MCAT Biology Review
Chapter 2: Reproduction
2.3 The Reproductive System
Biological sex is determined by the 23rd pair of chromosomes, with XX being female and XY being male. An ovum can only carry the X chromosome, while sperm can carry either the X or Y chromosome. The X chromosome carries a sizeable amount of genetic information; mutations in these genes can cause sex-linked (X-linked) disorders. Males are termed hemizygous with respect to many of the genes on the X chromosome because they only have one copy. Therefore, a male with a disease-causing allele on the unpaired part of X chromosome will necessarily express that allele. Females, on the other hand, may be homozygous or heterozygous with respect to genes on the X chromosome. Most X-linked disorders are recessively inherited; therefore, females express these disorders far less frequently than males. Females carrying a diseased allele on an X-chromosome, but not exhibiting the disease, are said to be carriers.
MNEMONIC
Sex-linked is X-linked.
Comparatively, the Y chromosome contains very little genetic information. One notable gene on the Y chromosome is SRY (sex-determining region Y), which codes for a transcription factor that initiates testis differentiation and, thus, the formation of male gonads. Therefore, in the absence of the Y chromosome, all zygotes will be female. In the presence of the Y chromosome, a zygote will be male.
REAL WORLD
In reality, there are a handful of Y-linked diseases, most of which result in reduced fertility. A father will pass a Y-linked disease to all of his sons, assuming fertility has not been lost. These diseases are extremely rare, and are not included on the official MCAT content lists.
MALE REPRODUCTIVE ANATOMY
The male reproductive system is shown in Figure 2.7.
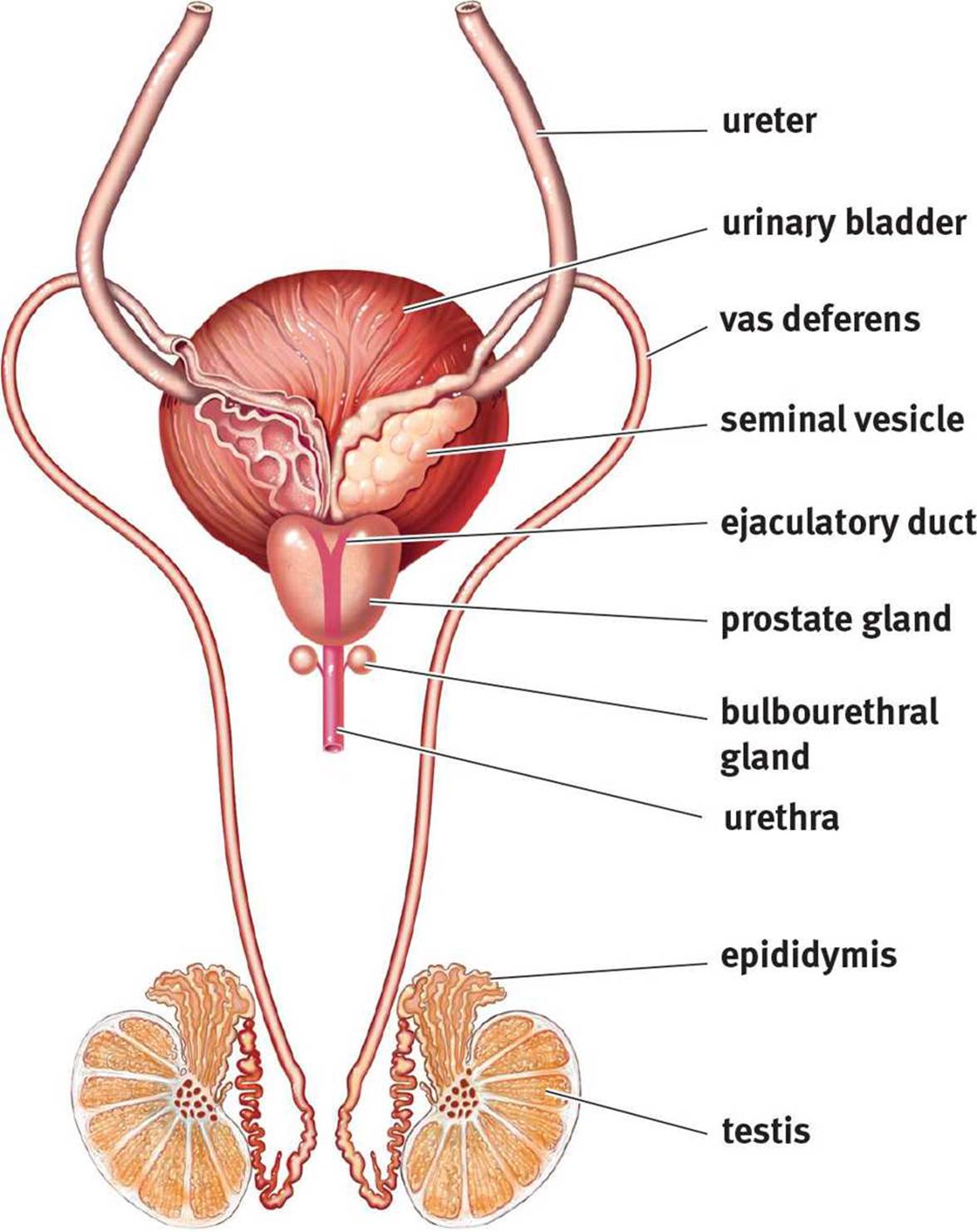 Figure 2.7. Male Reproductive System
Figure 2.7. Male Reproductive System
In males, the primitive gonads develop into the testes. The testes have two functional components: the seminiferous tubules and the interstitial cells (of Leydig). Sperm are produced in the highly coiled seminiferous tubules, where they are nourished by Sertoli cells. The cells of Leydig secrete testosterone and other male sex hormones (androgens). The testes are located in the scrotum, which is an external pouch that hangs below the penis and maintains a temperature 2° to 4°C lower than the body. In fact, there is a layer of muscle around the vas deferens (ductus deferens) that can raise and lower the testis to maintain the proper temperature for sperm development.
