Biology of Humans
17. Reproductive Systems
In the previous few chapters, we learned about the systems that are needed to maintain our bodies. In this chapter, we look at the structures of the reproductive systems and how they function. We also consider the sex hormones and the ways in which they regulate reproductive processes.
Gonads
In both males and females, the gonads—testes or ovaries—are the most important structures in the reproductive system. The gonads serve two important functions: (1) they produce the gametes, meaning the eggs and sperm—the cells that will fuse and develop into a new individual; and (2) they produce the sex hormones. The male gonads are the testes, and the gametes they produce are the sperm. The testes also produce the sex hormone testosterone. The ovaries are the female gonads. The gametes they produce are the eggs. The sex hormones they produce are estrogen and progesterone.
Male and Female Reproductive Roles
Males and females make an equal genetic contribution to the next generation by contributing one copy of each chromosome to their offspring. However, they have different "reproductive strategies" to help ensure that their DNA (packaged in their chromosomes) is passed along to a new generation. A male's strategy is to produce millions of sperm, deliver them to the female reproductive system, and hope that one sperm reaches an egg. In contrast, a female usually produces only one egg approximately once a month. If sperm delivery is appropriately timed with egg production, a sperm and egg may fuse in a process called fertilization.
If conditions are right, the cell created by fertilization, called a zygote, will develop into a new individual (see Chapter 18). A male's role in the reproductive process ends with delivery of sperm, but a female's role continues after egg production; she nourishes and protects the offspring until birth. The egg is packed with nutrients to provide for early development, and the woman's uterus serves as a nourishing, protective environment for the developing offspring.
· This beautiful baby girl seems comfortable in her new surroundings, although they can hardly be as sheltering and secure as her mother's uterus.
The development of eggs and sperm involves two types of cell division. The first is mitosis, a process in which a cell with 23 pairs of chromosomes replicates its chromosomes and divides into two identical cells, each with 23 pairs of chromosomes. The alterations in genetic content occur during the second type of cell division, called meiosis, which begins with a cell that has two copies of each of the 23 kinds of chromosome (called a diploid cell) and ends with up to four cells that each contain only one of each kind of chromosome (called haploid cells). Meiosis entails two rounds of cell division (called meiosis I and meiosis II). (The details of mitosis and meiosis are described in Chapter 19.)
Each cell in your body contains 23 pairs of chromosomes (for a total of 46 chromosomes). One member of each pair came from your father's sperm; the other member of each pair came from your mother's egg. Each of the 23 kinds of chromosome contains a different portion of the instructions for making and maintaining your body, and two of each kind are necessary for health and normal development. It is important, therefore, that only one member of each pair be present in a gamete.
Form and Function of the Male Reproductive System
The male reproductive system consists of the testes, a system of ducts through which the sperm travel; the penis; and various accessory glands. Accessory glands produce secretions that help protect and nourish the sperm as well as provide a transport medium that aids the delivery of sperm to the outside of the male's body. The structure of the male reproductive system is summarized in Table 17.1.
TABLE 17.1. Review of Male Reproductive System
Structure |
Function |
Testes |
Produce sperm and testosterone |
Epididymis |
Location of sperm storage and maturation |
Vas deferens |
Conducts sperm from epididymis to urethra |
Urethra |
Tube through which sperm or urine leaves the body |
Prostate gland |
Produces secretions that make sperm mobile and that counteract the acidity of the female reproductive tract |
Seminal vesicles |
Produce secretions that make up most of the volume of semen |
Bulbourethral glands |
Produce secretions just before ejaculation; may lubricate; may rinse urine from urethra |
Penis |
Delivers sperm to female reproductive tract |
Testes
The male reproductive system has two testes (singular, testis; Figure 17.1). Each is located externally to the body in a sac of skin called the scrotum. The temperature in the scrotum is several degrees cooler than within the abdominal cavity. The lower temperature is important in the production of healthy sperm.
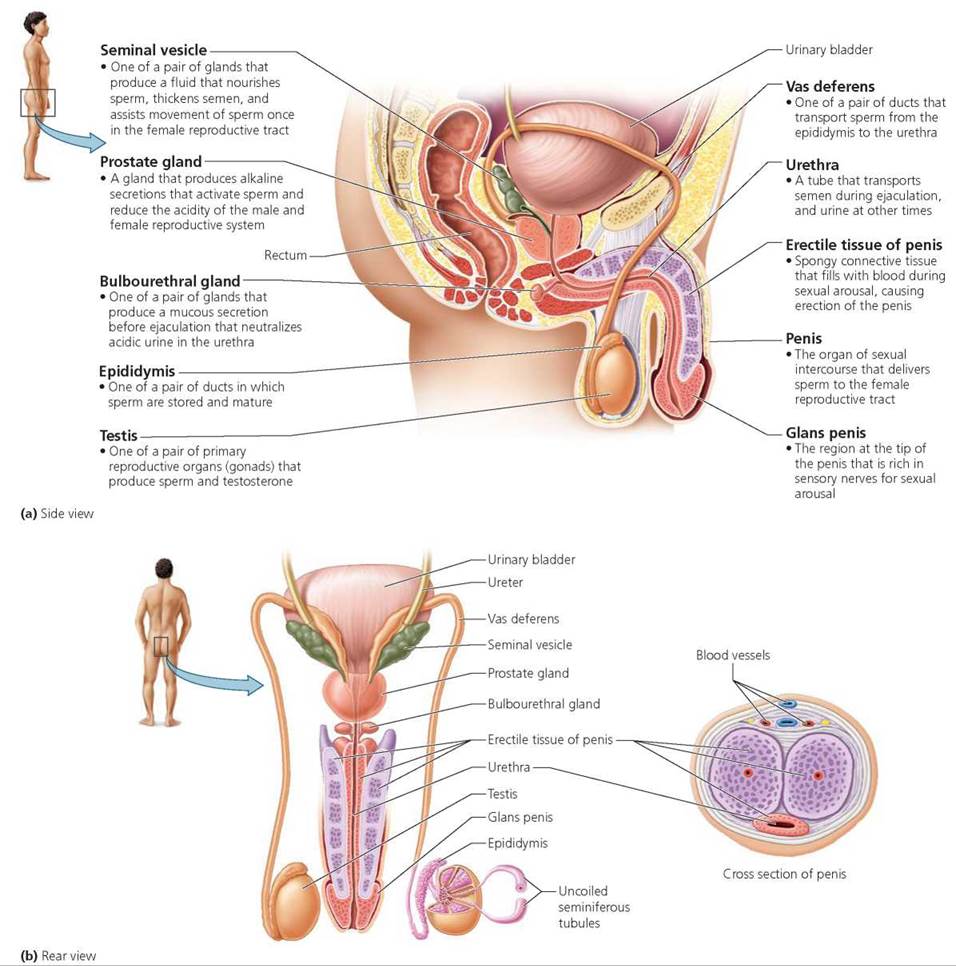
FIGURE 17.1. The male reproductive system
Reflexes in the scrotum help keep the temperature within the testes fairly stable. Cooling of the scrotum, such as might occur when a male jumps into frigid water, triggers contraction of a muscle that pulls the testes closer to the warmth of the body. In a hot shower, however, the muscle relaxes, and the testes hang low, away from the heat of the body. The skin of the scrotum is also amply supplied with sweat glands that help cool the testes.
Beginning at puberty (the transition to sexual maturity), which usually occurs during the teenage years, a healthy male produces more than 100 million sperm each day. The microscopic sites of sperm production are the seminiferous tubules (Figure 17.2). We will consider the development of sperm in more detail later in this chapter.
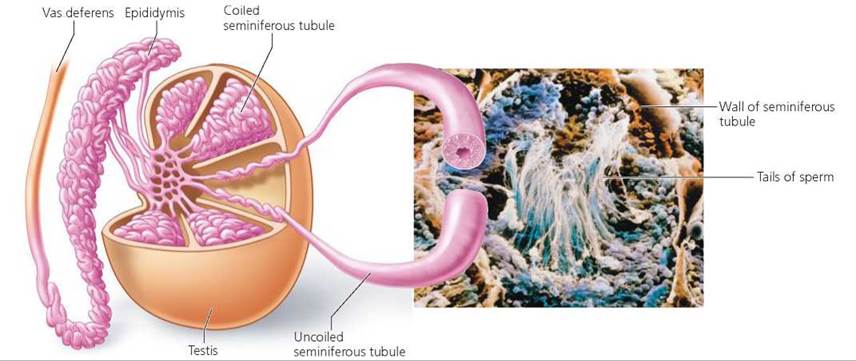
FIGURE 17.2. The internal structure of the testis and epididymis
The interstitial cells are located between the seminiferous tubules of the testis. They produce the steroid sex hormones, collectively called androgens. The most important androgen is testosterone, which is needed for sperm production and the maintenance of male reproductive structures.
Testicular cancer is the most common form of cancer among men between the ages of 15 and 35 years, although it affects only 1% of all men. Testicular cancer is more likely to occur in men whose testes did not descend into the scrotum or descended after 6 years of age. Because this cancer does not usually cause pain, it is important for every man to examine his testes each month to feel for a lump or a change in consistency. The cure rate for tumors caught in the early stages is nearly 100%.
Duct System
Sperm produced in the seminiferous tubules next enter a highly coiled tubule called the epididymis, where the sperm mature and are stored (see Figure 17.1). Sperm that enter the epididymis look mature, but they cannot yet function as mature sperm. During their stay in the epididymis, the sperm become capable of fertilizing an egg and of moving on their own, although they do not yet do so.
The tube that conducts sperm from the epididymis to the urethra is called the vas deferens. Some sperm may be stored in the part of the vas deferens closest to the epididymis. When a man reaches sexual climax, rhythmic waves of muscle contraction propel the sperm along the vas deferens.
The urethra conducts urine (from the urinary bladder) or sperm (from the vas deferens) out of the body through the penis, the male organ of sexual intercourse and urination. Sperm and urine do not pass through the urethra at the same time. A circular muscle contracts and pinches off the connection to the urinary bladder during sexual excitement.
