Medical Microbiology
Section 4 Clinical manifestation and diagnosis of infections by body system
23 Obstetric and perinatal infections
Introduction
During pregnancy, a novel set of tissues potentially susceptible to infection appear, including the fetus, the placenta and the lactating mammary glands. The placenta acts as an effective barrier, protecting the fetus from most circulating microorganisms, and the fetal membranes shield the fetus from microorganisms in the genital tract. Perforation of the amniotic sac, for instance, at a late stage of pregnancy, often results in fetal infection.
During pregnancy, certain infections in the mother can be more severe than usual (malaria, hepatitis) or latent viruses such as herpes simplex virus (HSV) and cytomegalovirus (CMV) can reactivate and infect the fetus, and after delivery the raw uterine tissue is susceptible to streptococcal and other pathogens, causing puerperal sepsis.
The fetus, once infected via the placenta, is highly susceptible, but may survive certain pathogens and develop congenital abnormalities; examples include: rubella, CMV, Toxoplasma gondii and Treponema pallidum. Bacteria from the vagina, such as group B streptococci, can cause neonatal septicaemia, meningitis and death, and a birth canal infected with Neisseria gonorrhoeae or Chlamydia trachomatis inoculates the infant to cause neonatal conjunctivitis. Maternal genital HSV infection can cause more serious neonatal disease and is underreported.
Maternal HIV infection often causes abortion, prematurity and low birth weight. In resource-poor countries or where maternal infection is undiagnosed, up to 40% of infants are infected, about one-third in utero and two-thirds perinatally from maternal blood or milk. Maternal blood may also transmit hepatitis B and C viruses, and milk can be a source of human T-cell lymphotropic virus type 1 (HTLV-1) infection.
Here, we describe infections that occur during pregnancy and around the time of birth, and discuss their effects on the mother, the fetus and the neonate.
Infections occurring in pregnancy
Immune and hormonal changes during pregnancy worsen or reactivate certain infections
The fetus may be considered as an immunologically incompatible transplant that must not be rejected by the mother. Reasons for the failure to reject the fetus include:
• the absence or low density of major histocompatibility complex (MHC) antigens on placental cells
• a covering of antigens with blocking antibody
• subtle defects in the maternal immune responses.
A severe or generalized immunosuppression in the mother would be undesirable because it would mean potentially disastrous susceptibility to infectious disease. Certain infections, however, are known to be more severe (Table 23.1), and certain persistent infections reactivate during pregnancy (Table 23.2). The hormonal changes that accompany pregnancy can also increase susceptibility. The picture is further complicated when there is malnutrition, which in itself impairs host defences by weakening immune responses, decreasing metabolic reserves and interfering with the integrity of epithelial surfaces.
Table 23.1 The effect of pregnancy on the severity of infectious disease
|
Infection |
Comments |
|
Malaria |
? Depressed cell-mediated immunity |
|
Viral hepatitis |
The viral load may fluctuate due to immunomodulation in pregnancy |
|
Influenza |
Higher mortality during pandemics |
|
Poliomyelitis |
Paralysis more common |
|
Urinary tract infection |
Cystitis; pyelonephritis more common; atony of bladder and ureter leads to less effective flushing, emptying |
|
Candidiasis |
Vulvovaginitis |
|
Listeriosis |
Influenza-like illness |
|
Coccidioidomycosis |
Leading cause of maternal mortality in endemic areas in SW USA and Latin-America |
Table 23.2 Reactivation of persistent infections during pregnancy
|
Infection |
Phenomenon |
|
Cytomegalovirus |
Increased shedding from cervix, virus in milk of nursing mother |
|
Herpes simplex virus |
Increased replication in cervical region |
The fetus has poor immune defences
Once the fetus is infected, it is exquisitely susceptible because:
• IgM and IgA antibodies are not produced in significant amounts until the second half of pregnancy.
• There is no IgG antibody synthesis.
• Cell-meditated immune responses are poorly developed or absent, with inadequate production of the necessary cytokines.
