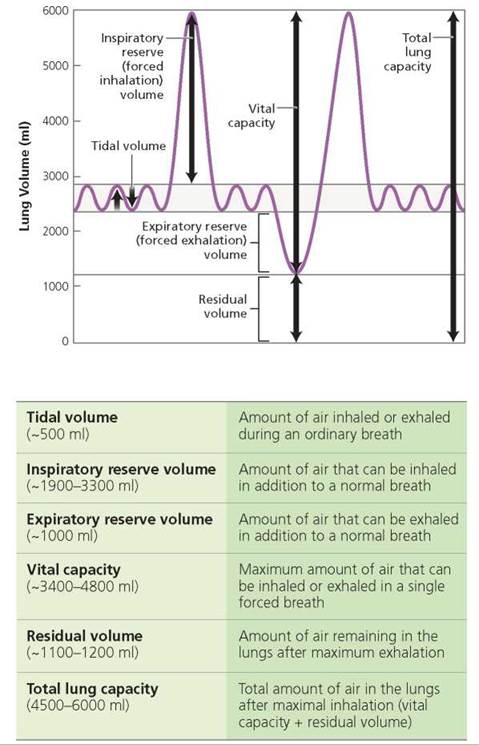
FIGURE 14.10. A spirometer is used to measure the volumes of air in the lungs.
If, after inhaling normally, you were to inhale until you could not take in any more air, you would probably bring another 1900 to 3300 ml of air into your lungs. This volume of air is nearly 4 to 7 times the volume moved during quiet breathing. The additional volume of air that can be brought into the lungs after normal inhalation is called the inspiratory reserve volume.
After you have exhaled normally, you can still force about 1000 ml of additional air from the lungs. This additional volume of air that can be expelled from the lungs after the tidal volume is called the expiratory reserve volume. Decreases in expiratory reserve volume are characteristic of obstructive lung diseases such as bronchitis and asthma. New York City firefighters and other rescue workers at the scene of the collapse of the World Trade Center on September 11, 2001, experienced a significant decrease in expiratory reserve volume in the year following the disaster. The decline in lung function among rescue workers, presumably due to the inhalation of toxic dust, was equivalent to that expected from 12 years of aging. Those who were on the scene when the towers fell, or shortly afterward, suffered the most damage.
If you were to take the deepest breath possible and exhale until you could not force any more air from your lungs, you would be demonstrating your vital capacity, the maximum amount of air that can be moved into and out of the lungs during forceful breathing. The vital capacity, therefore, equals the sum of the tidal volume, the inspiratory reserve, and the expiratory reserve. Although average values for college-age people are about 4800 ml in men and 3400 ml in women, the values can vary tremendously depending on a person's health and fitness. One illness that affects vital capacity is pneumonia. It causes fluid to accumulate within the alveoli, taking up space that would normally be occupied by air.
The lungs can never be completely emptied, even with the most forceful expiration. The amount of air that remains in the lungs after exhaling as much air as possible, called the residual volume, is roughly 1100 to 1200 ml of air. As we will see later in the chapter, emphysema is a lung condition in which the alveolar walls break down, creating larger air spaces that are more difficult to empty. Thus, the residual volume increases. This residual air is lower in oxygen than is inhaled air, so a person with emphysema feels short of breath.
Because some air is always left in the lungs, the vital capacity is not a measure of the total amount of air that the lungs can hold. The total lung capacity, the total volume of air contained in the lungs after the deepest possible breath, is calculated by adding the residual volume to the vital capacity. This volume is approximately 6000 ml in men and 4500 ml in women.
Transport of Gases between the Lungs and the Cells
We have seen that breathing brings air into the lungs and expels air from the lungs. Recall that three other processes then play roles in delivering the oxygen to the cells and disposing of carbon dioxide from the cells. External respiration occurs in the alveoli of the lungs; there, oxygen diffuses into the blood, and carbon dioxide diffuses from the blood. Gas transport is accomplished by the blood, which carries oxygen to the cells and carbon dioxide away from the cells. Internal respiration occurs in the various tissues; there, oxygen diffuses out of the blood and into the cells, and carbon dioxide diffuses out of the cells and into the blood (Figure 14.11).
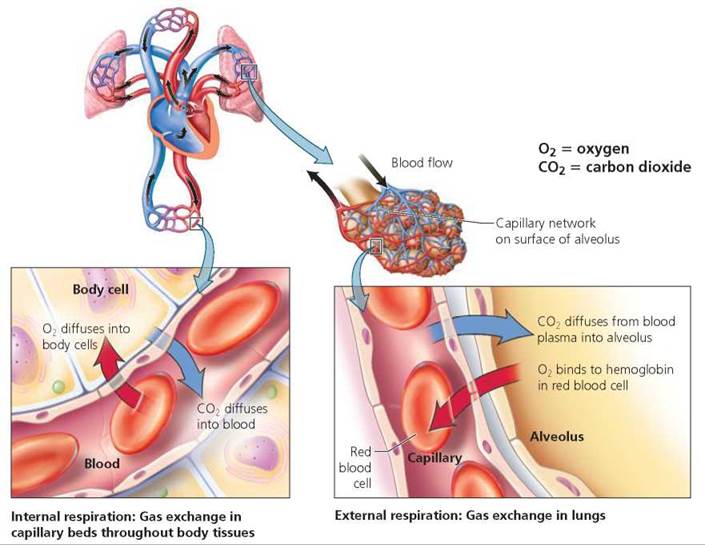
FIGURE 14.11. In the lungs, oxygen diffuses from the alveoli Into the blood. Oxygen Is carried to the cells in red blood cells. At the cells, oxygen diffuses from the blood to the body cells, which use the oxygen and produce carbon dioxide in the process. Carbon dioxide diffuses into the blood and is carried back to the lungs, where it diffuses from the blood into an alveolus and is exhaled.