As sperm are formed, they are passed to the epididymis where their flagella gain motility, and they are then stored until ejaculation. During ejaculation, sperm travel through the vas deferens to the ejaculatory duct at the posterior edge of the prostate gland. The two ejaculatory ducts then fuse to form the urethra, which carries sperm through the penis as they exit the body. In males, the reproductive and urinary systems share a common pathway; this is not the case in females.
MNEMONIC
Pathway of sperm through the male reproductive system: SEVE(N) UP
· Seminiferous tubules
· Epididymis
· Vas deferens (also called the ductus deferens)
· Ejaculatory duct
· (Nothing)
· Urethra
· Penis
As sperm pass through the reproductive tract, they are mixed with seminal fluid, which is produced through a combined effort by the seminal vesicles, prostate gland, and bulbourethral gland. The seminal vesicles contribute fructose to nourish sperm, and both the seminal vesicles andprostate gland give the fluid mildly alkaline properties so the sperm will be able to survive in the relative acidity of the female reproductive tract. The bulbourethral (Cowper’s) glands produce a clear viscous fluid that cleans out any remnants of urine and lubricates the urethra during sexual arousal. The combination of sperm and seminal fluid is known as semen.
REAL WORLD
The prostate enlarges with age and frequently causes problems in older males, including benign prostatic hypertrophy. Because the prostate surrounds the urethra, classic symptoms of this condition include urinary frequency, urgency, and nighttime awakenings to use the bathroom.
Spermatogenesis
As mentioned above, spermatogenesis, the formation of haploid sperm through meiosis, occurs in the seminiferous tubules. In males, the diploid stem cells are known as spermatogonia. After replicating their genetic material (S stage), they develop into diploid primary spermatocytes. The first meiotic division will result in haploid secondary spermatocytes, which then undergo meiosis II to generate haploid spermatids. Finally, the spermatids undergo maturation to become mature spermatozoa. Spermatogenesis results in four functional sperm for each spermatogonium.
Mature sperm are very compact. They consists of a head (containing the genetic material), a midpiece (which generates ATP from fructose), and a flagellum (for motility), as shown in Figure 2.8. The midpiece is filled with mitochondria, which generate the energy to be used as the sperm swims through the female reproductive tract to reach the ovum in the fallopian tubes. Each sperm head is covered by a cap known as an acrosome. This structure is derived from the Golgi apparatus and is necessary to penetrate the ovum. Once a male reaches sexual maturity during puberty, approximately 3 million sperm are produced per day through the rest of life.