Accessory Glands
Semen, the fluid released through the urethra at sexual climax, contains sperm and is composed of the secretions of the accessory glands: the prostate gland, the paired seminal vesicles, and paired bulbourethral glands. Very little of the volume of semen is made up of sperm.
About the size of a walnut, the prostate gland surrounds the upper portion of the urethra, just beneath the urinary bladder. Prostate secretions are slightly alkaline and serve both to activate the sperm, making them fully capable of moving, and to counteract the acidity of the female reproductive tract.
The prostate often begins enlarging when a man reaches middle age. The enlarged prostate may squeeze the urethra and restrict urine flow, making urination difficult. This benign enlargement of the prostate gland that accompanies aging is not related to prostate cancer.
Prostate cancer is an important cause of cancer deaths among men. Unlike testicular cancer, prostate cancer usually affects older men. There are two ways of detecting prostate cancer: a rectal exam and a blood test. Most physicians recommend that both tests be used in the diagnosis. During a rectal exam for prostate cancer, a physician inserts a gloved finger into the rectum and feels the prostate through the rectum's wall (see Figure 17.1). A cancerous prostate is firm or may contain a hard lump. The blood test for prostate cancer measures the amount of a protein called prostate-specific antigen (PSA). Because this protein is produced only by the prostate gland, the amount of PSA in the blood reflects the size of the prostate. As a tumor within the prostate grows, the blood level of PSA usually rises.
The secretions of the seminal vesicles contain citric acid, fructose, amino acids, and prostaglandins, which are chemicals secreted by one cell that alter the activity of nearby cells. Fructose is a sugar that provides energy for the sperm's long journey to the egg. Some of the amino acids thicken the semen. This thickening helps keep the sperm within the vagina and protects the sperm from contacting the acidic environment of the vagina. The prostaglandins serve to cut the viscosity of female cervical mucus (which could otherwise slow the movement of sperm) and to cause uterine contractions that assist the movement of sperm.
The bulbourethral glands release a clear, slippery liquid immediately before ejaculation. This fluid may serve to rinse the slightly acidic urine remnants from the urethra before the sperm pass through.
Penis
The penis is a cylindrical organ whose role in reproduction is to deliver the sperm to the female reproductive system. The tip of the penis is enlarged, forming a smooth, rounded head known as the glans penis, which has many sensory nerve endings and is important in sexual arousal. When a male is born, a cuff of skin called the foreskin covers the glans penis. The foreskin can be pulled back to expose the glans penis. The surgical removal of the foreskin is called circumcision.
The transfer of sperm to the female reproductive system during sexual intercourse usually requires the penis to be erect. An erection consists of increases in the length, width, and firmness of the penis, due to changes in the blood supply to the organ. Within the penis are three columns of spongy erectile tissue, which is a loose network of connective tissue with many empty spaces (see Figure 17.1). During sexual arousal, the arterioles that pipe blood into the spongy tissue dilate (widen), and the spongy tissue fills with blood, causing the penis to become larger. At the same time, the expanding spongy tissue squeezes shut the veins that drain the blood from the penis. As a result, the blood flows into the penis faster than it can leave, causing the spongy tissue to fill with blood and press against a connective tissue casing. This makes the penis firm, larger, and erect.
Erectile dysfunction (ED, also called impotence) is a male's inability to achieve or maintain an erection (and thus to have sexual intercourse). It is not unusual for a man to experience ED at some point in his life. This condition has some psychological causes, including worry, stress, a quarrel with the partner, and depression. However, it also has many physical causes. Nerve damage, which often accompanies chronic alcoholism and sometimes diabetes, can be responsible. Because an erection depends on adequate blood supply, fatty deposits in the arteries serving the penis (as in atherosclerosis) can also cause ED. Medications—especially certain drugs used to treat high blood pressure, antihistamines, antinausea and antiseizure drugs, antidepressants, sedatives, and tranquilizers—may cause the problem. Cigarette smoking, heavy alcohol consumption, or marijuana use can also cause ED.
The first step in treating ED is to eliminate the cause of the problem, if possible. Should impotency continue, drugs for erectile dysfunction—Viagra, Levitra, Cialis—may be prescribed. These drugs can help a man achieve and maintain an erection when he is sexually aroused. They work by prolonging the effect of nitric oxide, a chemical that is released when the man becomes sexually aroused and that causes the widening of the arterioles in the penis. As the arterioles widen, blood flow increases, and an erection results.
Stop and think
Why is it that Viagra, Levitra, or Cialis cannot cause an erection in a man who is not sexually aroused?
Sperm Development
The sequence of events within the seminiferous tubules that leads to the development of sperm is called spermatogenesis. This process reduces the number of chromosomes in the resulting gametes to one member of each pair and changes the sperm cells' shape and functioning to make the sperm efficient chromosome-delivery vehicles.
The process of spermatogenesis (Figure 17.3) begins in the outermost layer of each seminiferous tubule, where undifferentiated diploid cells called spermatogonia (singular, spermatogonium) develop. Each spermatogonium divides by mitosis to produce two new diploid spermatogonia. One of these spermatogonia pushes deeper into the wall of the tubule, where it will enlarge to form a primary spermatocyte, which is also a diploid cell. Primary spermatocytes undergo the two divisions of meiosis to form secondary spermatocytes (after meiosis I), which mature into spermatids (after meiosis II). Although the spermatids are haploid and have the correct set of chromosomes for joining with the egg during fertilization, numerous structural changes must still occur to create cells capable of swimming to the egg and fertilizing it. These changes convert spermatids to streamlined spermatozoa, or sperm. Spermatogonia mature into spermatozoa in about two months.
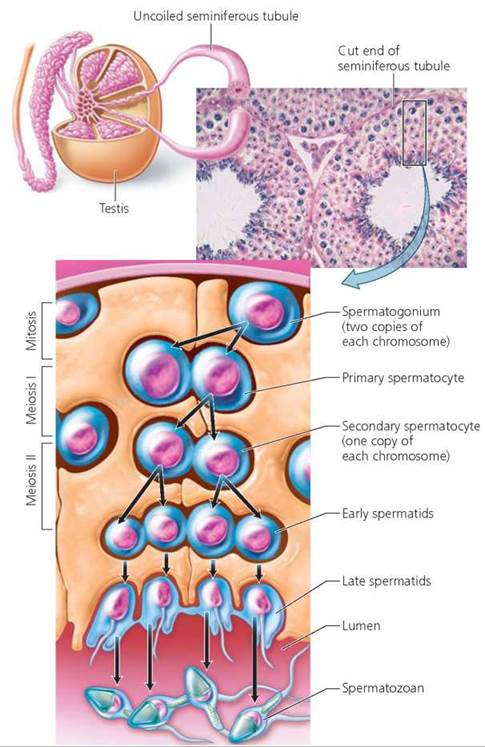
FIGURE 17.3. The stages of spermatogenesis in the wall of a seminiferous tubule. As the cells that will become sperm develop, they are pushed from the outer wall of the tubule to the lumen, or central canal.
The mature sperm cell has three distinct regions: the head, the midpiece, and the tail (Figure 17.4). The head of the sperm is a flattened oval that contains little else besides the 23 densely packed chromosomes (remember that the sperm is haploid). Positioned like a ski cap on the head of the sperm is the acrosome, a membranous sac containing enzymes. A few hours after the sperm have been deposited in the female reproductive system, the membranes of the acrosomes break down. The enzymes then spill out and digest through the layers of cells surrounding the egg, assisting fertilization. Within the midpiece, mitochondria are arranged in a spiral. Remember that the mitochondria are the powerhouses of the cell. They provide energy in the form of ATP to fuel the movements of the tail. The tail contains contractile filaments. The whiplike movements of the tail propel the sperm during its long journey through the female reproductive system.
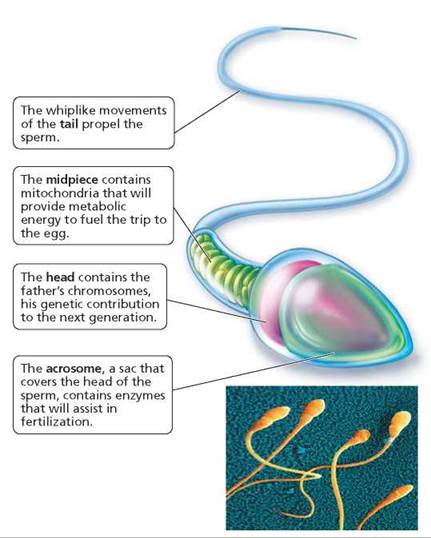
FIGURE 17.4. The structure of a mature sperm (spermatozoan)
Hormones
Testosterone, secreted by the interstitial cells of the testes, is important for sperm production as well as the development of male characteristics. At puberty, testosterone turns boys into men (literally). It is responsible for the growth spurt that occurs when a male reaches puberty, stimulating the growth of the long bones of the arms and legs. It also makes the male reproductive organs, including the testes and penis, larger. In addition, testosterone is responsible for the development and maintenance of the male secondary sex characteristics, which are features associated with "masculinity" but not directly related to reproductive functioning. For example, the growth of muscles and the skeleton tends to result in wide shoulders and narrow hips. Pubic hair develops, as does hair under the arms. A beard appears, perhaps accompanied by hair on the chest. Meanwhile, the voice box enlarges and the vocal cords thicken, causing a deepening of the male voice. And, importantly, testosterone is responsible for sex drive.
The level of testosterone in the body remains relatively steady because its production is regulated by a negative feedback loop (see Chapter 10) involving hormones from the hypothalamus, the anterior pituitary gland, and the testes. The hormones that regulate male reproductive processes are summarized in Figure 17.5 and Table 17.2. Testosterone levels rise when a region of the brain called the hypothalamus releases gonadotropin-releasing hormone (GnRH). This hormone stimulates the anterior pituitary gland, a pea-sized endocrine gland on the underside of the brain, to secrete luteinizing hormone (LH). In turn, LH stimulates the production of testosterone by the interstitial cells of the testis. (For this reason, LH is sometimes called interstitial cell-stimulating hormone, or ICSH.) The rising testosterone level inhibits the release of GnRH from the hypothalamus. As a result, the amount of LH produced by the anterior pituitary drops. This decrease in the LH level then lowers the amount of testosterone secretion, removing the inhibition on the hypothalamus. These interactions keep testosterone levels constant.