Oxygen Transport and Hemoglobin
Oxygen is carried from the alveoli throughout the body by the blood. Almost all—about 98.5%—of the oxygen that reaches the cells is bound to hemoglobin, a protein in the red blood cells. Hemoglobin bound to oxygen is called oxyhemoglobin (HbO2). The remaining 1.5% of the oxygen delivered to the cells is dissolved in the plasma. Whole blood, which consists of cells as well as plasma, carries 70 times more oxygen than an equal amount of plasma alone.
Hemoglobin picks up oxygen at the lungs and releases it at the cells. But what determines whether hemoglobin will bind to oxygen or release it? The most important factor deciding this question is the partial pressure of oxygen, which is directly related to its concentration. In a mixture of gases, each gas contributes only part of the total pressure of the whole mixture of gases. The pressure exerted by one of the gases in a mixture is called its partial pressure.
Recall from Chapter 3 that substances always diffuse from regions of higher concentration or pressure to regions of lower concentration or pressure. In the alveoli of the lungs, where the concentration of oxygen is high, hemoglobin in the red blood cells in nearby capillaries picks up oxygen. The oxygen is then released near the cells, where the oxygen concentration is low.
Carbon Dioxide Transport and Bicarbonate Ions
The carbon dioxide produced by cells as they use oxygen is removed by the blood. Carbon dioxide transport occurs in three principal ways:
1. Dissolved in blood plasma. Between 7% and 10% of the carbon dioxide is transported dissolved in the plasma as molecular carbon dioxide.
2. Carried by hemoglobin. Hemoglobin molecules in red blood cells carry slightly more than 20% of the transported carbon dioxide. When carbon dioxide combines with hemoglobin, it forms a compound called carbaminohemoglobin.
3. As a bicarbonate ion. By far the most important means of transporting carbon dioxide is as bicarbonate ions dissolved in the plasma. About 70% of the carbon dioxide is transported this way. Carbon dioxide (CO2) produced by cells diffuses into the blood and into the red blood cells. In both the plasma and the red blood cells, it reacts with water (H2O) and forms carbonic acid (H2CO3). Carbonic acid quickly dissociates to form hydrogen ions (H+) and bicarbonate ions (HCO3-). The process of bicarbonate ion formation in the capillaries of the tissues is represented by the following formula:
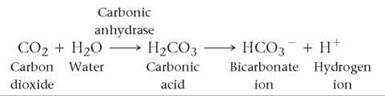
Although these reactions occur in the plasma as well as in red blood cells, they occur hundreds of times faster in red blood cells. The higher rate of reaction is caused by the enzyme carbonic anhydrase that is found within red blood cells but not in the plasma. The hydrogen ions produced by the reaction combine with hemoglobin. In this way, hemoglobin acts as a buffer, and the acidity of the blood changes only slightly as it passes through the tissues. The bicarbonate ions diffuse out of the red blood cells into the plasma and are transported to the lungs.
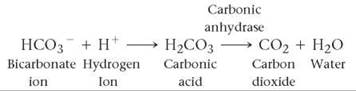
In the lungs, the process is reversed. When the blood reaches the capillaries of the lungs, carbon dioxide diffuses from the blood into the alveoli because the concentration (partial pressure) of carbon dioxide is comparatively low in the alveoli. Because the concentration of carbon dioxide in the blood is higher than in the alveoli, the chemical reactions we have just described reverse direction. The bicarbonate ions rejoin the hydrogen ions to form carbonic acid. In the presence of carbonic anhydrase within the red blood cells, carbonic acid is converted to carbon dioxide and water. The carbon dioxide then leaves the red blood cells, diffuses into the alveolar air, and is exhaled. The reactions in the lungs are summarized below.
Besides being the form in which carbon dioxide is transported by the blood, bicarbonate ions are an important part of the body's acid-base buffering system. They help neutralize acids in the blood. If the blood becomes too acidic, the excess hydrogen ions are removed by combining with bicarbonate ions to form carbonic acid. The carbonic acid then forms carbon dioxide and water, which are exhaled. (Bicarbonate ions and the acid-base balance of the blood are also discussed in Chapter 2.)
Stop and think
Carbon monoxide is a poisonous gas that binds to hemoglobin much more readily than does oxygen, and it binds in the same site as oxygen. Thus, when carbon monoxide is bound to hemoglobin, oxygen cannot bind. Why is carbon monoxide poisoning potentially fatal?
Respiratory Centers in the Brain
Breathing rate influences the amount of oxygen that can be delivered to cells and the amount of carbon dioxide that can be removed from the body. Neural and chemical controls adjust breathing rate to meet the body's needs.