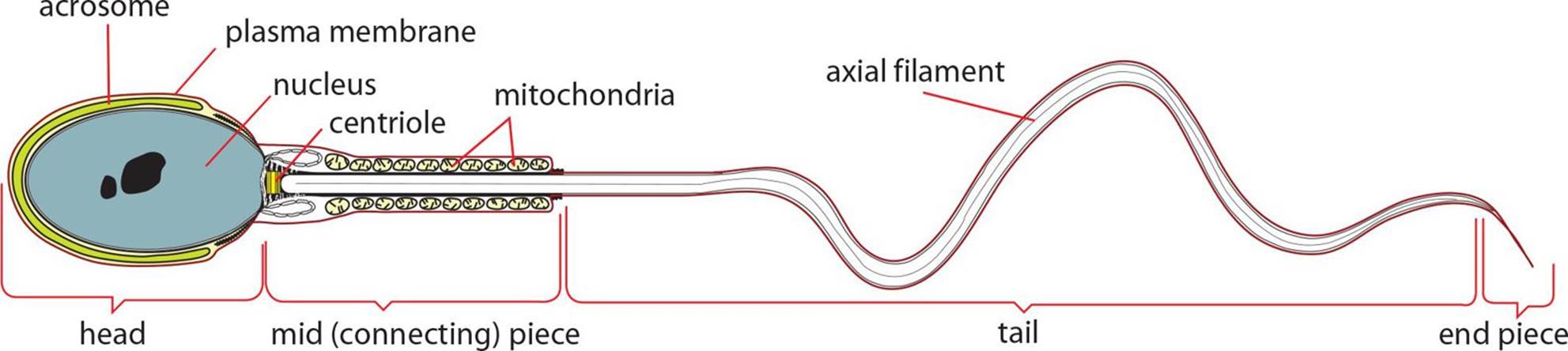 Figure 2.8. Structure of a Mature Sperm
Figure 2.8. Structure of a Mature Sperm
FEMALE REPRODUCTIVE ANATOMY
Unlike the male reproductive system, all of the female reproductive organs are internal, as shown in Figure 2.9. The gonads, known as ovaries, produce estrogen and progesterone. The ovaries are located in the pelvic cavity; each consists of thousands of follicles, which are multilayered sacs that contain, nourish, and protect immature ova (eggs). Between puberty and menopause, one egg per month is ovulated through the peritoneal sac, which lines the abdominal cavity. It is then drawn into the fallopian tube or oviduct, which is lined with cilia to propel the egg forward. The fallopian tubes are connected to the muscular uterus, which is the site of fetal development. The lower end of the uterus, known as the cervix, connects to the vaginal canal, where sperm are deposited during intercourse. The vagina is also the passageway through which childbirth occurs. The external female anatomy is known collectively as the vulva. As mentioned earlier, females have separate excretory and reproductive tracts.
