MCAT Biology Review
Chapter 11: The Musculoskeletal System
Introduction
Populations affected by large disasters or traumatic events like wars or earthquakes are often fertile ground for unique medical discoveries. During World War II, Nazi Germany bombed London for 57 consecutive days during the beginning of what came to be known as the Blitzkrieg, or eight-month Lightning War. Victims of the Blitz, as it is known in London, included those afflicted with a specific set of symptoms: pain and swelling with accompanying effects of depleted blood volume (shock, weakness, low blood pressure, and decreased urine output). Less obvious was acute kidney failure, which could lead quickly to death if left untreated.
What caused the Blitz victims to suffer from these symptoms? Extreme physical trauma to muscles—namely, compression—destroys skeletal muscle tissue. This condition is called rhabdomyolysis (rhabdo– refers to striation, myo– to muscle, and –lysis to breakdown).
The products of skeletal muscle dissolution, some of which are toxic, circulate in the blood until they are filtered out. Creatine kinase is one of these products; in fact, rhabdomyolysis is diagnosed with a creatine kinase level five times the normal upper limit. Myoglobin is another. Much like hemoglobin, myoglobin uses heme to carry oxygen. It is not, however, housed within a red blood cell. Thus, an erythrocyte-free urine sample that tests positive for heme points compellingly toward rhabdomyolysis. Myoglobin oxygen reserves are just one of the specialized features of muscles, as we will see in this chapter.
Skeletal muscles are only able to exert an effect on the body by moving bony structures around joints. Bones are more than simply a support structure, however; they also provide protection to internal organs, serve as a storage reserve of calcium and other minerals, and are the site of hematopoiesis. Further, skeletal muscle isn’t the only form of muscle in the body; smooth muscle plays roles in the cardiovascular, respiratory, reproductive, and digestive systems, and cardiac muscle comprises the contractile tissue of the heart. In this chapter, we’ll explore the biology of all of these tissues, completing our tour of systems anatomy and physiology!
11.1 The Muscular System
The muscular system is composed of not only skeletal muscle, but also smooth muscle and cardiac muscle. Skeletal muscle is essential for supporting the body and allowing for movement. The contraction of skeletal muscle also compresses venous structures and helps propel blood through the low-pressure venous system toward the heart, as well as lymph through the lymphatic system. Rapid muscle contraction also leads to shivering, which is important in thermoregulation. Smooth muscle is responsible for involuntary movement, such as the rhythmic contractions of smooth muscle in the digestive system called peristalsis. Smooth muscle also aids in the regulation of blood pressure by constricting and relaxing the vasculature. Cardiac muscle is a special type of muscle that is able to maintain rhythmic contraction of the heart without nervous system input. In this section, we will discuss each type of muscle as well as the physiology of muscles.
TYPES OF MUSCLE
Muscle can be divided into the three different subtypes: skeletal muscle, smooth muscle, and cardiac muscle. Each muscle type performs specific functions, although they share some similarities. All muscle is capable of contraction, which relies on calcium ions. All muscle is innervated, although—as we will see—the part of the nervous system that innervates the muscle and the ability of the muscle to contract without nervous input varies from type to type.
Skeletal Muscle
Skeletal muscle is responsible for voluntary movement and is therefore innervated by the somatic nervous system. Due to the arrangement of actin and myosin into repeating units called sarcomeres, it appears striped or striated when viewed microscopically. Skeletal muscle is multinucleated because it is formed as individual muscle cells fuse in long rods during development.
There are multiple different types of fibers within skeletal muscle. Red fibers, also known as slow-twitch fibers, have high myoglobin content and primarily derive their energy aerobically. Myoglobin is an oxygen carrier that uses iron in a heme group to bind oxygen, imparting a red color. Red fibers also contain many mitochondria to carry out oxidative phosphorylation. White fibers, also known as fast-twitch fibers, contain much less myoglobin. Because there is less myoglobin, and therefore less iron, the color is lighter. These two types of fibers can be mixed in muscles. Muscles that contract slowly, but that can sustain activity (such as the muscles that support posture), contain a predominance of red fibers. Muscles that contract rapidly, but fatigue quickly, contain mostly white fibers.
REAL WORLD
Poultry provides a great example of the difference between red and white fibers. Most muscles of support, such as the thigh, are considered dark meat and contain a high concentration of red fibers. Active muscles, like the pectoral muscles (breast meat), are considered white meat and have a high concentration of white fibers.
Smooth Muscle
Smooth muscle is responsible for involuntary action. Thus, smooth muscle is controlled by the autonomic nervous system. It is found in the respiratory tree, digestive tract, bladder, uterus, blood vessel walls, and many other locations. Smooth muscle cells have a single nucleus located in the center of the cell. Just like skeletal muscle, smooth muscle cells contain actin and myosin, but the fibers are not as well-organized, so striations cannot be seen. Compared to skeletal muscle, smooth muscle is capable of more sustained contractions; a constant state of low-level contraction, as may be seen in the blood vessels, is called tonus. Smooth muscle can actually contract without nervous system input in what is known as myogenic activity. In this case, the muscle cells contract directly in response to stretch or other stimuli.