Basic Breathing Pattern
As you sit there reading your text, your breathing is probably rather rhythmic, with about 12 to 15 breaths a minute. The basic rhythm is controlled by a breathing (respiratory) center located in the medulla of the brain (Figure 14.12). Within the breathing center are an inspiratory area and an expiratory area.
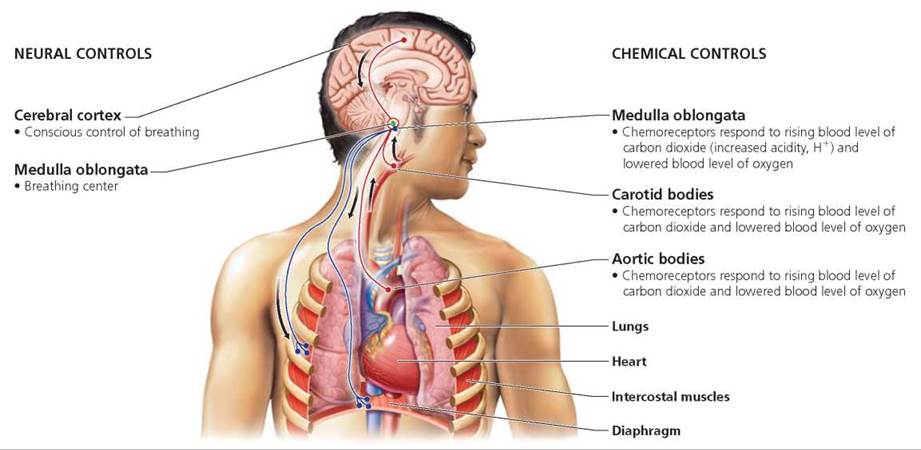
FIGURE 14.12. Neural and chemical controls of breathing
During quiet breathing, when you are calm and breathing normally, the inspiratory area shows rhythmic bouts of neural activity. While the inspiratory neurons are active, impulses that stimulate contraction are sent to the muscles involved in inhalation (the diaphragm and the intercostals). As we have seen, contraction of the diaphragm and the intercostals causes the size of the thoracic cavity to increase, thus moving air into the lungs. After about 2 seconds of inhalation, the activity of the neurons in the inspiratory center ceases for about 3 seconds. When inspiratory neurons cease activity, the diaphragm and intercostals relax, and passive exhalation occurs. During heavy breathing, such as might occur during exercise, the expiratory center causes contraction of other intercostal muscles and abdominal muscles, quickly pushing air out of the lungs.
Most of the time we breathe without giving it a thought. However, we can voluntarily alter our pattern of breathing through impulses originating in the cerebral cortex (the "conscious" part of the brain). We control breathing when we speak or sigh, and we can voluntarily pant like a dog. Holding our breath while swimming underwater is obviously a good idea. At certain other times, holding our breath can protect us from inhaling smoke or irritating gases.
During forced breathing, as might occur during strenuous exercise, stretch receptors in the walls of the bronchi and bronchioles throughout the lungs prevent the overinflation of the lungs. When a deep breath greatly expands the lungs and stretches these receptors, they send impulses over the vagus nerve that inhibit the breathing center, permitting exhalation. As the lungs deflate, the stretch receptors are no longer stimulated.
Chemoreceptors
The purpose of breathing is to control the blood levels of carbon dioxide and oxygen. We now consider how the levels of these gases control the breathing rate, which in turn influences the levels of the gases (Figure 14.13).
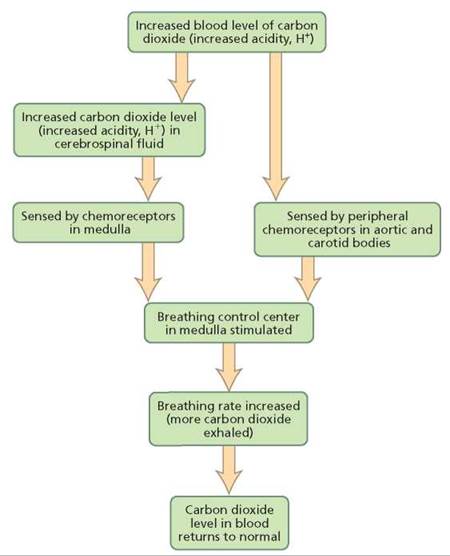
FIGURE 14.13. The role of carbon dioxide in controlling the breathing rate
Carbon dioxide. The most important chemical influencing breathing rate is carbon dioxide. The mechanism by which carbon dioxide regulates breathing depends on the hydrogen ions produced when carbon dioxide goes into solution and forms carbonic acid:

Three groups of chemoreceptors respond to the changing levels of hydrogen ions in the blood (Figure 14.12). Central chemoreceptors are located in a region of the brain called the medulla, near the breathing center. Peripheral chemoreceptors are located in the aortic bodies and the carotid bodies, small structures associated with the main blood vessel leaving the heart and going to the body as well as with the main blood vessels to the head. The chemoreceptors in the aortic bodies and carotid bodies also respond when the blood level of oxygen is low.
The chemoreceptors in the medulla are near its surface, where they are bathed in cerebrospinal fluid. Carbon dioxide diffuses from the blood into the cerebrospinal fluid, where it raises the hydrogen ion concentration by forming carbonic acid. When the rising hydrogen ion concentration stimulates the chemoreceptors in the medulla, breathing rate is increased and more carbon dioxide is exhaled, causing a decrease in the blood level of carbon dioxide.