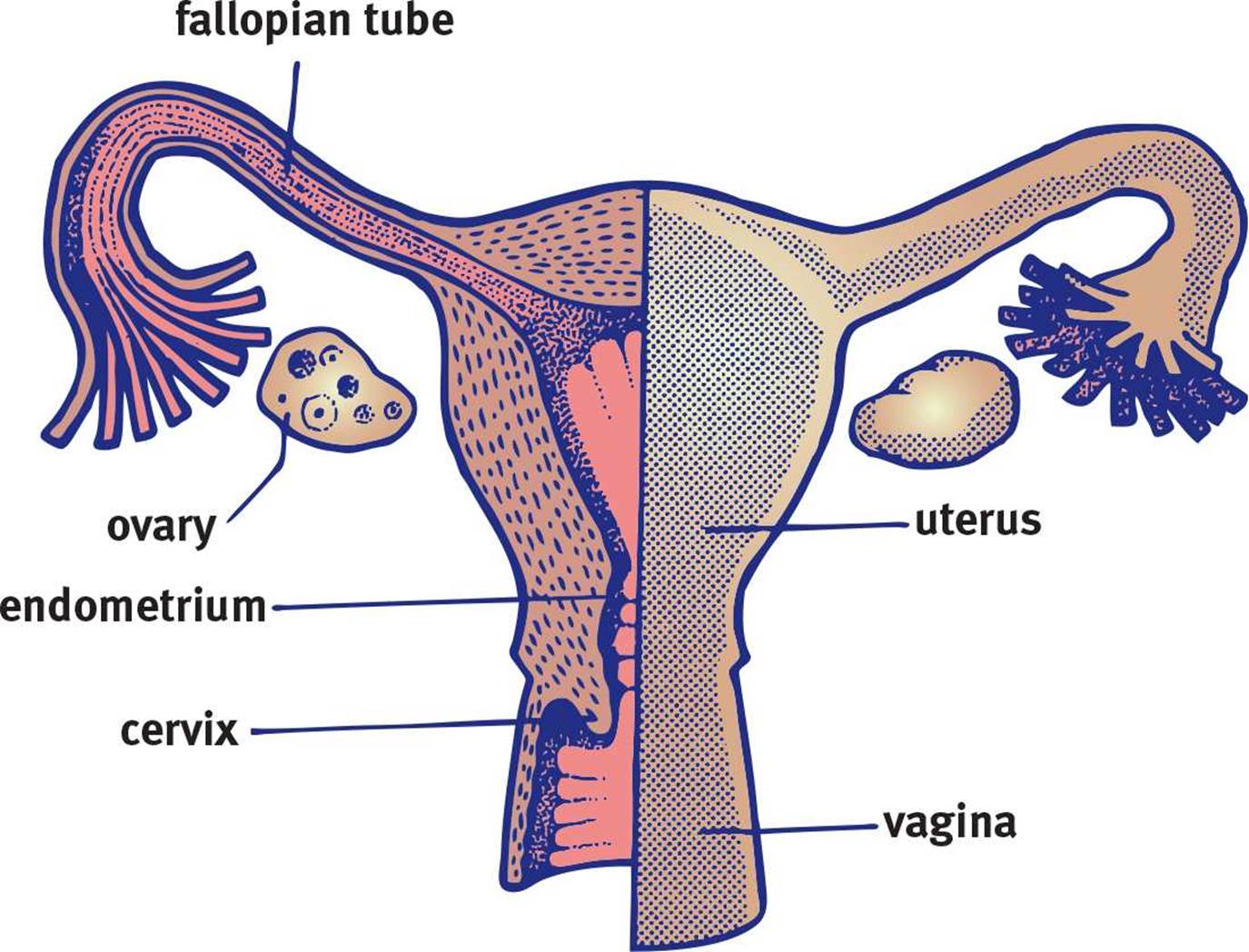 Figure 2.9. Female Reproductive System
Figure 2.9. Female Reproductive System
Oogenesis
The production of female gametes is known as oogenesis. Although gametocytes undergo the same meiotic process in both females and males, there are some significant differences between the two sexes. First, there is no unending supply of stem cells analogous to spermatogonia in females; all of the oogonia a woman will ever have are formed during fetal development. By birth, all of the oogonia have already undergone DNA replication and are considered primary oocytes. These cells are 2n, like primary spermatocytes, and are actually arrested in prophase I. Once a woman reaches menarche (her first menstrual cycle), one primary oocyte per month will complete meiosis I, producing a secondary oocyte and a polar body. The division is characterized by unequal cytokinesis, which doles ample cytoplasm to one daughter cell (the secondary oocyte) and nearly none to the other (the polar body). The polar body generally does not divide any further and will never produce functional gametes. The secondary oocyte, on the other hand, remains arrested in metaphase II and does not complete the remainder of meiosis II unless fertilization occurs.
Oocytes are surrounded by two layers: the zona pellucida and the corona radiata. The zona pellucida surrounds the oocyte itself and is an acellular mixture of glycoproteins that protect the oocyte and contain compounds necessary for sperm cell binding. The corona radiata lies outside the zona pellucida and is a layer of cells that adhered to the oocyte during ovulation. Meiosis II is triggered when a sperm cell penetrates these layers with the help of acrosomal enzymes. The secondary oocyte undergoes the second meiotic division to split into a mature ovum and another polar body, which will eventually be broken down. A mature ovum is a very large cell consisting of large quantities of cytoplasm and organelles; indeed, the ovum contributes nearly everything to the zygote (half of the DNA, cytoplasm, organelles including mitochondria, RNA for early cellular processes, and physical space), whereas sperm only contribute half of the DNA. Upon completion of meiosis II, the haploid pronuclei of the sperm and the ovum join, creating a diploid zygote.