Indeed, if the fetus were able to generate a vigorous response to maternal antigens, a troublesome graft-versus-host reaction could be unleashed.
Most microorganisms have sufficient destructive activity to kill the fetus once it is infected, leading to spontaneous abortion or stillbirth. Here, our interests focus on the few microorganisms that are capable of more subtle, non-lethal effects. They overcome the placental barrier by infecting it so that the infection then spreads to the fetus. They can then interfere with fetal development or cause lesions so that a live but damaged baby is born.
Congenital infections
Intrauterine infection may result in death of the fetus or congenital malformations
After primary infection during pregnancy, certain microorganisms enter the blood, establish infection in the placenta, and then invade the fetus. The fetus sometimes dies, leading to abortion, but when the infection is less severe, as in the case of a relatively non-cytopathic virus, or when it is partially controlled by the maternal IgG response, the fetus survives. It may then be born with a congenital infection, often showing malformations or other pathologic changes. The infant is generally small and fails to thrive. It produces specific antibodies, but often, for instance with CMV, fails to generate an adequate virus-specific cell-mediated immune response, remaining infected for a long period. Hence, the lesions may progress after birth. It is a striking feature of these infections that they are generally mild or unnoticed by the mother.
Important causes of congenital infections are shown in Table 23.3. Viruses that induce fetal malformations (i.e. act as teratogens) share certain characteristics with other teratogens such as drugs or radiation (Table 23.4). The fetus tends to show similar responses (e.g. hepatosplenomegaly, encephalitis, eye lesions, low birth weight) to different infectious agents, and the diagnosis is difficult on purely clinical grounds. Most of these infections, HSV, rubella, CMV and syphilis, can also, at times, kill the fetus. They generally follow primary infection of the mother during pregnancy, so their incidence depends upon the proportion of non-immune females of childbearing age.
Table 23.3 Maternal infections that are transmitted to the fetus
|
Microorganism |
Effects |
|
Rubella virus |
Congenital rubella |
|
Cytomegalovirus (CMV) |
Congenital CMV, deafness, mental retardation |
|
Human immunodeficiency virus (HIV) |
Congenital infection, childhood AIDS; about 1 in 5 infants born to infected mothers are infected in uteroa |
|
Varicella-zoster virus (VZV) |
Skin lesions; musculoskeletal, CNS abnormalities when fetus infected before 20 weeks. After later infection childhood zoster a common sequelb |
|
Herpes simplex virus (HSV) |
Neonatal HSV infection, often disseminated. Much higher risk when maternal infection primary rather than recurrent, infection in utero is rare |
|
Hepatitis B virus |
Congenital hepatitis B, persistent infectiona,c |
|
Parvovirus B19 |
After maternal infection 5–10% fetuses lost (abortion, hydrops fetalis) |
|
Treponema pallidum |
Congenital syphilis, classical syndrome |
|
Toxoplasma gondii |
Congenital toxoplasmosis |
|
Listeria monocytogenes |
Congenital listeriosis, pneumonia, septicaemia, meningitisb |
|
Mycobacterium leprae |
Congenital infection common in mothers with lepromatous leprosy |
Congenitally infected babies may be symptomless, especially in cytomegalovirus infection. They are often small, fail to thrive or show detectable abnormalities later in childhood. In all cases, the baby remains infected, often for long periods, and may infect others.
a This figure is for resource-poor countries with no intervention (no antiretroviral drugs, no caesarean section, or avoidance of breastfeeding).
b Infection also occurs during and immediately after birth.
c Protection of newborn by hepatitis B vaccine plus specific immunoglobulin.