Oxygen. Because oxygen, not carbon dioxide, is essential to survival, it may be somewhat surprising to learn that oxygen does not influence the breathing rate unless its blood level falls dangerously low. Only then do oxygen-sensitive chemoreceptors in the aortic bodies and carotid bodies send a message that the blood oxygen level is at a critical point, initiating a last-minute call to the medulla to increase the breathing rate and raise oxygen levels. If the oxygen level falls much more, the neurons in the inspiratory area die from a lack of oxygen and do not respond well to impulses from the chemoreceptors. As a result, the inspiratory area begins to send fewer impulses to the muscles of inspiration, the breathing rate decreases, and breathing may even cease completely.
Respiratory Disorders
Even in a restful day, you move more than 86,000 liters of air into and out of your lungs. The inhaled air may contain disease- causing organisms or noxious chemicals and particles. The respiratory system clears most of these materials out before they can cause harm. However, some of the disease-causing organisms, including viruses and bacteria, and other harmful substances remain and cause problems.
Common Cold
Any one of more than 200 viruses can cause a cold. Not surprisingly, some 30 million Americans have a cold at this moment. (The "common cold" is indeed common.) Because there are so many cold-causing viruses, you can, and usually do, get several colds a year, each from a different virus. Most people get their first cold before they are one year old.
Typically, a cold begins with a runny nose, possibly a sore throat, and sneezing. In the beginning, the nasal discharge is thin and watery, but it becomes thicker as it fills the nasal cavity. Almost any part of the respiratory system can be affected. Sneezing and a stuffy nose indicate that the infection is in the upper respiratory system. When the pharynx is affected, a sore throat results. The infection may spread to the bronchi, causing a cough, or to the larynx, making your voice hoarse.
As miserable as you feel with a cold, you can take comfort from knowing that your suffering will not last forever (see the Health Issue essay, Surviving a Common Cold). A cold is selflimiting, lasting only 1 to 2 weeks. Furthermore, colds are seldom fatal, except occasionally among the very young or very old or in those people already seriously ill with another malady.
Colds are spread when the causative virus is transmitted from an infected person. The viruses are plentiful in nasal secretions. However, transmission of the virus is not usually the result of direct inhalation of infected droplets from a cough or sneeze. It is more likely to be the result of handling an object that is contaminated with the virus. Cold viruses may remain capable of causing an infection on the skin or on an object for several hours, waiting for an unsuspecting person to touch them and contaminate his or her fingers. Subsequently, when the virus-laden fingers are touched to the mucous membranes of the nose, the transfer is completed. The best ways to prevent a cold are to wash your hands frequently and avoid being around people who have colds.
Flu
Flu is an abbreviation of influenza, another viral disease. The kinds of viruses that cause the flu are few compared to the number of different viruses that can cause a cold. In fact, the viruses that cause the flu in humans are all variants of three major types—A, B, and C (but there are hundreds of variants of these three basic types). Influenza of the A type is often more serious than B in that it is more frequently accompanied by severe complications, and it more frequently results in death. Influenza C causes a mild illness with cold symptoms.
Symptoms of the flu are similar to those of a cold, but they appear more suddenly and are more severe. (Though the onset of the flu may seem sudden, actually, by the time flu symptoms emerge, the disease has been incubating for several days.) A typical flu begins with chills and a high fever, about 103°F (39°C) in adults and perhaps higher in children. Many flu victims experience aches and pains in the muscles, especially in the back. Other common symptoms include a headache, sore throat, dry cough, weakness, pain and burning in the eyes, and sensitivity to light. When the flu hits, you usually feel sick enough to go to bed. The flu generally lasts for 7 to 10 days, but an additional week or more may pass before you are completely back on your feet.
The flu is often complicated by secondary infections, which set in when other disease-causing organisms take advantage of the body's weakened state. The most common complication is pneumonia, an inflammation of the lungs (described next). Possible secondary infections caused by bacteria include bronchitis, sinusitis, and ear infections.
One way to prevent the flu is by getting a flu shot—a vaccine made from the strains of viruses that scientists anticipate will cause the next outbreaks of the illness. Flu shots are only about 60% to 70% effective because the viruses they target mutate rapidly, causing new strains to appear. The new strains are not recognized by the immune system defenses that were programmed by the latest vaccine. Because each flu season brings new strains of flu viruses, the effectiveness of the vaccine lasts only as long as that season's most prevalent strains. As a result, new vaccines must be developed continually to protect us, and flu shots must be repeated each year.
Pneumonia
Pneumonia is an inflammation of the lungs that causes fluid to accumulate in the alveoli, thus reducing gas exchange. It also causes swelling and narrowing of the bronchioles, making breathing difficult. Pneumonia is usually caused by infection with bacteria or viruses, but fungi and protozoans can also cause it. Many cases of pneumonia develop after a common cold or influenza. Radiation, chemicals, and allergies can also bring it on.
Symptoms of pneumonia often begin suddenly. They include fever and chills, chest pain, cough, and shortness of breath. The severity of pneumonia varies from mild to life threatening. Treatment depends on the cause of the illness.
Strep Throat
Strep throat, a sore throat caused by Streptococcus bacteria, is a problem mainly in children 5 to 15 years old. The soreness is usually accompanied by swollen glands (lymph nodes) and a fever.