SEXUAL DEVELOPMENT
The ability to reproduce is under hormonal control. Prior to puberty, the hypothalamus restricts production of gonadotropin-releasing hormone (GnRH). At the start of puberty, this restriction is lifted as the hypothalamus releases pulses of GnRH, which then triggers the anterior pituitary gland to synthesize and release follicle- stimulating hormone (FSH) and luteinizing hormone (LH). These hormones trigger the production of other sex hormones that develop and maintain the reproductive system.
Male Sexual Development
During the fetal period (from 9 weeks after fertilization until birth), presence of the Y chromosome allows for production of androgens, resulting in male sexual differentiation. For the duration of infancy and childhood, androgen production is low. Testosterone, produced by the testes, increases dramatically during puberty, and sperm production begins. In order to achieve this, there is a delicate interplay of FSH and LH stimulation on two cell types in the testes. FSH stimulates the Sertoli cells and triggers sperm maturation, whereas LH causes the interstitial cells to produce testosterone. Testosterone not only develops and maintains the male reproductive system, but also results in the development of secondary sexual characteristics, such as facial and axillary hair, deepening of the voice, and changes in growth patterns. Testosterone production remains high through adulthood and declines as men age. This hormone exerts negative feedback on the hypothalamus and anterior pituitary, so that production is limited to appropriate levels.
REAL WORLD
If the receptors for testosterone are absent or defective, it cannot exert its effects. The result is a condition called androgen insensitivity syndrome (AIS), in which a genetic male (XY) has female secondary sexual characteristics. In complete androgen insensitivity, a genetic male will appear female at birth. Often, these individuals are not discovered until puberty when they are examined for amenorrhea (failure to menstruate).
Female Sexual Development
The ovaries, which are derived from the same embryonic structures as the testes, are also under the control of FSH and LH secreted by the anterior pituitary. The ovaries produce estrogens and progesterone.
Estrogens are secreted in response to FSH, and they result in the development and maintenance of the female reproductive system and female secondary sexual characteristics (breast growth, widening of the hips, changes in fat distribution). In the embryo, estrogens stimulate development of the reproductive tract. In adults, estrogens lead to the thickening of the lining of the uterus (endometrium) each month in preparation for the implantation of a zygote.
Progesterone is secreted by the corpus luteum—the remnant follicle that remains after ovulation—in response to LH. Interestingly, progesterone is involved in the development and maintenance of the endometrium, but not in the initial thickening of the endometrium—this is the role of estrogen. This means that both estrogen and progesterone are required for the generation, development, and maintenance of an endometrium capable of supporting a zygote. By the end of the first trimester of a pregnancy, progesterone is supplied by the placenta, and the corpus luteum atrophies and ceases to function.
MNEMONIC
Estrogen establishes and progesterone protects the endometrium.
THE MENSTRUAL CYCLE
During the reproductive years (from menarche to menopause), estrogen and progesterone levels rise and fall in a cyclic pattern. In response, the endometrial lining will grow and be shed. This is known as the menstrual cycle and can be divided into four events, as shown in Figure 2.10: the follicular phase, ovulation, the luteal phase, and menstruation.