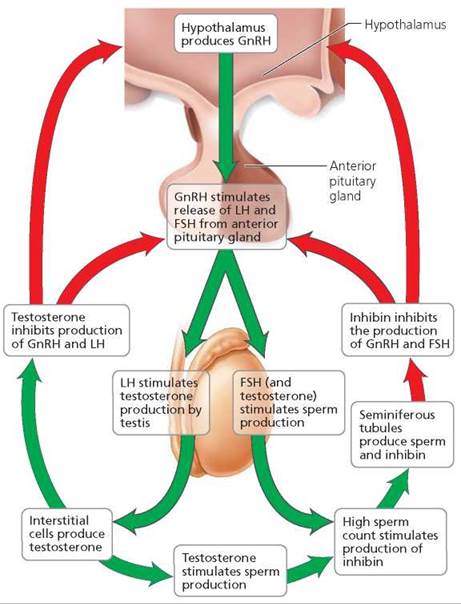
FIGURE 17.5. The feedback relationships among the hypothalamus, anterior pituitary, and testes control the production of both sperm and testosterone.
TABLE 17.2. Hormones Important in Regulating Male Reproductive Processes
Hormone |
Source |
Effects |
Testosterone |
Interstitial cells in testes |
Sperm production; development and maintenance of male reproductive structures, male secondary sex characteristics; sex drive |
Gonadotropinreleasing hormone (GnRH) |
Hypothalamus (in brain) |
Stimulates the anterior pituitary gland to release LH |
Luteinizing hormone (LH) |
Anterior pituitary gland (in brain) |
Stimulates interstitial cells of testis to produce testosterone |
Follicle-stimulating hormone (FSH) |
Anterior pituitary gland (in brain) |
Enhances sperm formation |
Inhibin |
Seminiferous tubules in testes |
Inhibits FSH secretion by anterior pituitary gland, causing a decrease in sperm production and testosterone production |
Sperm production is regulated by another negative feedback loop. Besides secreting LH, the anterior pituitary gland produces follicle-stimulating hormone (FSH). Follicle-stimulating hormone stimulates sperm production by making the cells that will become sperm more sensitive to the stimulatory effects of testosterone. FSH works by causing certain cells within the seminiferous tubules to secrete a protein that binds and concentrates testosterone.
When sperm numbers are high, the seminiferous tubules produce a hormone called inhibin in addition to sperm. Inhibin is named for its ability to inhibit, or lessen, the production of FSH from the anterior pituitary. It also may inhibit the hypothalamic secretion of GnRH. Thus, rising levels of inhibin cause a decline in testosterone level and sperm production. As the sperm count falls, so does the level of inhibin. Released from inhibition, the anterior pituitary then increases production of FSH, and the hypothalamus produces GnRH, which increases sperm production again.
Stop and think
Some male athletes take anabolic steroids to build muscles. A side effect of steroid abuse is a reduction in testis size. Considering that the anabolic steroids mimic the effect of testosterone, how can the shrinking testis size be explained?
Form and Function of the Female Reproductive System
The female reproductive system consists of the ovaries, the oviducts, the uterus, the vagina, and the external genitalia. Its structure is shown in Figure 17.6, and its functions are summarized in Table 17.3.
TABLE 17.3. Review of Female Reproductive System
Structure |
Function |
Ovary |
Produces eggs and the hormones estrogen and progesterone |
Oviducts |
Transport ovulated oocyte (or embryo if fertilization occurred) to the uterus; the usual site of fertilization |
Uterus |
Receives and nourishes embryo |
Vagina |
Receives penis during intercourse; serves as birth canal |
Clitoris |
Contributes to sexual arousal |
Breasts |
Produce milk |
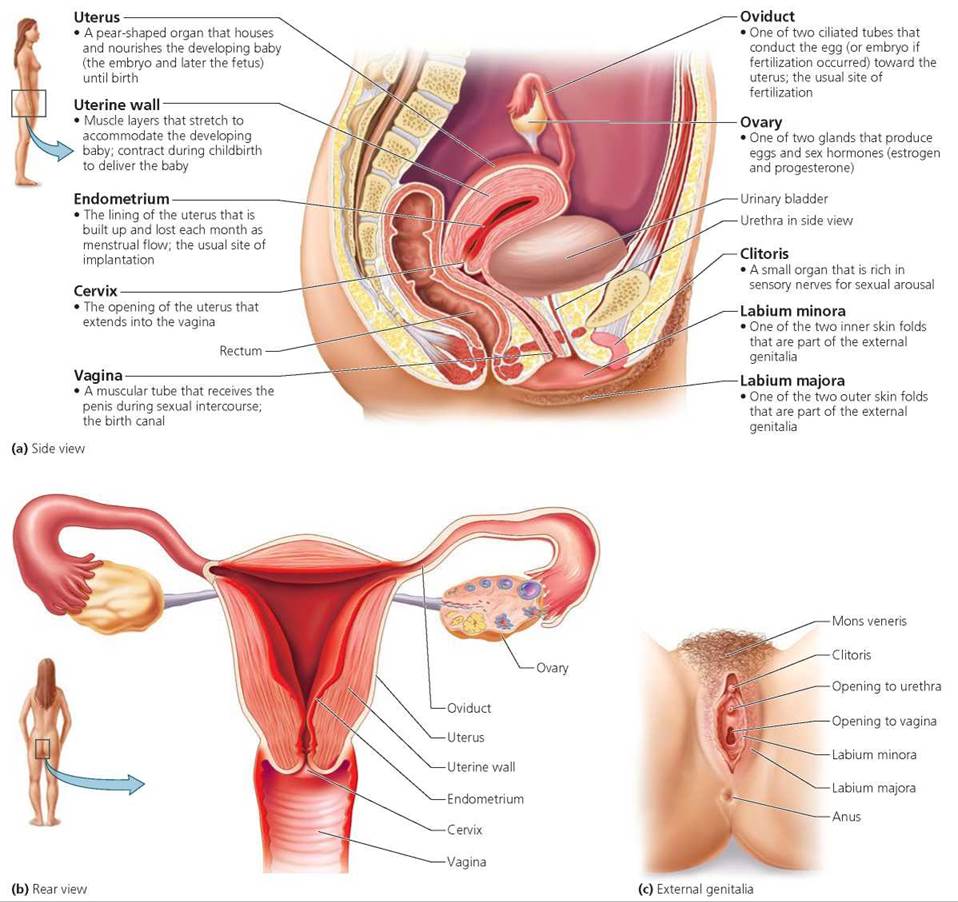
FIGURE 17.6. The female reproductive system
Ovaries
Each ovary is about twice the size of an almond. There is an ovary on each side of the uterus. The ovaries have two important functions: (1) to produce eggs in a process called oogenesis and (2) to produce the hormones estrogen and progesterone. These two functions are intimately related and occur in cycles, as we will see.
Oviducts
Two oviducts, also known as fallopian tubes or uterine tubes, extend from the uterus to the ovaries—although they do not attach to the ovaries. They transport the immature egg, called an oocyte, from the ovary to the uterus. The end of each oviduct nearest the ovary is open and funnel shaped. Its many ciliated, fingerlike projections drape over the ovary but are rarely in direct contact with it. Shortly before the egg is released from the ovary, the projections from the tubes begin to wave. The currents they create, and those caused by the cilia lining the tubes, help draw the oocyte into the oviduct. If fertilization occurs, it usually takes place in the oviduct, near the ovary. The resulting zygote begins its development into an embryo in the oviduct. The beating cilia and the rhythmic, muscular contractions of the oviduct sweep the egg or the early embryo along the oviduct toward the uterus
Uterus
The uterus is a hollow, muscular organ that before pregnancy is about the size and shape of an inverted pear. The uterus receives and nourishes the developing baby (first called an embryo, but after 8 weeks called a fetus). During pregnancy, as the fetus grows, the uterus expands to about 60 times its original size. After childbirth, the uterus never quite returns to its prepregnancy size.
The wall of the uterus has two main layers: a muscular layer and a lining called the endometrium (endo-, within; metr-, uterus; -ium, region). The smooth muscle of the uterine wall contracts rhythmically in waves during childbirth and forces the infant out. The thickness of the endometrium varies over a cycle of approximately 1 month (this cycle is discussed later in this chapter). If an embryo forms, it implants (embeds) in the endometrium, which provides nourishment during early pregnancy. If an embryo does not form, the endometrium completes its cycle by being lost as menstrual flow.
If an embryo implants in an area other than the uterus, the condition is described as an ectopic pregnancy (ect-, outside). The most common type of ectopic pregnancy is a tubal pregnancy, in which the embryo implants in an oviduct. A tubal pregnancy cannot be carried to term. It must be surgically terminated because it endangers the mother's life. If the embryo is permitted to continue growing, it will eventually rupture the oviduct, and the rupture can cause the mother to bleed to death internally.
The narrow neck of the uterus, called the cervix, projects into the vagina, a muscular tube that opens to the outside of the body. The vagina receives the penis during sexual intercourse. Sperm that are deposited in the vagina can enter the uterus through an opening in the cervix and then swim to the oviduct to meet the egg. The vagina is also the birth canal. The infant is pushed through the cervix and then the vagina on the way to greet the world.
External Genitalia
The female reproductive structures that lie outside the vagina are collectively known as the external genitalia or the vulva. Two hair-covered folds of skin surround the vaginal opening. The labia majora ("big lips") enclose two thinner skin folds, the labia minora ("little lips"). The anterior portions of the labia minora form a hood over the clitoris. Like the penis, the clitoris has many nerve endings sensitive to touch. During tactile stimulation, the erectile tissue in the clitoris becomes swollen with blood and contributes to a woman's sexual arousal.