MCAT EXPERTISE
The MCAT loves to test the fact that both smooth and cardiac muscle exhibit myogenic activity. These muscle cells will respond to nervous input, but do not require external signals to undergo contraction.
Cardiac Muscle
Cardiac muscle has characteristics of both smooth and skeletal muscle types. Cardiac muscle is primarily uninucleated, but cells may contain two nuclei. Like smooth muscle, cardiac muscle is involuntary and innervated by the autonomic nervous system. However, like skeletal muscle, cardiac muscle appears striated.
One of the unique characteristics of cardiac muscle is how each cardiac myocyte communicates. Cardiac muscle cells are connected by intercalated discs, which contain many gap junctions. These gap junctions are connections between the cytoplasm of adjacent cells, allowing for the flow of ions directly between cells. This allows for coordinated muscle cell depolarization and efficient contraction of cardiac muscle.
Cardiac muscle cells are able to define and maintain their own rhythm through myogenic activity. Starting at the sinoatrial (SA) node, depolarization spreads using conduction pathways to the atrioventricular (AV) node. From there, the depolarization spreads to the bundle of His and its branches, and then to the Purkinje fibers. The gap junctions allow for progressive depolarization to spread via ion flow across the gap junctions between cells. The nervous and endocrine systems also play a role in the regulation of cardiac muscle contraction. The vagus nerve provides parasympathetic outflow to the heart and slows the heart rate. Norepinephrine from sympathetic neurons or epinephrine from the adrenal medulla binds to adrenergic receptors in the heart, causing an increased heart rate and greater contractility. One of the ways epinephrine does this is by increasing intracellular calcium levels within cardiac myocytes. Ultimately, cardiac contraction—like that of all types of muscle—relies on calcium.
The main characteristics of each muscle type are summarized in Table 11.1.
|
Skeletal Muscle |
Cardiac Muscle |
Smooth Muscle |
|
Striated |
Striated |
Nonstriated |
|
Voluntary |
Involuntary |
Involuntary |
|
Somatic innervation |
Autonomic innervation |
Autonomic innervation |
|
Many nuclei per cell |
1-2 nuclei per cell |
1 nucleus per cell |
|
Ca2+ required for contraction |
Ca2+ required for contraction |
Ca2+ required for contraction |
|
Table 11.1. Types of Muscle |
||
MICROSCOPIC STRUCTURE OF SKELETAL MUSCLE
Each type of muscle has a specific microscopic structure. However, the MCAT tends to focus on the contractile elements and microscopic structure of skeletal muscle. In order to accurately answer those questions on Test Day, let’s take a moment to discuss skeletal muscle in detail.
The Sarcomere
The sarcomere is the basic contractile unit of skeletal muscle. Sarcomeres are made of thick and thin filaments. The thick filaments are organized bundles of myosin, whereas the thin filaments are made of actin along with two other proteins: troponin and tropomyosin. These proteins help to regulate the interaction between the actin and myosin filaments.
MNEMONIC
To remember which filament is associated with troponin and tropomyosin, remember that actin has a T in it.
Each sarcomere is divided into different lines, zones, and bands, as shown in Figure 11.1. Z-lines define the boundaries of each sarcomere. The M-line runs down the center of the sarcomere, through the middle of the myosin filaments. The I-band is the region containing exclusively thin filaments, whereas the H-zone contains only thick filaments. The A-band contains the thick filaments in their entirety, including any overlap with thin filaments. During contraction, the H-zone, I-band, the distance between Z-lines, and the distance between M-lines all become smaller, whereas the A-band’s size remains constant.
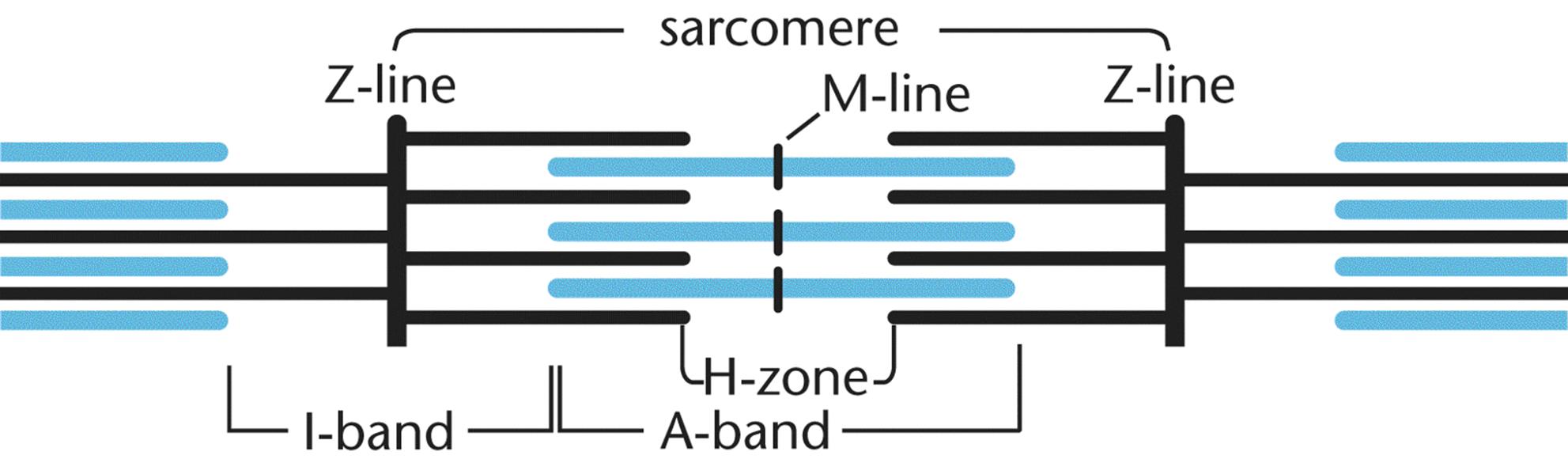 Figure 11.1. The Sarcomere Sarcomeres are the functional units of striated muscle.