Although the pain of strep throat may be so mild that a doctor is never consulted, ignoring a strep infection can have serious consequences. If untreated, the Streptococcus bacteria can spread to other parts of the body and cause rheumatic fever or kidney problems. The main symptoms of rheumatic fever are swollen, painful joints and a characteristic rash. About 60% of rheumatic fever sufferers develop disease of the heart valves. Another possible consequence of a streptococcal infection is kidney disease (glomerulonephritis). The kidney damage is due to a reaction from the body's own protective mechanisms. The body produces antibodies that destroy the bacteria, but if these antibodies persist after the bacteria have been killed, they can cause the kidneys to become inflamed. The inflamed kidneys may be unable to filter the blood, and blood may leak into the urine.
Symptoms of strep throat include a sore throat and two of three of the following: fever of 101°F (38.33°C), white or yellow coating on tonsils, or swollen glands in the neck. Because many viruses can cause sore throats that look like strep infections, the only way to identify strep throat is to test for the causative organism. If Streptococcus bacteria are found, an antibiotic, usually penicillin, is prescribed to prevent rheumatic fever and kidney disease.
Tuberculosis
Tuberculosis (TB) is caused by a rod-shaped bacterium, Mycobacterium tuberculosis. It is spread when the cough of an infected person sends bacteria-laden droplets into the air and the bacteria are inhaled into the lungs of an uninfected person. Because the bacteria are inhaled, the lungs are usually the first sites attacked, but the bacteria can spread to any part of the body, especially to the brain, kidneys, or bone.
As a defense against the bacteria, the body forms fibrous connective tissue casings, called tubercles, that encapsulate the bacteria (hence, the name of the disease). Although the formation of tubercles slows the spread of the disease, it does not actually kill the bacteria. The immune system destroys at least some of the walled-off bacteria and may, in fact, kill them all. But pockets of bacteria may persist undetected for many years. Later, if the immune system becomes weakened, the disease may progress to the secondary stage as pockets of bacteria become reactivated and multiply. Furthermore, bacteria may escape from the tubercles and be carried by the bloodstream to other parts of the body. Whenever the patient becomes weak, ill, or poorly nourished, bacteria can become active and multiply, causing the disease to flare up.
The initial symptoms of tuberculosis, if they occur, are similar to those of the flu. In the secondary stage, the patient usually develops a fever, loses weight, and feels tired. If the infection is in the lungs, as is usual, it causes a dry cough that eventually produces pus-filled and blood-streaked phlegm. In this stage the bacteria multiply rapidly and destroy the cells of the affected organ. The second stage of TB can be fatal, especially if it is caused by a multi-drug-resistant strain of bacteria, and resistant strains are becoming increasingly common (discussed in Chapter 13a).
Health Issue
Surviving a Common Cold
The only thing more common than the cold is advice on how to treat it. Here we will examine the validity of some frequently suggested treatments for a cold.
1. Take large doses of vitamin C? Vitamin C will not prevent a cold unless you are malnourished or under extreme physical stress. Nonetheless, some people who take vitamin C may experience less severe or shorter colds than do people who do not take vitamin C.
2. Suck on a zinc lozenge? Some evidence exists that zinc slows viral replication, prevents cold viruses from adhering to nasal membranes, and boosts the immune system.
3. Take echinacea? Commonly known as the purple coneflower, echinacea has been used for centuries by cold sufferers. However, scientific studies examining whether the herbal medication is effective in preventing or treating the common cold have produced conflicting results.
4. Take an antibiotic? Antibiotics are not effective against viruses and cannot cure a cold. Unnecessary use of an antibiotic may cause side effects such as diarrhea and can lead to the development of bacterial resistance to the drug, as discussed in Chapter 13a.
5. Go to bed? Bed rest enables the body to muster its resources and fight secondary infections. Staying at home with a cold is also socially responsible, because it helps prevent the spread of the virus. Bed rest will not cure your cold or shorten its duration.
6. Have some chicken soup? Grandmothers have long prescribed chicken soup to treat a cold, and doctors finally agree that the advice has some merit. You should always consume plenty of fluids when you have a cold. They help loosen secretions in the respiratory tract and thus reduce congestion, allowing you to breathe more easily. Hot fluids, such as chicken soup, are more effective than cold ones for increasing the flow of nasal mucus.
Questions to Consider
• Do you think that it should be illegal to market cold remedies that have not been proven effective?
• A cold is not usually a serious illness. Should employees be prohibited from taking sick days for a cold?
What would you do?
DOTS (Directly Observed Therapy, short course) is the World Health Organization's recommended treatment for tuberculosis. DOTS, which mandates that someone witness the TB patient swallowing medication each day, is in place in most major cities in the United States. The treatment ranges from 6 months to 2 years (the latter, if a multi-drug-resistant strain is present). Patients' failure to complete TB treatment is what has led to the drug-resistant strains of the TB bacterium. Is DOTS a fair balance of protection of the public with personal rights? What do you think?
Bronchitis
Viruses, bacteria, or chemical irritation may cause the mucous membrane of the bronchi to become inflamed—a condition called bronchitis. The inflammation results in the production of excess mucus, which triggers a deep cough that produces greenish yellow phlegm.