Table 23.4 Comparison between teratogenic viruses and other teratogens
|
Viral teratogens (e.g. rubella) |
Other teratogens (e.g. drugs, radiation) |
|
|
Critical stages of susceptibility during pregnancy (organogenesis) |
+ |
+ |
|
Fetal death a possible outcome |
+ |
+ |
|
Maternal effects minimal or absent |
+ |
+ |
|
Cause retarded fetal growth |
+ |
+ |
|
Increase in frequency of naturally occurring abnormalities |
− |
+ |
|
Influence of genetic factors in mother/fetus |
− |
+ |
Routine antenatal screening for rubella antibody, treponemal antibody (which includes syphilis, yaws, pinta or bejel, which cannot be identified individually by serology), hepatitis B surface antigen and HIV antibody is being carried out to differing degrees worldwide. These tests help identify women who are infected with hepatitis B or HIV, infected or have been exposed in the past to treponemal infections, the most important of which is syphilis in this setting, or are susceptible to rubella.
Routine screening programmes lead to clinical management issues for both the mother and child. For example, HIV diagnosis will lead to consideration of antiretroviral therapy for the mother and, immediately on birth, the child, offering a caesarean section delivery, and advising against breastfeeding to reduce the risk of vertical transmission. In addition, the child will then be followed up for at least 12 months using sensitive tests to determine whether HIV has been transmitted vertically. Diagnosis of chronic hepatitis B infection will result in determination of the maternal level of infectivity, and subsequently offering an accelerated course of hepatitis B vaccine alone or, if the mother is highly infectious, vaccine and HBV-specific immunoglobulin to the baby. In addition, there are antiviral drugs for chronic hepatitis B that might be offered, together with long-term follow-up, to the mother. Rubella-susceptible women are offered rubella immunization postnatally. Women found to have been exposed to treponemal infection in pregnancy are offered antibiotic treatment and the baby is followed up for the first year using serology to identify active infection, as congenital syphilis can result from earlier untreated infection of the mother. In the case of CMV, which is not part of routine antenatal screening in the UK and USA, for example, a primary infection, reinfection or reactivation of the latent virus during pregnancy can lead to fetal infection (see next section).
The likelihood of fetal infection is increased when the mother develops a poor immune response, when the concentration of infectious agents in her blood is high (primary or secondary syphilis, e antigen positive hepatitis B carrier, HIV), or in a primary infection.
There is no good evidence to suggest that maternal mumps, influenza or poliovirus infection during pregnancy leads to harmful effects in the fetus, but the human parvovirus (see Ch. 26) occasionally causes fetal damage or death in 5–10% of cases following maternal infection in early pregnancy. The infected fetus develops severe anaemia with ascites and hepatosplenomegaly (hydrops fetalis) as the virus infects progenitor erythroid stem cells. Intrauterine exchange blood transfusion is used to manage hydrops fetalis.
Congenital rubella
The fetus is particularly susceptible to rubella infection when maternal infection occurs during the first 3 months of pregnancy
At this time, the heart, brain, eyes and ears are being formed and the infecting virus interferes with their development. If the fetus survives, it may show certain abnormalities (Fig. 23.1). Not all fetuses are affected; in one study, detectable congenital defects were seen in 15% of cases when maternal rubella occurred in the first month of pregnancy, 25% in the second month, 18% in the third month and 7% in the fourth month. The figure for the first month is relatively low because fetal death is a common sequel at this stage.
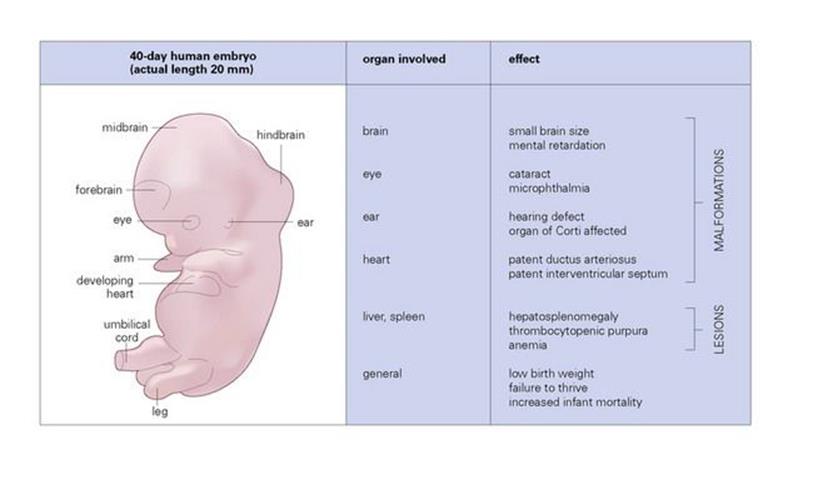
Figure 23.1 Organ involvement and effects in congenital rubella.