Figure 11.1. The Sarcomere Sarcomeres are the functional units of striated muscle.
MNEMONIC
To remember which is the thin and thick filament, remember acthin: actin filaments are thin (while myosin filaments are thick).
MNEMONIC
Parts of the sarcomere:
· Z—Z is the end of the alphabet, and the end of the sarcomere
· M—in the middle of the myosin filaments
· I—I is a thin letter (thin filaments only)
· H—H is a thick letter (thick filaments only)
· A—all of the thick filament, whether or not it is overlapping
Gross Structure of Myocytes
Sarcomeres are attached end-to-end to form myofibrils. Myofibrils are surrounded by a covering known as the sarcoplasmic reticulum (SR), a modified endoplasmic reticulum that contains a high concentration of Ca2+ ions. The sarcoplasm is a modified cytoplasm located just outside the sarcoplasmic reticulum. The cell membrane of a myocyte is known as the sarcolemma. The sarcolemma is capable of propagating an action potential and can distribute the action potential to all sarcomeres in a muscle using a system of transverse tubules (T-tubules) that are oriented perpendicularly to the myofibrils, as shown in Figure 11.2. Each myocyte, or muscle cell, contains many myofibrils arranged in parallel and can also be called a muscle fiber. The nuclei, of which there are many, are usually found at the periphery of the cell. Finally, many myocytes in parallel form a muscle.
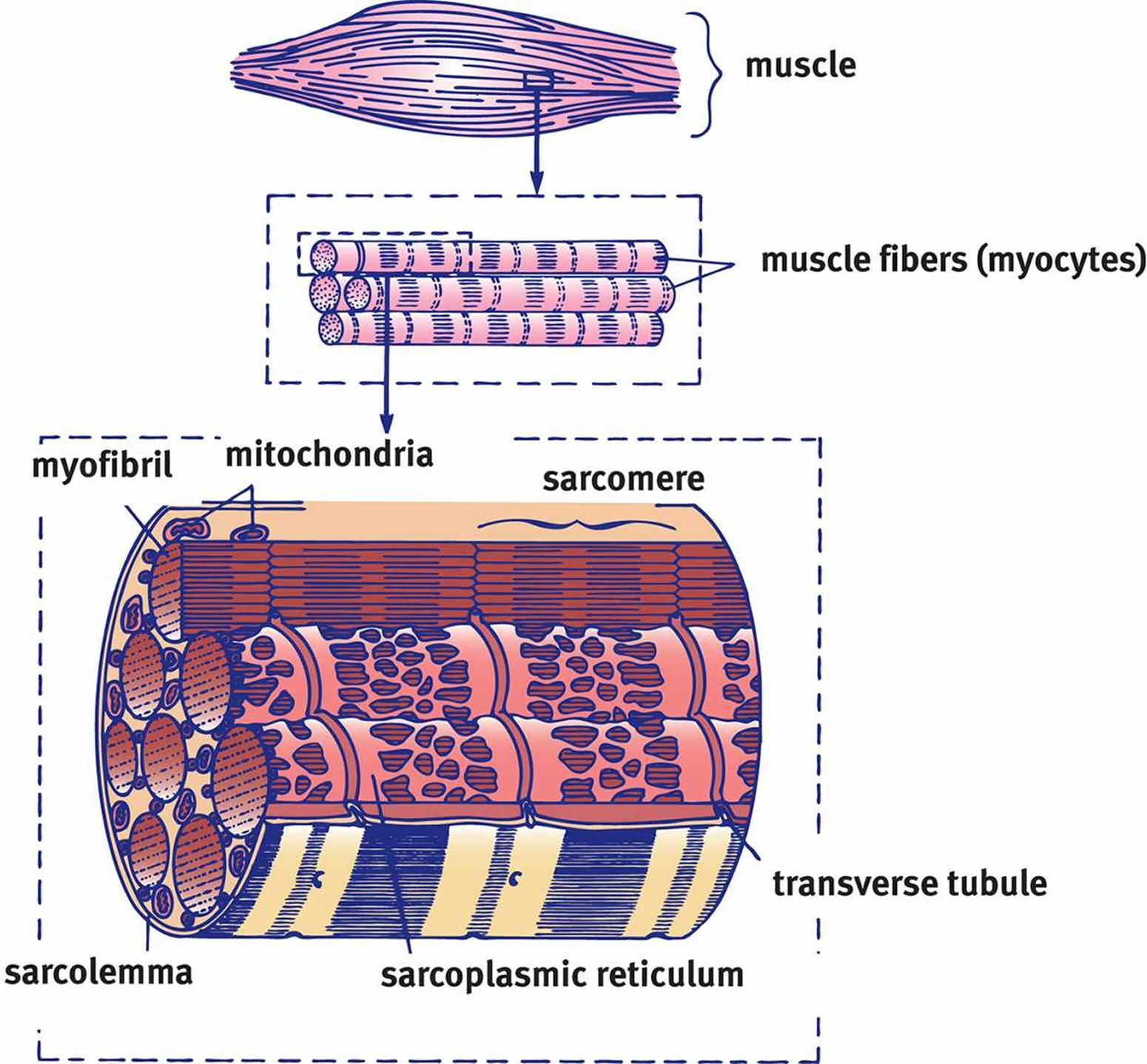 Figure 11.2. Architecture of Skeletal Muscle A muscle is composed of parallel myocytes (muscle fibers), which are composed of parallel myofibrils.