There are two types of bronchitis: acute and chronic. Acute bronchitis, which often follows a cold, is usually caused by the cold virus itself, but it may be caused by bacteria that take advantage of the body's lowered resistance and invade the trachea and bronchi. An antibiotic will hasten recovery if the cause is bacterial.
When a cough that brings up phlegm is present for at least 3 months in each of 2 consecutive years, the condition is called chronic bronchitis, a more serious problem that is usually associated with cigarette smoking or air pollution. Some people with chronic bronchitis may lack an enzyme that normally protects the air passageways from such irritants. As the disease progresses, breathing becomes increasingly difficult, partly because the linings of the air tubules thicken, narrowing the passageway for air. Contraction of the muscles in bronchiole walls and excessive secretion of mucus further obstruct the air tubules.
Chronic bronchitis can have serious consequences. The degenerative changes in the lining of the air tubules make removal of mucus more difficult. As a result, the patient is more likely to develop lung infections such as pneumonia, which can be fatal, and degenerative changes—such as emphysema—in the lungs.
Emphysema
Emphysema is a common consequence of smoking, although this condition can have other causes as well. In emphysema, the walls of the alveoli break down and merge, thereby making the alveoli fewer and larger (Figure 14.14). This change has two major effects: a reduction in the surface area available for gas exchange and an increase in the volume of residual, or "dead," air in the lungs. Exhalation, you may recall, is a passive process that depends on the elasticity of lung tissue. In emphysema, the lungs lose that elasticity, and air becomes trapped inside them. As the dead air space increases, adequate ventilation requires more forceful inhalation. Forcing the air in causes more alveolar walls to rupture, further increasing the dead air space. Lung size gradually increases as the residual volume of air becomes greater, giving a person with emphysema a characteristic barrel chest, but gas exchange continues to become more difficult because surface area is reduced, despite the increase in lung size. To get an idea of what poor lung ventilation caused by increased dead air space feels like, take a deep breath, then exhale only slightly, and repeat this process several times. Notice how quickly you feel an oxygen shortage if you continue taking very shallow breaths that keep the lungs almost completely filled with air.
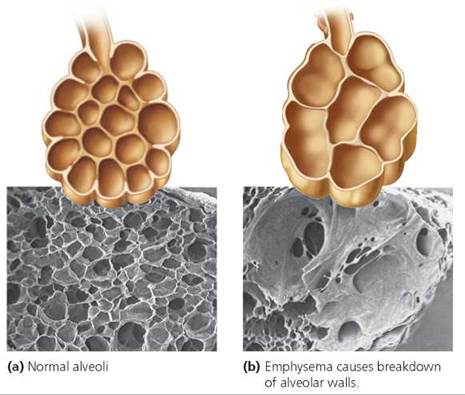
FIGURE 14.14. A comparison of (a) normal alveoli and (b) alveoli in an individual with emphysema. Notice that in emphysema, the alveolar walls rupture and there is a decrease in the surface area for gas exchange, an increase in the dead air space, and a thickening of the alveolar walls.
Shortness of breath, the main symptom of emphysema, is a result of both the decreased alveolar surface area and the increased dead air space. As the disease progresses, gas exchange becomes even more difficult because the alveolar walls thicken with fibrous connective tissue. The oxygen that does reach the alveoli has difficulty crossing the connective tissue to enter the blood. Thus, a person with emphysema constantly gasps for air.
Emphysema can be treated, but it cannot be cured. Cigarette smoking is the most common cause for emphysema, so the first step in treatment is usually to quit smoking. Medicines to widen the respiratory air tubules can be prescribed to make airflow to and from the lungs easier. In addition, supplemental oxygen may be administered to increase the amount of oxygen reaching the patient's body cells, which will relieve some of the symptoms of emphysema.
Lung Cancer
Between 85% and 90% of all cases of lung cancer are caused by smoking and are, therefore, preventable. Lung cancer usually has no symptoms until it is quite advanced. Therefore, it is not usually detected in time for a cure.
The progression to lung cancer begins with chronic inflammation of the lungs and is marked by changes in the cells of the airway linings. These cell changes are often caused by inhaled carcinogens, including those found in tobacco smoke (more chemicals found in tobacco smoke—and the respiratory problems they cause—are discussed in the Health Issue essay, Smoking and Lung Disease.)
In a nonsmoker, the lining of the air passageways has a basement membrane underlying basal cells and a single layer of ciliated columnar cells. In a smoker, one of the first signs of damage is an increase in the number of layers of basal cells. Next, the ciliated columnar cells die and disappear. The nuclei of the basal cells then begin to change as mutations accumulate, and the cells become disorganized. This is the beginning of cancer. Eventually, the uncontrolled cell division forms a tumor (Figure 14.15). When cancer cells break through the basement membrane, they can spread to other parts of the lung and to the rest of the body through a process called metastasis (see Chapter 21a).

FIGURE 14.15. Lung cancer. The tumor is the light-colored solid mass shown in the upper region of the lung.
Looking ahead
In this chapter, we considered how the respiratory system obtains the oxygen we need to survive and rids our bodies of carbon dioxide. In the next chapter, we will examine another function vital to life—digestion.