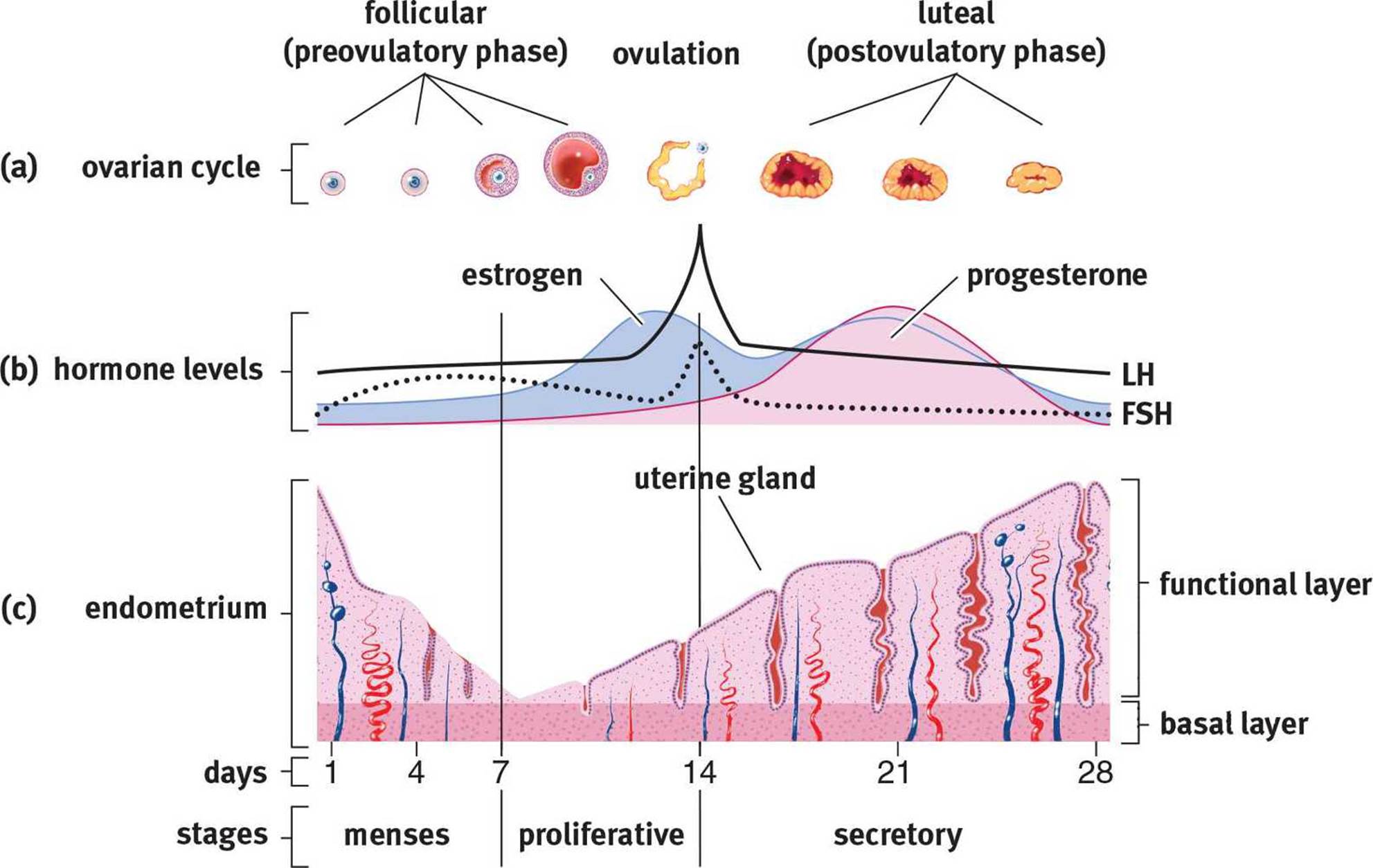 Figure 2.10. The Menstrual Cycle (a) Follicule-stimulating hormone (FSH) facilitates the maturation of a single ovum; (b) The peak of luteinizing hormone (LH) around day 14 marks ovulation, the release of the oocyte from the follicle; (c) The endometrial lining of the uterus reaches its peak in the luteal phase and is shed at the beginning of the next cycle.
Figure 2.10. The Menstrual Cycle (a) Follicule-stimulating hormone (FSH) facilitates the maturation of a single ovum; (b) The peak of luteinizing hormone (LH) around day 14 marks ovulation, the release of the oocyte from the follicle; (c) The endometrial lining of the uterus reaches its peak in the luteal phase and is shed at the beginning of the next cycle.
Follicular Phase
The follicular phase begins when the menstrual flow, which sheds the uterine lining of the previous cycle, begins. GnRH secretion from the hypothalamus increases in response to the decreased concentrations of estrogen and progesterone, which fall off toward the end of each cycle. The higher concentrations of GnRH cause increased secretions of both FSH and LH. These two hormones work in concert to develop several ovarian follicles. The follicles begin to produce estrogen, which has negative feedback effects and causes the GnRH, LH, and FSH concentrations to level off. Estrogen works to regrow the endometrial lining, stimulating vascularization and glandularization of the decidua.