Figure 11.2. Architecture of Skeletal Muscle A muscle is composed of parallel myocytes (muscle fibers), which are composed of parallel myofibrils.
KEY CONCEPT
The sarcoplasmic reticulum is just a fancy name for the specialized endoplasmic reticulum in muscle cells.
KEY CONCEPT
A myofibril is an arrangement of many sarcomeres in series. A muscle fiber (or myocyte, or muscle cell) contains many myofibrils within it, arranged in parallel. A muscle is made up of parallel muscle fibers. These names are very similar; pay careful attention to terminology when reading about muscle structure!
MUSCLE CONTRACTION
Contraction of muscle requires a series of coordinated steps that are repeated to induce further shortening. This process depends on both ATP and calcium.
Initiation
Contraction starts at the neuromuscular junction, where the nervous system communicates with muscles via motor (efferent) neurons. This signal travels down the neuron until it reaches the nerve terminal (synaptic bouton), where acetylcholine is released into the synapse. Acetylcholine binds to receptors on the sarcolemma, causing depolarization. Each nerve terminal controls a group of myocytes; together, the nerve terminal and its myocytes constitute a motor unit.
Depolarization triggers an action potential, which spreads down the sarcolemma to the T-tubules. The T-tubules travel into the muscle tissues to the sarcoplasmic reticulum. When the action potential reaches the sarcoplasmic reticulum, Ca2+ is ultimately released. The calcium ions bind to a regulatory subunit in troponin, triggering a change in the confirmation of tropomyosin, to which troponin is bound. This change exposes the myosin-binding sites on the actin thin filament, as shown in Figure 11.3.
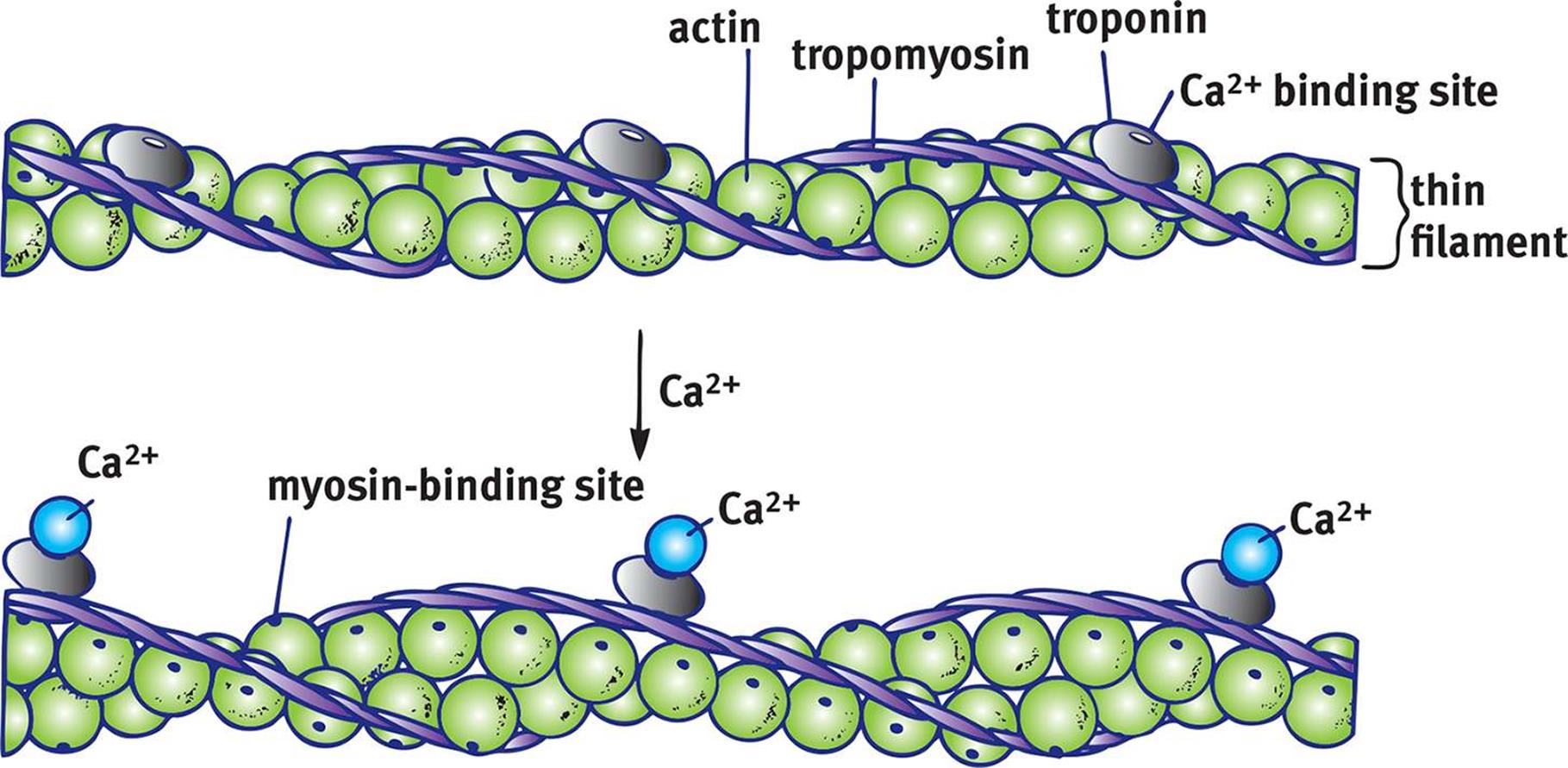 Figure 11.3. Regulation of Contraction with Calcium Calcium binds to troponin, leading to a conformational change in tropomyosin, which exposes the myosin-binding sites of actin.
Figure 11.3. Regulation of Contraction with Calcium Calcium binds to troponin, leading to a conformational change in tropomyosin, which exposes the myosin-binding sites of actin.
Shortening of the Sarcomere
The free globular heads of the myosin molecules move toward and bind with the exposed sites on actin. The newly formed actin–myosin cross bridges then allow myosin to pull on actin, which draws the thin filaments toward the M-line, resulting in shortening of the sarcomere. The actin–myosin cross-bridge cycle is illustrated in Figure 11.4.