Breasts
The breasts, or mammary glands, are present in both sexes, but they produce milk to nourish a newborn only in females. Inside the female breast are 15 to 25 groups of milk-secreting glands. A milk duct drains each group through the nipple. Interspersed around the glands and ducts is fibrous connective tissue that supports the breast. Most of the breast consists of fatty tissue (Figure 17.7). Breast cancer is the second leading cause of cancer deaths among women (see the Health Issue essay, Breast Cancer).
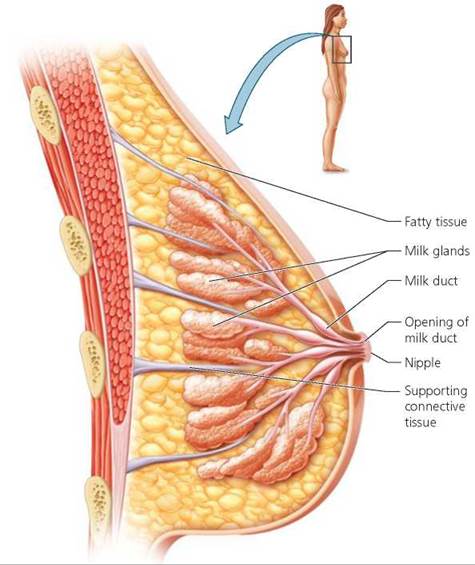
FIGURE 17.7. Breast structure
Ovarian Cycle
The changes in the ovary that produce the egg occur in a cycle about 1 month long called the ovarian cycle. Although the ovaries do not produce mature eggs until a female reaches puberty, the preparations for egg production begin before she is born. Recall that the egg is a haploid cell formed by meiosis, the type of cell division that forms gametes. During fetal development, oogonia, which are diploid cells in the ovaries, enlarge and begin to store nutrients. Some begin meiosis by making a copy of their chromosomes (but the copies of each chromosome remain attached to one another). The cells that prepare for meiosis are called primary oocytes. (They are immature eggs.) A single layer of flattened cells, called follicle cells, surrounds each primary oocyte. The entire structure is called a primary follicle.
Long before her birth, all of a woman's potential eggs have formed. In fact, she may have formed as many as 2 million primary follicles. Only about 700,000 remain when she is born, and the number continues to decrease after birth. The eggs remain in this immature state until she reaches puberty, usually at 10 to 14 years of age. By the time of puberty, a female's lifetime supply of potential eggs has dwindled to between 200,000 and 400,000. Only 400 to 500 of these eggs will ever mature.
Beginning at puberty, some primary follicles, usually one each month, resume their development (Figure 17.8). The follicle's outer cells begin dividing, forming layers of cells and secreting a fluid that contains estrogen. The ovarian cycle that converts a primary follicle into an egg each month consists of the following steps:
• Follicle maturation. The follicle cells continue dividing, and fluid begins to accumulate between them. As the fluid accumulates, the wall of follicle cells splits into two layers. The inner layer of follicle cells directly surrounds the primary oocyte. The outer layer forms a balloonlike sphere enclosing the fluid and the oocyte. This structure grows rapidly.
• Formation of a mature follicle. Within about 10 to 14 days after its development began, the follicle assumes its mature form, called a secondary or Graafian follicle. The primary oocyte then completes the first meiotic division, which it prepared for years earlier. When the primary oocyte divides, it forms two cells of unequal size: a large cell that contains most of the cytoplasm and nutrients, called a secondary oocyte, and a tiny cell, called the first polar body. The polar body is essentially a garbage bag for one set of chromosomes. It has very few cellular constituents and plays no further role in reproduction. The secondary oocyte is a much larger cell packed with nutrients that will nourish the embryo until it reaches the uterus.
• Ovulation. About 12 hours after the secondary oocyte has formed, the mature follicle pops, like a blister, releasing the oocyte mass, which is about the size of the head of a pin. The release of the oocyte from the ovary is called ovulation. If a sperm penetrates the secondary oocyte, meiosis advances to completion: The replicate chromosomes are separated. This time, too, the cytoplasm divides unequally. One of the resulting sets of chromosomes goes into a small cell, called the second polar body, and the other set goes into a large cell, the mature ovum, or egg. If fertilization does not occur, the egg does not complete meiosis.
• Formation of the corpus luteum. The cells that made up the outer sphere of the mature Graafian follicle remain in the ovary, and luteinizing hormone (LH) transforms them into an endocrine structure called the corpus luteum (meaning "yellow body"). The corpus luteum secretes both estrogen and progesterone. Unless pregnancy occurs, the corpus luteum degenerates. If pregnancy occurs, the corpus luteum will be maintained by a hormone from the embryo called human chorionic gonadotropin, as we will see later in this chapter.
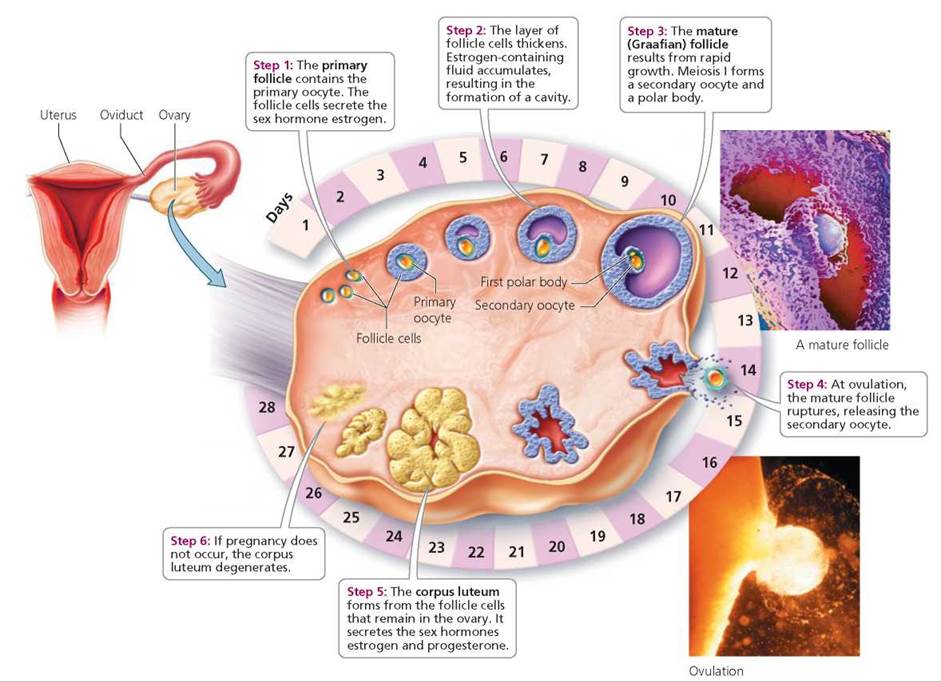
FIGURE 17.8. The ovarian cycle. A follicle does not move around the ovary during its development, as depicted here. The steps indicate the sequence of events that occur in a single place in the ovary during the approximately 28-day cycle.
Coordination of the Ovarian and Uterine Cycles
Because of the events we have been describing, a woman's fertility is cyclic. At approximately monthly intervals, an egg matures and is released from an ovary. Simultaneously, the uterus is readied to receive and nurture the young embryo. These two processes must be coordinated. If fertilization does not occur, the uterine provisions are discarded as menstrual flow. The ovaries and uterus will prepare for fertilization again during the next cycle. The events in the ovary, known as the ovarian cycle, must be closely coordinated with those in the uterus, known as the uterine cycle (or the menstrual cycle). The length of the uterine cycle may vary from cycle to cycle and from woman to woman. The timing of events within a uterine cycle will vary with the cycle's length. We will describe the events as they might occur in a 28-day cycle.
A female's fertility is governed by hormones (Table 17.4). Events in both the uterus and the ovary are coordinated by interactions between hormones from the anterior pituitary gland and from the ovary. The anterior pituitary gland produces follicle-stimulating hormone (FSH) and luteinizing hormone (LH). As in the male, the release of these hormones is regulated by a hormone from the hypothalamus called GnRH. In the female, FSH and LH cause the ovary to release its hormones, estrogen and progesterone. Progesterone and estrogen (except at a very high level) exert negative feedback on the anterior pituitary, which causes the levels of FSH and LH to decline. As a result, the levels of estrogen and progesterone decline, reducing the inhibition on the anterior pituitary gland—and so, the hormones cycle.
TABLE 17.4. Hormones Involved in Regulating Female Reproductive Processes
Hormone |
Source |
Effects |
Estrogen |
Ovaries (follicle cells and corpus luteum) |
Maturation of the egg; development and maintenance of female reproductive structures, secondary sex characteristics; thickens endometrium of uterus in preparation for implantation of embryo; cell division in breast tissue |
Progesterone |
Ovaries (corpus luteum) |
Further prepares uterus for implantation of embryo; maintains endometrium |
Follicle-stimulating hormone (FSH) |
Anterior pituitary gland (in brain) |
Stimulates development of a follicle in the ovary |
Luteinizing hormone (LH) |
Anterior pituitary gland (in brain) |
Triggers ovulation; causes formation of the corpus luteum |
Stop and think
Fertility clinics may administer FSH to women who are having difficulty getting pregnant. Why would FSH increase the likelihood of pregnancy? Why would women treated with FSH be more likely to have multiple births?
Menstruation. Traditionally, the first day of menstrual flow is considered day 1 of the uterine cycle because it is the most easily recognized event in the cycle (Figure 17.9). The bleeding usually lasts an average of 5 days. During menstruation, the ovarian hormones, estrogen and progesterone, are at their lowest levels, allowing the anterior pituitary gland to produce its hormones, especially FSH. In turn, FSH causes a new egg follicle in the ovary to develop and produce estrogen. (Hence its name, follicle-stimulating hormone.) Thus, even as the uterus loses the endometrial lining it prepared during the previous cycle in which no egg was fertilized, the egg that will be released in the next cycle is developing.