Health Issue
Smoking and Lung Disease
Smoking is the greatest single preventable cause of disease, disability, and death in our society. In fact, every cigarette pack and cigarette advertisement in the United States must bear a warning from the Surgeon General stating the dangers of tobacco smoke. Yet tobacco, which causes bodily harm when used exactly as intended, is legal to sell to anyone at least 18 years old.
Because the objective of smoking is to bring smoke into the lungs, we can expect some of its most damaging effects to be seen there. The damage to the respiratory system of smokers is gradual and progressive. It begins as the smoke hampers the actions of two of the lungs' cleansing mechanisms—cilia and macrophages. Even the first few puffs from a cigarette slow the movement of the cilia, making them less effective in sweeping debris from the air passageways. Smoking an entire cigarette prevents the cilia from moving for an hour or longer. With continued smoking, the nicotine and sulfur dioxide in the smoke paralyze the cilia, and the cyanide destroys the ciliated cells.
Cigarette smoke causes a smoker's lungs to be chronically inflamed. The inflammation summons macrophages, the wandering cells that engulf foreign debris, to the lungs for the purpose of cleaning the lung surfaces. But, just as smoke paralyzes the cilia, it also paralyzes the macrophages, further hampering the cleansing efforts. As the cilia and macrophages become less effective, greater quantities of tar and disease-causing organisms remain within the respiratory system. As a result, cigarette smokers spend more time sick in bed and lose more workdays each year than do nonsmokers.
At the same time that the cilia and macrophages are being slowed, the smoke stimulates the mucus-secreting cells in the linings of the respiratory passageways. Consequently, the smaller airways become plugged with mucus, making breathing more difficult. At this point, if not before, “smoker's cough” begins. Coughing is a protective reflex, and initially the smoker coughs simply because smoke irritates air passageways. However, as smoking continues and the cilia become less and less able to remove mucus and debris, the only way to remove the material from the passageways is to cough. The cough is generally worse in the morning, when the body attempts to clear away the mucus that accumulated overnight.
Gradually, the inflammation and congestion within the lungs, along with the constant irritation from smoke, lead to chronic bronchitis, a disease characterized by a persistent deep cough that brings up mucus. The air passageways become narrow due to the thickening of their linings caused by repeated infection, accumulation of mucus, and contraction of the smooth muscle in their walls. Airflow is restricted, resulting in breathlessness and wheezing.
Emphysema, in which the walls of alveoli are destroyed, is often the next stage in the progressive damage to the lungs. Airways and alveolar walls lose elasticity as tar causes body defense cells to secrete destructive enzymes. Consequently, the lung tissues can no longer absorb the increase in pressure that accompanies a cough, and the delicate alveolar walls break like soap bubbles. With more and more alveoli destroyed, the surface area for gas exchange is reduced, so less oxygen is delivered to the body. Besides all these negative effects on the respiratory system, smoking is the single major cause of lung cancer, and it causes other cancers as well. In fact, smoking is responsible for 30% of all cancer deaths.
The health benefits if you quit smoking are enormous. Much of the damage caused by smoke is reversible once you quit. For example, the risk of lung cancer drops, though it never falls as low as the level for people who have never smoked.
Questions to Consider
• Do you think that a ban on smoking in buildings violates smokers' rights?
• Many states are drastically increasing the tax on cigarettes. This action increases revenues and discourages an unhealthy behavior. Do you think that such a tax is unfair because it targets a particular segment of the population?
• What steps might you take to help a loved one quit smoking?
Highlighting the Concepts
Structures of the Respiratory System (pp. 267-273)
• The role of the respiratory system is to exchange oxygen and carbon dioxide between the air and the blood. The oxygen that we breathe is needed to maximize the number of energy-storing ATP molecules formed from food energy. Exhaling carbon dioxide, a waste product formed by the same reactions, helps regulate the acid-base balance of body fluids.
• The first structure that inhaled air usually passes through is the nose, which serves to clean, warm, and moisten the incoming air.
• The sinuses are air-filled spaces in the facial bones that also help warm and moisten the air.
• After leaving the nose, the inhaled air passes through the pharynx, or throat, and then the larynx, or voice box. Movements of the larynx during swallowing prevent food from entering the airways and lungs.
• The air passageways include the trachea, which branches to form bronchi, which branch various times in the lungs and eventually form progressively smaller branching tubules called bronchioles. The bronchioles terminate at the lungs' gas-exchange surfaces, the alveoli. Each alveolus is a thin-walled air sac encased in a capillary network.
Mechanism of Breathing (pp. 273-275)
• Pressure changes within the lungs, caused by changes in the size of the thoracic cavity, move air into and out of the lungs. Inspiration occurs when the size of the thoracic cavity increases, causing the pressure in the lungs to drop below atmospheric pressure. Expiration occurs when the size of the thoracic cavity decreases and pressure in the lungs rises above atmospheric pressure.
Transport of Gases between the Lungs and the Cells (pp. 275-277)
• Oxygen and carbon dioxide are exchanged between the alveolar air and the capillary blood by diffusion along their concentration (partial pressure) gradients. Oxygen diffuses from the alveoli into the blood, where it binds to hemoglobin within the red blood cells and is delivered to the body cells. A small amount of carbon dioxide is carried to the lungs dissolved in the blood plasma or bound to hemoglobin. Most, however, is transported to the lungs as bicarbonate ions.