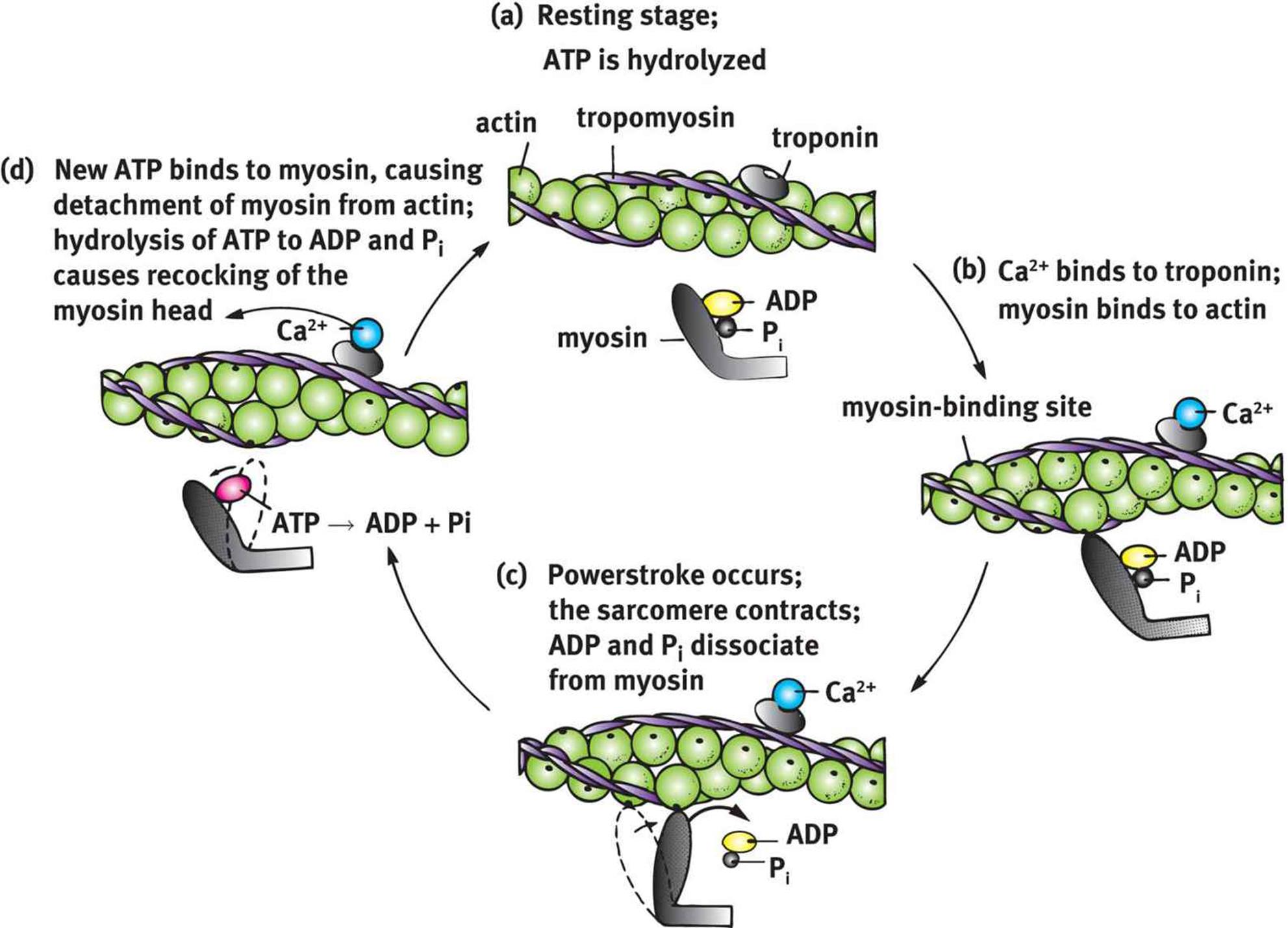 Figure 11.4. The Actin–Myosin Cross-Bridge Cycle Calcium and ATP are essential for muscle contraction and relaxation.
Figure 11.4. The Actin–Myosin Cross-Bridge Cycle Calcium and ATP are essential for muscle contraction and relaxation.
Starting at the top of the diagram, myosin carrying hydrolyzed ATP (ADP and an inorganic phosphate, Pi) is able to bind with the myosin-binding site. The release of the inorganic phosphate and ADP in rapid succession provides the energy for the powerstroke and results in sliding of the actin filament over the myosin filament. Then, ATP binds to the myosin head, releasing it from actin. This ATP is hydrolyzed to ADP and Pi, which recocks the myosin head so that it is in position to initiate another cross-bridge cycle. The repetitive binding and releasing of myosin heads on actin filaments allows for the thin filament to slide along the thick filament, causing sequential shortening of the sarcomere. This is known as the sliding filament model, as shown in Figure 11.5.
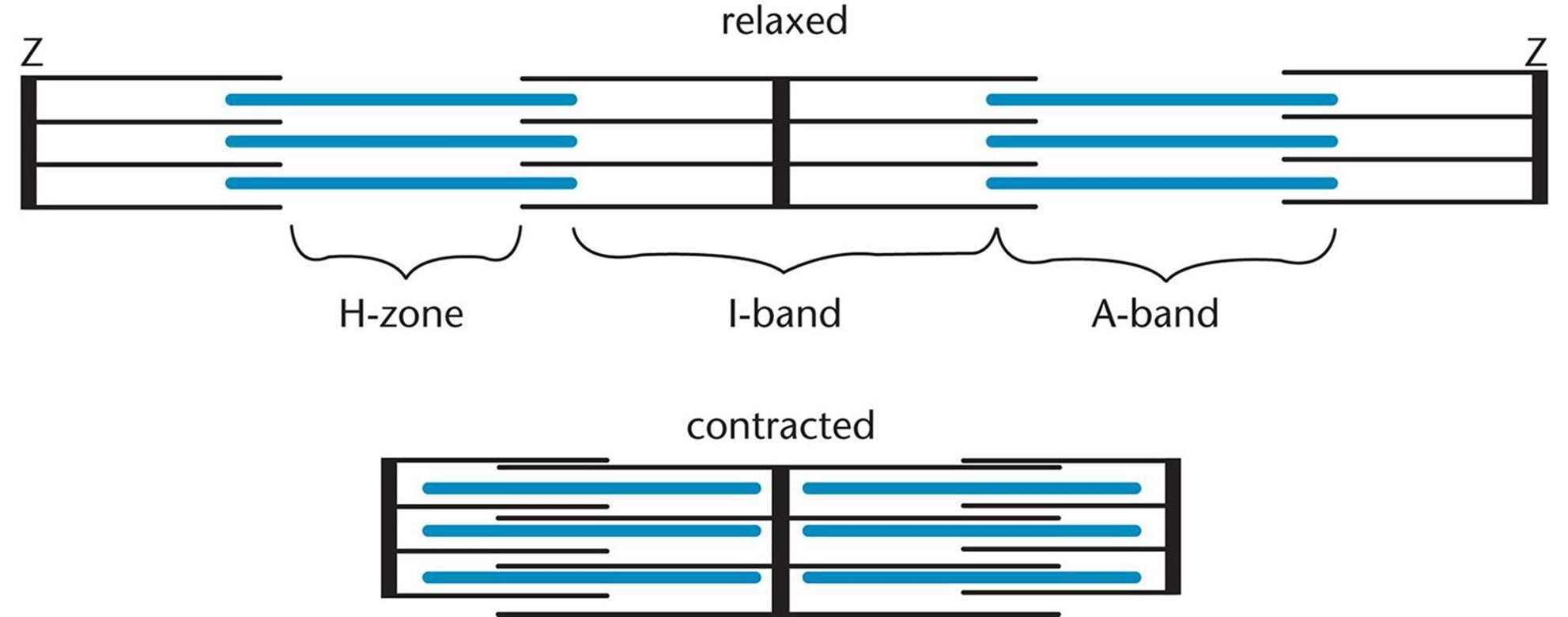 Figure 11.5. Sarcomere Contraction When a sarcomere contracts, both the H-zone and I-band shorten while the A-band is unchanged.