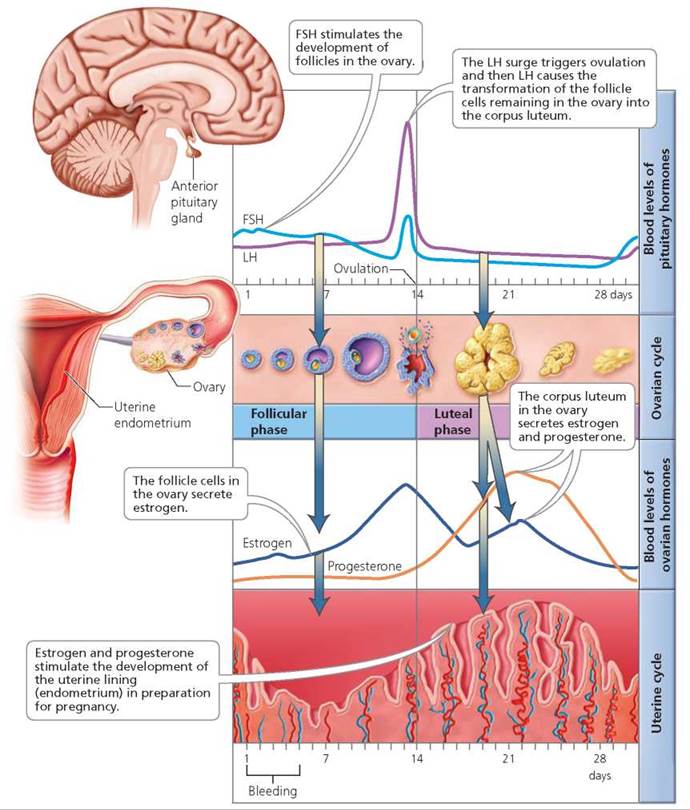
FIGURE 17.9. The ovarian and uterine cycles are coordinated by the interplay of hormones from the anterior pituitary gland and the ovary. The timing of events shown is for a 28-day cycle.
Couples who are trying to conceive a child can purchase kits to help them predict when ovulation will occur, so that intercourse can be timed appropriately to increase the chance of becoming pregnant. Which hormone would be the best predictor of ovulation? Why?
LH, because the surge in LH levels triggers ovulation.
Endometrium thickens. As the egg follicle develops, it produces an increasing amount of estrogen. Estrogen causes the cells in the endometrial lining of the uterus to divide. These cells store nutrients to nourish a future embryo during its early stages of development. In addition, estrogen inhibits the release of FSH through a negative feedback cycle (see Chapter 10). When the egg and follicle are nearly mature, the estrogen level rises rapidly and causes a sudden and spectacular release of LH (and FSH) from the anterior pituitary gland.1
Ovulation and formation of corpus luteum (in ovary). The LH surge causes several important events. It causes the egg to undergo its first meiotic division. Next, LH triggers ovulation, and the egg bursts out of the ovary to begin its journey along the oviduct. Continued secretion of LH then transforms the remaining follicle cells into the corpus luteum. The corpus luteum continues the estrogen secretion begun by the follicle cells and, importantly, also secretes progesterone.
Endometrium further prepared for implantation. Together, estrogen and progesterone make the endometrial lining of the uterus a hospitable place for the embryo. The blood supply to the endometrium increases. Uterine glands develop and then secrete a mucous material that can nourish the young embryo when it arrives in the uterus.
The rising estrogen and progesterone levels inhibit pituitary secretion of FSH and LH. As FSH levels decline, the development of new follicles is inhibited.
Corpus luteum degenerates. If fertilization does not occur, the corpus luteum will degenerate within about 2 weeks (14 days plus or minus 2 days, regardless of the length of the menstrual cycle). The degeneration of the corpus luteum results in falling levels of estrogen and progesterone.
Menstruation begins again. Progesterone is essential to the maintenance of the endometrium. As progesterone levels drop because of the degeneration of the corpus luteum, the blood vessels nourishing the endometrial cells collapse. The cells of the endometrium then die and are sloughed off, along with mucus and blood, as menstrual flow. No longer inhibited by estrogen and progesterone, FSH and LH levels begin to climb. Thus, the cycle begins again (Table 17.5).
TABLE 17.5. Ovarian and Uterine Cycles
Ovarian Cycle |
|
Uterine Cycle |
|
Approximate Timing in 28-Day Cycle |
Events |
Approximate Timing in 28-Day Cycle |
Events |
Days 1-13 |
Follicle develops, caused by FSH Follicle cells produce estrogen |
Day 1 |
Onset of menstrual flow (breakdown of endometrium) |
Day 14 |
Ovulation is triggered by LH surge |
Day 6 |
Endometrium begins to get thicker |
Days 15-21 |
Corpus luteum forms and secretes estrogen and progesterone |
Days 15-23 |
Endometrium is further prepared for implantation of the embryo by estrogen and progesterone |
Days 22-28 |
Corpus luteum degenerates, causing estrogen and progesterone level to decline |
Days 24-28 |
Endometrium begins to degenerate owing to declining maintenance by progesterone |
If the egg is fertilized, a hormone from the embryo, called human chorionic gonadotropin (HCG), maintains the corpus luteum. If implantation occurs, HCG will prevent the degeneration of the corpus luteum, keeping estrogen and progesterone levels high enough to prevent endometrial shedding. HCG is detectable in the mother's blood within 7 to 9 days after implantation and in her urine less than 2 weeks after implantation, which is usually before her first missed period. Between the second and third month of development, the placenta has developed sufficiently to take over the production of estrogen and progesterone during the rest of the pregnancy. The corpus luteum then degenerates.
What would you do?
It is clear that we have polluted our environment with chemicals that mimic the effects of estrogen. Sex hormones choreograph so many biological activities—development, anatomy, physiology, and behavior—that environmental estrogens can play havoc with human reproduction in myriad ways. It is also clear that this pollution is already affecting various animal species. What is not clear is how great a threat these chemicals are to humans. The International Union of Pure and Applied Chemistry (IUPAC) recommends research and monitoring of environmental estrogens. Implementing these recommendations would be costly. As a taxpayer, are you willing to pay for these precautions?
Menopause
A woman's fertility usually peaks when she is in her twenties and then gradually declines. By the time she reaches 45 to 55 years of age, few of the potential eggs prepared before birth remain in the ovaries. Those that do remain become increasingly less responsive to FSH and LH, the hormones that cause egg development and ovulation. The ovaries, therefore, gradually stop producing eggs, and the levels of estrogen and progesterone fall. During this time, menstrual cycles become increasingly irregular. Eventually ovulation and menstruation stop completely, at a stage in a woman's life called menopause.
The drop in estrogen levels has some physiological effects that can range in severity from annoying to life threatening. At one end of the scale is the loss of a layer of fat that was formerly promoted by estrogen. This loss results in a reduction in breast size and the appearance of wrinkles. Estrogen also plays an important role in regulating a woman's body thermostat. So, as estrogen levels fall, many women experience hot flashes—waves of warmth spreading upward from the trunk to the face. In addition, the absence of estrogen can cause vaginal dryness that can make sexual intercourse painful. Furthermore, without estrogen, the male hormones produced by the adrenal gland predominate and can cause facial hair to grow.
More serious problems associated with the estrogen deficit that accompanies menopause include an increased risk of diseases of the heart and blood vessels. Estrogen offers some protection against atherosclerosis, a condition in which fatty deposits clog the arteries. Thus, after menopause, this protective effect on the heart is lost. Another serious problem stems from the role estrogen plays in the body's ability to absorb calcium from the digestive system and to deposit it in bone. Without calcium, bone becomes weak and porous—a condition known as osteoporosis (discussed in Chapter 5).
Until 2002, doctors routinely prescribed hormone replacement therapy (HRT), which contains estrogen and progesterone, for postmenopausal women. HRT reduces hot flashes and vaginal dryness and protects against osteoporosis. The routine recommendation ended with a study showing that HRT elevates a woman's risk of stroke. Today, doctors help postmenopausal women weigh the benefits and risks of HRT, so a woman can make a wise decision on whether to use HRT.
Health Issue
Breast Cancer
Breast cancer usually begins with abnormal growth of the cells lining the milk ducts of the breast, but it sometimes begins in the milk glands themselves. Some types of breast cancer aggressively invade surrounding tissues. Typically, cancerous cells begin to spread when the tumor is about 20 mm (about 3/4 in.) in diameter. At this point, they break through the membranes of the ducts or glands where they initially formed and move into the connective tissue of the breast. They may then move into the lymphatic vessels or blood vessels permeating the breast or into both; the vessels may transport the cells throughout the body.
Detecting Breast Cancer
Early detection is a woman's best defense against breast cancer. A monthly breast selfexam (BSE) is helpful in detecting a lump early (Figure 17.A). If a woman begins doing regular breast self-exams in early adulthood, she becomes familiar with the consistency of her breast tissue. With this experience, it is easier to notice changes that might be signs of breast cancer. Mammograms, which are x-rays of breast tissue, can also help detect early breast cancer because they can reveal a tumor too small to be felt as a lump. A tumor large enough to be felt contains a billion or more cells—a few of which may already have spread from the tumor to other tissues of the body. After cancer cells spread, the woman's chance of survival decreases dramatically. An added benefit of mammograms is that they can detect tumors that are small enough to be removed by a type of surgery called lumpectomy, which removes the lump but spares the breast. At later stages of breast cancer, the entire breast may have to be removed in a type of surgery called mastectomy.