Respiratory Centers in the Brain (pp. 277-278)
• The basic rhythm of breathing is controlled by the inspiratory area within the medulla of the brain. The neurons within this center undergo spontaneous bouts of activity. When they are active, messages are sent, causing contraction of the diaphragm and the muscles of the rib cage. As a result, the thoracic cavity increases in size and air is drawn into the lungs. When the inspiratory neurons are inactive, the diaphragm and rib cage muscles relax, and exhalation occurs passively. Also in the medulla is an expiratory area that causes forceful exhalation during heavy breathing.
• The most powerful stimulant to breathing is an increased number of hydrogen ions in the blood, formed from carbonic acid when carbon dioxide dissolves in plasma. Extremely low levels of oxygen also increase breathing rate.
Respiratory Disorders (pp. 278-282)
• The common cold and the flu are caused by viruses. Pneumonia is an inflammation of the lungs (caused by bacteria or viruses) that causes fluid to fill the alveoli and narrows bronchioles. Strep throat is a sore throat caused by Streptococcus bacteria. Acute bronchitis is caused by either bacteria or a virus. Chronic bronchitis is a persistent irritation of the bronchi. Emphysema is a breakdown of the alveolar walls and thus a reduction in the gas- exchange surfaces. Chronic bronchitis and emphysema are usually caused by smoking or air pollution. The primary cause of lung cancer is cigarette smoking.
Reviewing the Concepts
1. Why must we breathe oxygen? p. 267
2. Trace the path of air from the nose to the lungs. p. 268
3. How are most particles and disease-causing organisms removed from the inhaled air before it reaches the lungs? pp. 268-269
4. Explain why food does not usually enter the lower respiratory system when you swallow. p. 271
5. How is human speech produced? p. 271
6. What is the function of the cartilage rings in the trachea? What would happen to the trachea without these rings? p. 272
7. What is the bronchial tree? p. 272
8. How are the pressure changes in the thoracic cavity that are responsible for breathing created? pp. 273-274
9. Which is a larger volume of air: tidal volume or vital capacity? Explain. pp. 274-275
10. How is most oxygen transported to the body cells? p. 275
11. How is most carbon dioxide transported from the cells to the lungs? p. 276
12. What region of the brain causes the basic breathing rhythm? р. 277
13. Explain how blood carbon dioxide levels regulate the breathing rate. p. 278
14. What are the causes of the shortness of breath experienced by people with emphysema? pp. 280-281
15. Choose the correct statement.
a. During quiet breathing, expiration does not usually involve the contraction of muscles.
b. Expiration occurs when the diaphragm and the rib muscles contract.
с. Expiration occurs as the chest (thoracic) cavity enlarges.
d. The larynx acts like a suction pump to pull air into the lungs.
16. You should be able to hold your breath longer than normal after you hyperventilate (breathe rapidly for a while) because hyperventilating
a. decreases your blood oxygen levels.
b. decreases blood carbon dioxide levels.
c. increases blood oxygen levels.
d. increases blood carbon dioxide levels.
17. The structure specialized to produce the sound of your voice is the
a. trachea.
b. larynx.
c. bronchiole.
d. epiglottis.
18. In a healthy person, most of the particles that are inhaled into the respiratory system
a. are trapped in the mucus and moved by cilia to the pharynx (toward the digestive system).
b. pass through the alveoli into the circulatory system, where they are engulfed by white blood cells.
c. are caught on the vocal cords.
d. are trapped in the sinuses.
19. In emphysema
a. the number of alveoli is reduced.
b. cartilage rings in the trachea break down.
c. the diaphragm is paralyzed.
d. the epiglottis becomes less mobile
20. The _____ is the flap that covers the trachea to prevent food from entering during swallowing.
21. The enzyme in red blood cells that reversibly converts carbonic acid to bicarbonate ions and hydrogen ions is _____.
Applying the Concepts
1. Tatyana is a young woman with iron-deficiency anemia, so her blood does not carry enough oxygen. Would you expect this condition to affect her breathing rate or tidal volume? Why or why not?
2. Cigarette smoke destroys the cilia in the respiratory system. Explain why the loss of these cilia is a reason that cigarette smokers tend to lose more workdays because of illness than do nonsmokers.
3. Rosa has a 4-year-old son, Juan, who threatens to hold his breath until she gives him a candy bar. Should she be worried about Juan holding his breath? Why?
4. Vincent is having an asthma attack. During an asthma attack the bronchioles constrict (get narrower in diameter). Does Vincent have more difficulty inhaling or exhaling? Why?
Becoming Information Literate
Use at least three reliable sources (books, journals, or websites) to answer the following questions. List each source you considered, and explain why you chose the three sources you used.
1. The incidence of childhood asthma has increased steadily during the last few decades. What hypotheses have been proposed (at least three) to explain this increase in asthma? What evidence supports each hypothesis?
2. Studies have shown that secondhand cigarette smoke can pose health risks to nonsmokers nearby. Many state and local governments have laws preventing smoking in public places so that nonsmokers are not exposed to secondhand smoke. Present at least two arguments for and two against laws that ban smoking in public places. Then take a stand for or against such laws and defend your position.
3. Many of the first responders to the site of the collapse of the World Trade Center on September 11, 2001, have developed respiratory problems. Describe some of these respiratory problems. What is being done to treat these problems? Is there financial assistance for the affected people to help pay for their treatment?