Figure 11.5. Sarcomere Contraction When a sarcomere contracts, both the H-zone and I-band shorten while the A-band is unchanged.
KEY CONCEPT
The binding of ATP is required for releasing the myosin head from the actin filament. It is the dissociation of ADP and Pi from myosin that is responsible for the powerstroke, not the binding of ATP.
Relaxation
Acetylcholine is degraded in the synapse by the enzyme known as acetylcholinesterase. This results in termination of the signal at the neuromuscular junction and allows the sarcolemma to repolarize. As the signal decays, calcium release ceases, and the SR takes up calcium from the sarcoplasm. The SR tightly controls intracellular calcium concentrations so that muscles are contracted only when necessary. ATP binds to the myosin heads, freeing them from actin. Once the myosin and actin disconnect, the sarcomere can return to its original width. Without calcium, the myosin-binding sites will be covered by tropomyosin and contraction will be prevented.
REAL WORLD
After death, ATP production ceases. Myosin heads cannot detach from actin, making it impossible for muscles to relax and lengthen. This condition is known as rigor mortis.
STIMULATION, SUMMATION, AND MUSCLE FATIGUE
Muscle cells, like neurons, exhibit an all-or-nothing response; either they respond completely to a stimulus or not at all. For muscle cells to respond, stimuli must reach a threshold value. The strength of a response from one muscle cell cannot be changed because the only options are all or nothing. Rather, nerves control overall force by the number of motor units they recruit to respond. Maximal response occurs when all fibers within a muscle are stimulated to contract simultaneously.
BRIDGE
Why do muscle fibers contract in an all-or-nothing fashion? Because they are innervated by neurons that deliver signals using action potentials, which are all-or-nothing phenomena as well. Action potentials are discussed in Chapter 4 of MCAT Biology Review.
Simple Twitch
A simple twitch is the response of a single muscle fiber to a brief stimulus at or above threshold, as shown in Figure 11.6a. It consists of a latent period, contraction period, and relaxation period. The latent period is the time between reaching threshold and the onset of contraction. It is during this time that the action potential spreads along the muscle and allows for calcium to be released from the sarcoplasmic reticulum. The muscle then contracts, and, assuming calcium is cleared from the sarcoplasm, it then relaxes.
Summation and Tetanus
If a muscle fiber is exposed to frequent and prolonged stimulation, it will have insufficient time to relax. The contractions will combine, become stronger and more prolonged. This is known as frequency summation, as shown in Figure 11.6b. If the contractions become so frequent that the muscle is unable to relax at all, this is known as tetanus. Prolonged tetanus will result in muscle fatigue, explained below. Note that tetanus (the disease) includes tetanus (the physiological phenomenon) as one of its primary clinical features, but that tetanic physiology also occurs under normal circumstances with multiple simple twitches in succession.