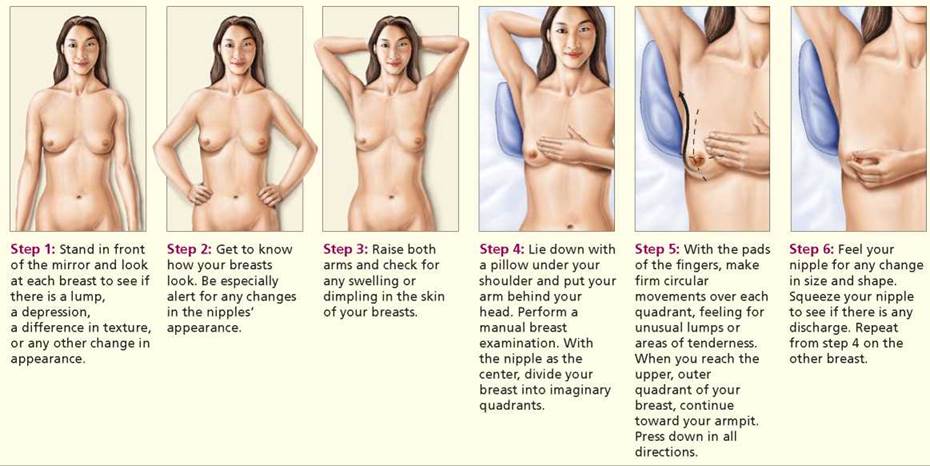
FIGURE 17.A. A monthly breast self-exam can help a woman find lumps in her breast before they have spread to surrounding tissue. It also makes make a woman familiar with the consistency of her breast tissue and therefore able to detect changes in consistency that might indicate cancer.
Risk Factors
Many of the factors that increase a woman's risk of breast cancer cannot be altered. One of these is the genes she inherited from her parents. At least two known genes increase a woman's risk of breast cancer. Although only 5% to 10% of all breast cancers are related to these genes, the unlucky women who inherit either of them have an 85% chance of developing breast cancer at some point in life.
Exposure to estrogen is a common thread running through the tapestry of risk factors associated with breast cancer. During each menstrual cycle, estrogen stimulates breast cells to begin dividing in preparation for milk production, in case the egg is fertilized. Excessive estrogen exposure, therefore, may be a factor that pushes cell division to a rate characteristic of cancer.
One factor that influences estrogen levels is the number of times a woman ovulates during her lifetime, because estrogen is produced by both the maturing ovarian follicle and the corpus luteum. The number of times a woman ovulates is, in turn, affected by factors such as the following:
1. Age when menstruation begins. Ovulation usually occurs in each menstrual cycle. Thus, the younger a woman is when menstruation begins, the more opportunities there are for ovulation and the greater her exposure to estrogen.
2. Menopause after age 55. The older a woman is at menopause, the more menstrual cycles she is likely to have experienced. Estrogen levels are low and ovulation ceases after menopause.
3. Childlessness and late age at first pregnancy. Ovulation does not occur during pregnancy. Thus, pregnancy gives the ovaries a rest. Furthermore, the hormonal patterns of pregnancy appear to transform breast tissue in a way that protects against cancer. As a result, delaying pregnancy until after age 30 or remaining childless increases a woman's risk of developing breast cancer later in life.
4. Breast-feeding. Nursing may guard against breast cancer by blocking ovulation or by causing physiological changes that leave the breast tissue more resistant to cancer-producing chemicals in the environment. Women who breast-feed their infants have a 20% lower risk of developing breast cancer at a young age—before they reach menopause—than do women who bottle-feed their infants.
5. Exercise. Even moderate exercise can suppress ovulation (and thus estrogen levels) in adolescents and women in their twenties (but, unfortunately, exercise is not as likely to suppress ovulation in older women).
Other factors may also influence estrogen levels. For instance, obese women have higher estrogen levels than do thin ones because estrogen is produced in fat cells as well as by the ovaries. Indeed, obesity—especially if the fat is carried above the waist—translates to a threefold elevated risk of breast cancer.
Questions to Consider
• Federal guidelines no longer recommend routine mammograms for women over 40. The American Cancer Society says that routine mammograms reduce the number of mastectomies and deaths from breast cancer. Would you recommend that your female family members and friends who are over 40 get routine mammograms? Why or why not?
• Some women who carry the genes that increase the risk of breast cancer decide to have their breasts removed to prevent the occurrence of breast cancer. Would you recommend that your female family members and friends who have the genes for breast cancer have preventative mastectomies? Why or why not?
Disorders of the Female Reproductive System
Premenstrual syndrome (PMS) is a collection of symptoms that appear in some women 7 to 10 days before their period begins. These symptoms include depression, irritability, fatigue, and headaches.
Some researchers suggest that a progesterone deficiency is to blame for the symptoms of PMS. Progesterone has a calming effect on the brain. It also decreases fluid retention. As progesterone levels plummet in the days just before menstruation, the nervous system may be stimulated and fluids may be retained. Fluid retention causes an uncomfortable, bloated feeling.
Treatments for PMS are varied. For women whose symptoms are severe, drugs that elevate the levels of serotonin—a neurotransmitter in the brain (Chapter 7)—are administered. Some women with milder symptoms are helped by changes in diet. Caffeine, alcohol, fat, and sodium should be avoided. On the other hand, foods high in calcium, potassium, manganese, and magnesium should be increased. Aerobic exercise for at least half an hour a day stimulates the release of enkephalins and endorphins (brain chemicals that produce pleasure), which may provide some relief.
Prostaglandins, chemicals used in communication between cells in many parts of the body, are the primary cause of menstrual cramps. Endometrial cells produce prostaglandins that, among other things, make the smooth muscle cells of the uterus contract, causing cramps. High levels of prostaglandins can cause sustained contractions, called muscle spasms, of the uterus. These muscle spasms may cut down blood flow—and therefore, the oxygen supply to the uterine muscles—and result in pain.
Endometriosis is a condition in which tissue from the lining of the uterus is found outside the uterine cavity— commonly in the oviducts, on the ovaries, or on the outside surface of the uterus, the bladder, or the rectum. In these cases, the endometrial tissue has moved out the open ends of the oviducts to the abdominal cavity. Endometrial tissue, wherever it is, grows and breaks down with the hormonal changes that occur during each menstrual cycle. These cyclic changes can cause extreme pain. Moreover, women with endometriosis often have difficulty becoming pregnant because endometrial tissue may block the oviduct or coat the ovary.
Stages of the Human Sexual Response
In both men and women, sexual arousal and sexual intercourse involve two basic physiological changes: certain tissues fill with blood (vasocongestion) and certain muscles undergo sustained or rhythmic contractions (myotonia). However, men and women differ in which tissues fill with blood and which muscles contract. The sequence of events that accompanies sexual arousal and intercourse is called the sexual response cycle. Let's consider the four stages of the human response cycle in men and in women.
1. Excitement. During the excitement phase of the sexual response cycle, sexual arousal increases. This stage occurs during foreplay, the activities that precede sexual intercourse, and prepares the penis and vagina for intercourse. In a male, blood fills the spongy tissue of the penis, which becomes erect, as described earlier. In a female, blood flow to the breasts, nipples, labia, and clitoris causes these structures to swell. Partly due to an increase in blood flow, the vaginal walls seep fluid that serves as a lubricant, which makes the insertion of the penis easier. Breathing rate and heart rate increase.
2. Plateau. During the plateau stage, sexual arousal is maintained at a high level. The changes that began during the first phase will continue through the plateau stage until orgasm. In men, increased blood flow causes the testes to enlarge, and muscle contraction pulls them closer to the body. In women, increased blood flow causes the outer third of the vagina to enlarge and the clitoris to retract under the clitoral hood. In both men and women, breathing rate and heart rate continue to increase.
3. Orgasm. The peak of the sexual response cycle, orgasm, is brief but usually intensely pleasurable. In both sexes, orgasm is characterized by muscle contractions of the reproductive structures. In men, ejaculation occurs during orgasm. Ejaculation takes place in two stages. In the first stage, contractions of glands and ducts in the reproductive system force sperm and the secretions of the accessory glands to the urethra. During the second stage of ejaculation, the urethra contracts and semen is forcefully expelled from the penis. Orgasm in women involves rhythmic muscle contractions in the vagina and uterus. Some women experience orgasm rarely or not at all, and others can experience orgasm repeatedly. The absence of orgasm does not affect a woman's ability to become pregnant.
4. Resolution. During the resolution stage, the body slowly returns to its normal level of functioning. Resolution usually takes longer in women than it does in men. Many women are capable of becoming aroused again during the resolution phase, but men usually experience an interval during the resolution stage when it is impossible for them to achieve another erection or orgasm.
Birth Control
Sexual activity carries with it the risk of both unwanted pregnancy and the possibility of contracting a sexually transmitted disease (STD; many STDs are discussed in Chapter 17a). The method couples use (if any) to avoid pregnancy influences the chances of contracting STDs. For this reason, as we discuss various means of contraception, we will also consider whether they reduce the risk of spreading sexually transmitted infections.
Abstinence
Abstinence—not having sexual contact at all—is the most reliable way to avoid both pregnancy and the spread of STDs. However, abstinence is not always used as a means of contraception.
Sterilization
Well before the end of their reproductive life spans, most people have had all the children they want. Other than abstinence, sterilization is the most effective way to ensure that pregnancy does not occur. However, unlike abstinence, sterilization offers no protection against STDs.
Sterilization in men usually involves an operation called a vasectomy, in which the vas deferens on each side is cut to prevent sperm from leaving the man's body. The procedure usually takes about 20 minutes and can be performed in a physician's office under local anesthesia. The physician makes small openings in the scrotum through which each vas deferens can be pulled and cut; a small segment is removed, and at least one end is sealed shut. Because sperm make up only about 1% of the semen, the volume of semen the man ejaculates is not noticeably reduced. His interest in sex is not lessened, because testosterone, which is responsible for the sex drive, is still released from the interstitial cells of the testis and carried around the body in the blood.
The most common method of female sterilization, tubal ligation, involves blocking the oviducts to prevent the egg and sperm from meeting. Commonly, the tubes are cut and the ends seared shut or mechanically blocked with clips or rings. Tubal ligation is frequently done using a procedure called laparoscopy, in which two small incisions are made in the abdominal cavity and the operation is visualized through a telescopic lens inserted through one of them. Laparoscopy is generally performed in a hospital under general anesthesia. Because the abdominal cavity is opened, the risk of infection is greater after tubal ligation than it is after a vasectomy. A woman continues to menstruate after a tubal ligation, because the ovarian hormones continue to be produced in a cyclic manner.
A newer method of sterilization for women does not require an incision. Instead, a small wire coil is inserted into the oviducts through the vagina, cervix, and uterus. During the next 3 months, scar tissue forms around the coil and blocks the passage of sperm.