Ovulation
Estrogen is interesting in that it can have both negative and positive feedback effects. Late in the follicular phase, the developing follicles secrete higher and higher concentrations of estrogen. Eventually, estrogen concentrations reach a threshold that paradoxically results in positive feedback, and GnRH, LH, and FSH levels spike. The surge in LH is important; it induces ovulation, the release of the ovum from the ovary into the abdominal (peritoneal) cavity.
Luteal Phase
After ovulation, LH causes the ruptured follicle to form the corpus luteum, which secretes progesterone. Remember that estrogen helps regenerate the uterine lining, but it is progesterone that maintains it for implantation. Progesterone levels begin to rise, while estrogen levels remain high. The high levels of progesterone again cause negative feedback on GnRH, FSH, and LH, preventing the ovulation of multiple eggs.
REAL WORLD
Oral contraceptive pills (OCPs) are simply estrogen/progesterone (or progesterone-only) preparations. These block conception by inhibiting LH and FSH release through negative feedback, thereby inhibiting ovulation. When a woman takes the placebo pills at the end of the month, withdrawal menstruation still occurs because estrogen and progesterone levels drop, but there is no egg that passes with the menstrual flow.
Menstruation
Assuming that implantation does not occur, the corpus luteum loses its stimulation from LH, progesterone levels decline, and the uterine lining is sloughed off. The loss of high levels of estrogen and progesterone removes the block on GnRH so that the next cycle can begin.
MCAT EXPERTISE
The MCAT likes to test your ability to identify graphs of the blood concentrations of FSH, LH, estrogen, and progesterone through the menstrual cycle. Be sure to know when each peaks by studying Figure 2.10.
Pregnancy
On the other hand, if fertilization has occurred, the resulting zygote will develop into a blastocyst that will implant in the uterine lining and secrete human chorionic gonadotropin (hCG). This hormone is an analog of LH, meaning that it looks very similar chemically and can stimulate LH receptors. This maintains the corpus luteum. hCG is critical during first trimester development because it is the estrogen and progesterone secreted by the corpus luteum that keep the uterine lining in place. By the second trimester, hCG levels decline because the placenta has grown to a sufficient size to secrete progesterone and estrogen by itself. The high levels of estrogen and progesterone continue to serve as negative feedback mechanisms, preventing further GnRH secretion.
KEY CONCEPT
Menstrual cycle:
· Follicles mature during the follicular phase (FSH, LH)
· LH surge at midcycle triggers ovulation
· Ruptured follicle becomes corpus luteum, which secretes estrogen and progesterone to build up uterine lining in preparation for implantation; LH and FSH are inhibited
· If fertilization does not occur, corpus luteum atrophies, progesterone and estrogen levels decrease, menses occurs, and LH and FSH levels begin to rise again
Menopause
As a woman ages, her ovaries become less sensitive to FSH and LH, resulting in ovarian atrophy. As estrogen and progesterone levels drop, the endometrium also atrophies, and menstruation stops. Also, because the negative feedback on FSH and LH is removed, the blood levels of these two hormones rise. This is called menopause. Profound physical and physiological changes usually accompany this process, including flushing, hot flashes, bloating, headaches, and irritability. Menopause usually occurs between the ages of 45 and 55.
MCAT Concept Check 2.3:
Before you move on, assess your understanding of the material with these questions.
1. What are the functions of interstitial cells of Leydig and Sertoli cells?
· Interstitial cells of Leydig:
· Sertoli cells:
2. During which phase of meiosis is a primary oocyte arrested? During which phase of meiosis is a secondary oocyte arrested?
· Primary oocyte:
· Secondary oocyte:
3. What is an acrosome? What organelle forms the acrosome?
4. What are the four phases of the female menstrual cycle? What are the features and relative hormone concentrations of each phase? (Note: Draw in symbols to signify the levels of each hormone, such as ↑, =, and ↓)
|
Phase |
Key Features |
FSH |
LH |
Estrogen |
Progesterone |