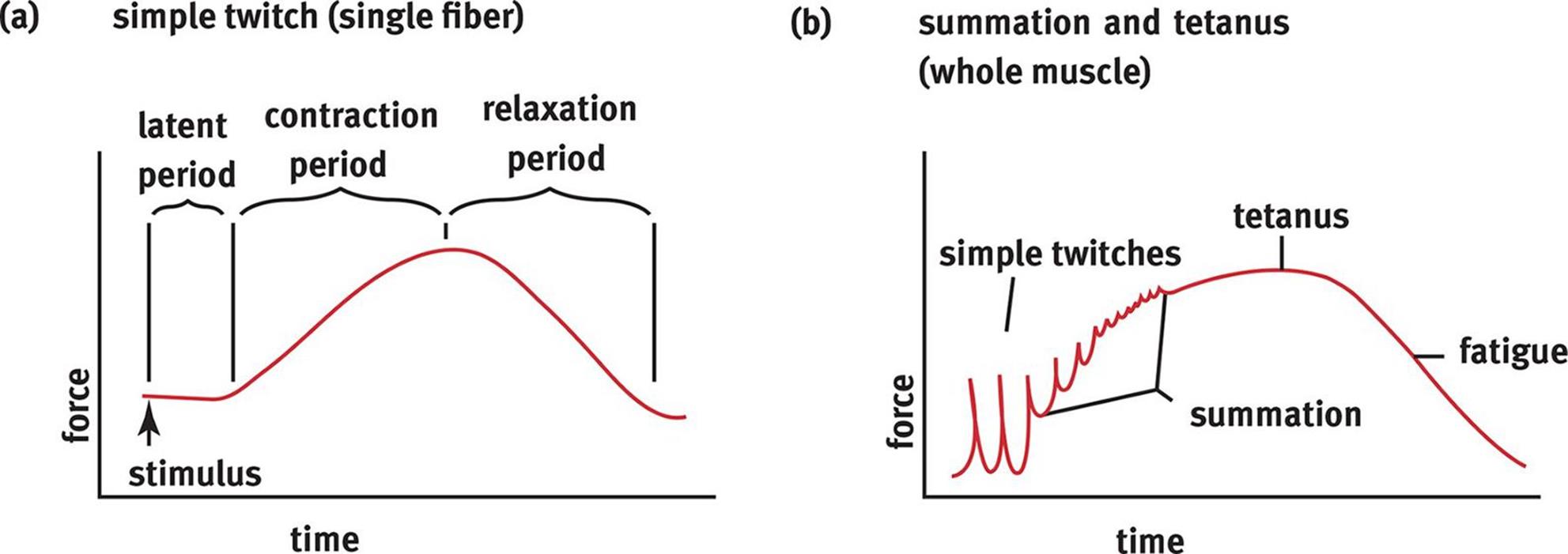 Figure 11.6. Force of Muscle Contraction Due to a Simple Twitch and Tetanus (a) A simple twitch contraction; (b) Summation of frequent simple twitches can lead to tetanus.
Figure 11.6. Force of Muscle Contraction Due to a Simple Twitch and Tetanus (a) A simple twitch contraction; (b) Summation of frequent simple twitches can lead to tetanus.
REAL WORLD
The disease tetanus is caused by a bacterium called Clostridium tetani that releases the toxin tetanospasmin. Tetanospasmin blocks the release of GABA from the neurons that inhibit motor neurons, making the motor neurons overexcitable. This leads to constant contraction of muscles, which can be so strong as to fracture bones. Tetanus can usually be prevented after exposure by administration of a tetanus toxoid vaccine.
Oxygen Debt and Muscle Fatigue
Muscles require ATP to function. Slow-twitch (red) muscle fibers have high levels of mitochondria and thus use oxidative phosphorylation to make ATP. However, this means that high concentrations of oxygen are required to generate the large amounts of ATP muscle cells need. There are two supplemental energy reserves in muscle. Creatine phosphate is created by transferring a phosphate group from ATP to creatine during times of rest. This reaction can then be reversed during muscle use to quickly generate ATP from ADP:
creatine + ATP ⇋ creatine phosphate + ADP
Muscle also contains myoglobin, which binds oxygen with high affinity. As exercising muscles run out of oxygen, they use myoglobin reserves to keep aerobic metabolism going. Fast-twitch (white) muscle fibers have fewer mitochondria and must rely on glycolysis and fermentation to make ATP under most circumstances. When a person exercises, heart rate and respiratory rate increase in order to move more oxygen to actively respiring muscles. The oxyhemoglobin dissociation curve undergoes a right shift in the presence of increased carbon dioxide concentration, increased hydrogen ion concentration (decreased pH), and increased temperature. However, even with these adaptations, muscle use can quickly overwhelm the ability of the body to deliver oxygen. Then, even red muscle fibers must switch to anaerobic metabolism and produce lactic acid, at which point the muscle begins to fatigue. The difference between the amount of oxygen needed by the muscles and the actual amount present is called the oxygen debt. After the cessation of strenuous exercise, the body must metabolize all of the lactic acid it has produced. Most lactic acid is converted back into pyruvate, which can enter the citric acid cycle. This process requires oxygen, and the amount of oxygen required to recover from strenuous exercise is equal to the oxygen debt.
MCAT Concept Check 11.1:
Before you move on, assess your understanding of the material with these questions.
1. What type(s) of muscle (skeletal, smooth, or cardiac) does each of the following describe? (Note: Circle the correct response(s) next to each item.)
|
· Striated: |
Skeletal |
Smooth |
Cardiac |
|
· Always uninucleated: |
Skeletal |
Smooth |
Cardiac |
|
· Always polynucleated: |
Skeletal |
Smooth |
Cardiac |
|
· Voluntary: |
Skeletal |
Smooth |
Cardiac |
|
· Innervated by the autonomic nervous system: |
Skeletal |
Smooth |
Cardiac |
|
· Exhibits myogenic activity: |
Skeletal |
Smooth |
Cardiac |
2. Which zone or band in the sarcomere does NOT change its length during muscle contraction? Why?
3. What are the events that initiate muscle contraction, in order? Start with neurotransmitter release and trace the pathway to the point where myosin binds with actin.
4. What role does the binding of ATP to the myosin head play in the cross-bridge cycle? What about the dissociation of ADP and inorganic phosphate from the myosin head?
· Binding of ATP:
· Dissociation of ADP and inorganic phosphate:
5. What is tetanus (the physiological phenomenon, not the disease)?