Sterilization should be considered permanent even though it is sometimes possible to reverse the procedure. At best, the reversal procedure is expensive and requires that the surgeon have special training in microsurgical techniques. Even then, success is not guaranteed.
Hormonal Contraception
Hormonal contraception is currently available only to females. There are two basic types: the methods that combine estrogen and progesterone and the progesterone-only means of contraception.
Combination estrogen and progesterone contraception. Several forms of birth control combine synthetic forms of estrogen and progesterone. Each of these methods works by mimicking the effects of natural hormones that would ordinarily be produced by the ovaries. Among these effects is the suppression of the release of FSH and LH from the anterior pituitary gland. Without these pituitary hormones, the egg does not mature and is not released from the ovary.
When most people speak about "the pill," they are referring to the combination birth control pill, so named because it contains synthetic forms of both estrogen and progesterone. A hormone-containing "combination" birth control pill is taken daily for 3 weeks, followed by a week of daily pills without hormones.
Over the past few years, additional methods of combined hormonal contraception have been developed. There is a skin patch (Ortho Evra) and a vaginal ring (NuvaRing), each of which slowly releases hormones for the 3 weeks it is in place (Figures 17.10a and 17.10b). When a woman uses the birth control pill, the vaginal ring, or the patch, she menstruates during the week in which hormones are not administered. Women who have difficulty remembering to take a pill each day may prefer these newer options. In addition, there are regimens of hormonal contraception (Seasonale and Seasonique) in which estrogen and progesterone pills are taken for 84 days, followed by a week of placebo pills or low-dose estrogen pills. A woman who is using Seasonale or Seasonique menstruates only four times a year, while taking the placebo pills. Lybrel is a regimen of pills that are taken continuously for one year, so that a woman menstruates only once a year.

FIGURE 17.10. Selected methods of birth control
For most healthy, nonsmoking women younger than 35 years of age, combination hormonal methods are extremely safe means of contraception. Nonetheless, a small number of hormonal contraceptive users do die each year from a complication, so the possibility of such complications should be recognized. The risk increases with age and with cigarette smoking. Hormonal contraception and cigarette smoking can both increase blood pressure and the risk of abnormal blood clot formation. Together, they have a greater effect than either does alone. Problems with the circulatory system are the most important of the serious (sometimes fatal) complications of hormonal contraception use. Most pill-associated deaths are caused by heart attack or stroke that results when the blood supply to the heart or a region of the brain is blocked. Hormonal contraception also increases the risk of abnormal blood clot formation.
Women who use combination hormonal contraceptives have a greater risk of catching certain STDs from an infected partner than do women who use other forms of birth control or no birth control at all. One way the pill increases the likelihood of transmission of these diseases is by making the vaginal environment more alkaline, a condition that favors the growth of bacteria that cause gonorrhea and chlamydia. Another reason that women on the pill have a greater risk of getting STDs is that it makes the user's cervix more vulnerable to disease-causing organisms; the pill causes delicate cells that line the cervical canal to migrate to the exposed surface of the cervix.
Progesterone-only contraception The most popular form of progesterone-only contraception is an injection (Depo- Provera) given every 3 months. Progesterone injections are an extremely effective means of contraception. There is also a progesterone-only pill (POP; also called the minipill). As when using the combined birth control pill, a woman must take the minipill faithfully every day. POPs are generally less effective than the combined pill. A progesterone-releasing intrauterine device (IUD; discussed shortly) is also available. A progesterone-containing implant, Implanon is a slender, flexible silicone rod about the size of a matchstick. An Implanon rod, when inserted under the skin in a woman's upper arm, is barely visible and provides extremely effective protection for three years as the progesterone slowly diffuses out of the capsules.
Progesterone-only contraceptives can prevent pregnancy in several ways. All types may prevent ovulation, but they vary in their ability to do so. They all cause thickening of cervical mucus, which hampers the passage of sperm to reach the egg. In addition, because estrogen is not used in this contraceptive, the endometrium is not prepared properly for the implantation of an embryo should fertilization occur. An important drawback is that progesterone-only contraceptives provide no protection against sexually transmitted diseases.
What would you do?
Clinical trials are under way to test the safety and effectiveness of various forms of hormonal birth control implants designed to be used by males. The hormones reduce sperm levels enough to make a man infertile, and sperm production resumes within a few months without the hormones. The implants do not protect against STDs. If you were a male in a long-term relationship, would you volunteer for this study? If you were the female in this relationship, would you want your partner to participate in the study? What criteria would you use to decide?
Intrauterine Devices
An intrauterine device (IUD) is a small device that is inserted into the uterus by a physician to prevent pregnancy (Figure 17.10c). It can be left in place for several years and should be removed by a physician. An IUD is highly effective in preventing pregnancy. It can interfere with both fertilization and implantation. However, IUDs offer no protection against the spread of sexually transmitted diseases. In the future, there may be a male equivalent of an IUD, called an Intra Vas Device, which is a plug inserted into the vas deferens to block the passage of sperm.
A risk associated with using an IUD is pelvic inflammatory disease, which is a general term for any bacterial infection of the pelvic organs. The risk is greatest in the weeks following IUD insertion, because disease-causing organisms, usually sexually transmitted organisms, can enter the uterus from the vagina at this time. The risk of pelvic infection due to an IUD is low—less than 1%. However, if it does occur, it can lead to sterility or ectopic pregnancy.
Barrier Methods
Barrier methods of contraception include the diaphragm, cervical cap, contraceptive sponge, and male and female condoms. Methods in this category work, as their name suggests, by creating a barrier between the egg and sperm.
A diaphragm is a dome-shaped, soft rubber cup containing a flexible ring. It is inserted into the vagina before intercourse so that it covers the cervix, preventing sperm from passing through (Figure 17.10d). A cervical cap is smaller than a diaphragm and fits snugly over the cervix. Before the diaphragm or cervical cap is inserted, spermicidal cream or jelly should be added to the inner surface. Because a diaphragm covers the cervix and the top of the vagina, it offers some, though limited, protection to the woman against important STDs, including chlamydia and gonorrhea. By protecting the cervix from the virus that causes genital warts, many types of which cause cervical cancer, it also lessens the risk of cervical cancer. A cervical cap, being smaller, offers no protection against STDs.
Unlike a diaphragm or cervical cap, a contraceptive sponge or condom can be purchased without a prescription. A contraceptive sponge is a small sponge that contains a spermkilling chemical. One side of the sponge has an indentation that the cervix fits into. The other side has a strap that makes removal easier. To activate the spermicide, the sponge must be thoroughly moistened before use. It is then inserted and offers protection against pregnancy for the next 24 hours.
The male condom is a thin sheath of latex, polyurethane, or natural membranes ("skin") that is rolled onto an erect penis, where it fits like a glove (Figure 17.10e). The sperm are trapped within the condom and cannot enter the vagina. The effectiveness of condoms in preventing pregnancy depends largely on how consistently they are used.
Other than complete abstinence from sexual activity, the latex condom is the best means of preventing the spread of STDs available today. The skin condoms may offer greater sensitivity; but they do allow some microorganisms, particularly viruses, to pass through. Latex has no pores, so microorganisms cannot pass through it. Health advisors highly recommend that people who might be exposed to STDs use a latex condom for disease protection, even if they are already using another means of birth control to prevent pregnancy. Keep in mind, however, that a condom can prevent disease transmission only between the body surfaces it separates. Diseases can still be spread by contact between other, unprotected body surfaces that are vulnerable to infection.
The female condom is a loose sac of polyurethane, a clear plastic that resembles the type used in a food-storage bag. At each end of the sac is a flexible ring that helps hold the device in place (Figure 17.10f). The female condom does reduce the risk of spreading sexually transmitted infections. Female condoms offer a barrier against STDs and prevent pregnancy for women who cannot count on their male partner to use condoms.
Stop and think
A latex condom provides an impenetrable barrier to disease- causing organisms. Yet, studies indicate that women who use a diaphragm or vaginal sponge routinely have lower rates of STDs than do women who rely on their male partners to use a condom. What might explain this seemingly illogical difference?
Spermicidal Preparations
Spermicidal preparations consist of a sperm-killing chemical (nonoxynol-9) in some form of carrier, such as foam, cream, jelly, film, or tablet. When spermicide is used without any other means of contraception, foams are the most effective option because they act immediately and disperse more evenly than other preparations. The sperm-killing effect of any spermicide lasts for about 1 hour after the product has been activated. Laboratory tests have shown that nonoxynol-9 kills the organisms responsible for many STDs. However, this chemical also damages the cells lining the vagina, and this damage could increase a woman's susceptibility to STDs.
Fertility Awareness
Fertility awareness, which also goes by the names of natural family planning and the rhythm method, is a way to reduce the risk of pregnancy by avoiding intercourse on all days on which sperm and egg might meet. This sounds easier than it is. Sperm can live in the female reproductive tract for 2 to 5 days, but the lower value is most likely. An egg lives only 12 to 24 hours after ovulation. Consequently, there are only 4 days in each cycle during which fertilization might occur. But which 4 days? Therein lies the problem. It is difficult enough to pinpoint when ovulation occurs, much less predict it several days in advance. The situation is not entirely hopeless, however. There are several ways for a woman to track her menstrual cycle: the calendar, body temperature, and cervical mucus. All of these methods require training to be used effectively.
Emergency Contraception
Emergency contraception, or the so-called morning-after pill, is a means of contraception that can actually be used in the first few days after unprotected intercourse. Doctors have prescribed birth control pills and inserted IUDs as emergency contraception for decades, but only recently have two pills specifically marketed for this use become available in the United States. One type (Preven) combines estrogen and progesterone. The second type (Plan B) contains only progesterone. With either type, the first dose should be taken within 3 to 5 days of unprotected intercourse and the second 12 hours later. Scientists do not fully understand the precise mechanisms of action; possible explanations for the pill's efficacy include inhibition or delay of ovulation, prevention of fertilization, thickening of cervical mucus, and alteration of the endometrium, making it an inhospitable place for implantation of the young embryo. Plan B can be purchased over the counter in a pharmacy by women 18 years of age or older.
Looking ahead
In this chapter, we have seen how the male and female reproductive systems function to produce offspring. Unfortunately, during sexual intimacy, the vulnerable surfaces of certain parts of the reproductive system come into contact, potentially allowing sexually transmitted organisms to spread. We explore this topic further in the next chapter.
__________________________________________________________
1 Above a critical level, estrogen exerts a positive feedback on the brain and anterior pituitary gland.
Highlighting the Concepts
Gonads (p. 332)
• The gonads (testes and ovaries) are the reproductive structures that produce the gametes (sperm and eggs), as well as sex hormones. Male testes produce the sex hormone testosterone.
Female ovaries produce the sex hormones estrogen and progesterone. A sperm and egg fuse at fertilization, producing a cell called a zygote that under the right circumstances will develop into a new individual.
Male and Female Reproductive Roles (pp. 332-333)
• A male produces a large number of sperm and delivers them to the female reproductive system. A female usually produces only one nutrient-filled egg during each approximately month-long interval. The female also nourishes and protects the developing baby (the embryo and later the fetus) in her uterus.
Form and Function of the Male Reproductive System (pp.333-338)
• The male reproductive system is composed of the testes, a series of ducts (the epididymis, vas deferens, and urethra), accessory glands (the prostate, seminal vesicles, and bulbourethral glands), and the penis.
• The testes are located outside the body cavity in a sac called the scrotum, which helps regulate the temperature of the testes to ensure proper sperm development.
• Within the seminiferous tubules of the testes, the production of gametes, called spermatogenesis, is a continuous process. Sperm are haploid gametes produced by meiosis.
• After leaving the seminiferous tubules, sperm mature and are stored in the epididymis. At ejaculation, sperm travel through the vas deferens and the urethra to leave the body.
• Semen is the fluid released when a man ejaculates. Most of the semen consists of the secretions of the accessory glands.
• The penis transfers sperm to the female during sexual intercourse. Erectile dysfunction is the inability to achieve or maintain an erection. There are several options for treatment.
• Each sperm has three distinct regions. The head of the sperm contains the male's genetic contribution to the next generation. The midpiece is packed with mitochondria, which produce ATP to power movement. The whiplike tail propels the sperm to the egg.
• In males, the hormone testosterone is produced by the interstitial cells, which are located within the testes between the seminiferous tubules.
• Male reproductive processes are regulated by an interplay of hormones from the anterior pituitary gland in the brain (LH and FSH), from the hypothalamus (GnRH), and from the testes (testosterone and inhibin).
Form and Function of the Female Reproductive System (pp.338-344)
• The female reproductive system consists of the ovaries, oviducts, uterus, vagina, and external genitalia.
• The ovaries produce eggs and the sex hormones estrogen and progesterone.
• The oviducts transport the immature egg, zygote, and then the early embryo to the uterus. Fertilization usually occurs in the oviduct.
• The uterus supports the growth of the developing baby (embryo and then fetus). The embryo implants in the lining of the uterus, the endometrium, which provides nourishment during development. The muscular wall of the uterus allows the uterus to stretch as the fetus grows, and contractions of the muscle force the baby out of the uterus during childbirth. The cervix is the opening of the uterus.
• The female breasts produce milk to nourish the baby after childbirth.
• The events of the ovarian cycle lead to the release of an egg. A female is born with a finite number of primary follicles. A primary follicle is a primary oocyte (an immature egg) surrounded by a single layer of follicle cells. The primary oocytes will remain in this state until puberty, when (usually) one each month will resume development and be ovulated as a secondary oocyte.
• Hormones from the pituitary gland (FSH and LH) and from the ovary (estrogen and progesterone) regulate the ovarian cycle (which prepares an egg for fertilization) and the uterine or menstrual cycle (which prepares the endometrium of the uterus for implantation of the embryo). However, if the egg is fertilized, the young embryo produces human chorionic gonadotropin (HCG), which maintains the corpus luteum. HCG is the hormone that pregnancy tests detect.
• At menopause, which usually occurs between the ages of 45 and 55, menstruation and ovulation stop. As a result, the levels of estrogen and progesterone drop. Menopause has many psychological and physiological effects on a woman's body.
Disorders of the Female Reproductive System (pp. 344-345)
• Premenstrual syndrome (PMS), a collection of symptoms that occur in some women several days before their period begins, may be caused by low levels of progesterone or of the brain chemical serotonin. Menstrual cramps are caused by prostaglandins, which make muscles contract.
• Endometriosis is a condition in which endometrial tissue is found outside the uterus.
Stages of the Human Sexual Response (p. 346)
• The human sexual response is the sequence of events that occur during sexual intercourse. This cycle consists of four phases: excitement (increased arousal), plateau (continued arousal), orgasm (climax), and resolution (return to a normal level of functioning).
Birth Control (pp. 346-349)
• Abstinence (refraining from intercourse) and sterilization (vasectomy or tubal ligation) are the most effective ways to prevent pregnancy. Hormonal contraception (combined estrogen plus progesterone or progesterone-only methods) interferes with the regulation of reproductive processes. An intrauterine device interferes with fertilization and implantation. Barrier methods of contraception (the diaphragm, cervical cap, contraceptive sponge, and male or female condom) prevent the union of sperm and egg. Spermicidal preparations kill sperm. Natural family planning (the rhythm method) consists of abstinence at times when fertilization could occur.
• Morning-after pills are emergency contraception that can reduce the risk of an unwanted pregnancy resulting from unprotected intercourse.
Reviewing the Concepts
1. Name the male and female gonads. What are the functions of these organs? p. 332
2. How is the temperature maintained in the testes? Why is temperature control important? p. 333
3. Trace the path of sperm from their site of production to their release from the body, naming each tube the sperm pass through. p. 333
4. Name the male accessory glands and give their functions. pp. 334-335
5. What is the function of the penis in reproduction? Describe the process by which the penis becomes erect. p. 336
6. Name and describe the functions of the three regions of a sperm cell. p. 336
7. List the hormones from the hypothalamus, the anterior pituitary gland, and the testes that are important in the control of sperm production. Explain the interactions between these hormones. p. 337
8. What are the two main layers in the wall of the uterus? p. 338
9. List the major structures of the female reproductive system and give their functions. pp. 338-339
10. What is an ectopic pregnancy? Why is it dangerous to the mother's health? p. 338
11. Describe the structure of female breasts. What is their function? pp. 338-339
12. Describe the ovarian cycle. Include in your description primary oocytes, primary follicles, mature Graafian follicles, and the corpus luteum. pp. 338-339
13. Describe the interplay of hormones from the anterior pituitary and from the ovaries that is responsible for the menstrual cycle. pp. 340-343
14. What is menopause? Why does menopause lower estrogen levels? What are some effects of lowered estrogen levels? pp. 343-344
15. What are the stages of the human sexual response? p. 346
16. Describe a vasectomy and a tubal ligation. p. 346
17. How does the combination birth control pill reduce the chances of pregnancy? p. 347
18. What health risks are associated with use of the birth control pill? p. 347
19. How do progesterone-only means of contraception reduce the risk of pregnancy? p. 347
20. What is an IUD? p. 348
21. How do the diaphragm, male condom, and female condom prevent pregnancy? p. 348
22. The interstitial cells
a. are found in the seminal vesicles.
b. produce a secretion that makes up most of the volume of semen.
c. secrete testosterone.
d. store sperm.
23. Choose the incorrect statement about semen.
a. It helps lubricate passageways in the male reproductive system, so sperm travel through them more easily.
b. Sperm cells make up most of the volume of semen.
c. It helps reduce the acidity of the female reproductive system, thereby increasing sperm survival.
d. It contains nourishment for the sperm.
24. After sperm are released in the female reproductive system, they can move to the egg and fertilize it. Which is the correct order of structures through which the sperm will pass?
a. Vagina, cervix, body of uterus, oviduct
b. Ovary, cervix, body of uterus, oviduct
c. Endometrium, cervix, oviduct, ovary
d. Ovary, oviduct, endometrium, cervix
25. Which is the correct pairing of a structure with its function?
a. Endometrium; the usual site of fertilization
b. Corpus luteum; production of estrogen and progesterone
c. Epididymis; production of testosterone
d. Seminal vesicles; store sperm while they mature
26. The controversial pill Mifepristone (formerly called RU486) works to terminate a pregnancy by preventing progesterone from acting. This effect would cause an abortion because prog esterone is needed to
a. trigger ovulation.
b. cause the formation of the corpus luteum.
c. maintain the endometrium.
d. increase the levels of LH.
27. Sperm are stored and mature in the _____.
28. Fertilization usually occurs in the _____.
Applying the Concepts
1. You are a health care provider in a family planning clinic. Your first client is a woman who is 22 years old and in excellent health. She is about to marry her high school sweetheart. She and her fiance have never had sexual intercourse with anyone else. They want a very effective means of contraception because they would like to wait until he finishes graduate school to start a family. She does not smoke. Which means of birth control would you recommend for this client? Why?
2. Endometriosis, a condition in which endometrial tissue implants on pelvic organs outside the uterus, causes pain in the pelvic area. Why would the pain be greatest around the time of menstruation?
3. A male friend of yours and his wife would like to have a baby. They are having difficulty conceiving a child. The doctor told him that the reason for this difficulty is a low sperm count. Since further tests are costly and would take time to complete, the doctor told your friend that as a first step, he might try wearing loose clothing and switching to boxer shorts, rather than his customary tight briefs. Why do you think the doctor made this suggestion?
Becoming Information Literate
Use at least three reliable sources (journals, newspaper, websites) to answer the following questions. Explain why you chose those sources.
1. Three extended-use hormonal contraceptives are available for women: Lybrel (used for one year) Seasonale, and Seasonique (both used for 90 days). How do these contraceptives prevent pregnancy? Are they safe? What are the pros and cons of using them?
2. There is contradictory evidence that environmental estrogens are affecting human reproductive systems. What are some effects that some researchers attribute to environmental estrogen? Discuss the evidence for and against a link between environmental estrogens and at least one of these effects.