Congenital rubella can affect the eye, heart, brain and ear
Clinical manifestations of congenital rubella include low birth weight and eye (Fig. 23.2) and heart lesions. Effects on the brain and ears may not become detectable until later in childhood, in the form of mental retardation and deafness. Up to 80% of infected infants eventually suffer from deafness. About 25% of congenitally infected children develop insulin-dependent diabetes mellitus later in life (the virus replicates in the pancreas), but rubella is a very uncommon cause of this disease. There is 15% mortality in infants showing signs of infection at birth, often associated with hypogammaglobulinaemia.
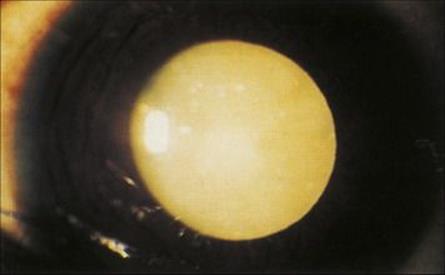
Figure 23.2 Cataract in congenital rubella.
(Courtesy of R.J. Marsh and S. Ford.)
Fetal rubella IgM is found in cord and infant blood
Infected fetuses produce their own IgM antibody to rubella virus, which can be detected in cord and infant blood. Maternal IgG antibodies are also present and together with interferons help control the spread of infection in the fetus. Virus can be isolated from the infant’s throat or urine. The infant sheds virus into the throat and urine for several months and can infect susceptible individuals. Rubella virus RNA detection may be carried out in specific centres in order to assist with the diagnosis.
Congenital rubella can be prevented by vaccination
Vaccination with live attenuated rubella virus is given during childhood, usually with the combined MMR (mumps, measles and rubella) vaccine (see Ch. 34). Pregnancy is a contraindication to vaccination, as it is a live vaccine, and the only safe time during reproductive life is the immediate postpartum period. This is an interesting example of a vaccine that is given to protect an as yet non-existent individual (the future fetus), the infection being only subclinical or mild in the mother. Until effective vaccines became available in the late 1960s (Box 23.1), rubella was an important cause of congenital heart disease, deafness, blindness and mental retardation. The virus continues to circulate in the community and damage fetuses in countries with less extensive rubella vaccination programmes.
![]()
Box 23.1  Lessons in Microbiology
Lessons in Microbiology
Rubella and the fetus
Dr Norman McAllister Gregg (1892–1966) was ophthalmic surgeon to the Royal Alexandra Hospital for Children in Sydney, and during the Second World War, he noticed what he called an ‘epidemic’ of congenital cataract in infants. He went further and made the astute observation that all the mothers had suffered from rubella during early pregnancy. There were 78 infants with cataract, and 68 of the mothers had a history of rubella in early pregnancy. Many of the infants had heart defects, were small, and two-thirds of them had microphthalmia. He published his findings in 1941, providing the first clear demonstration that an environmental factor could cause congenital malformations. It is a striking feature of the infection that, whereas the fetus suffers cruel malformations, the mother shows little or no signs of illness. We now know that several other viruses, notably CMV, can do this, as well as factors such as thalidomide and folate deficiency. Later studies on rubella revealed that congenitally infected infants also developed deafness and brain defects. Survivors were followed up until 1991 when they were 50, and other abnormalities have been observed, including the development of diabetes by the age of 25 years and certain vascular abnormalities.
It was not until 1962 that the causative virus was isolated and grown in cell culture. A rubella epidemic in the USA in 1964–1965 left in its wake 20 000 infants with the congenital rubella syndrome. By the late 1960s, an effective live virus vaccine was available, and congenital rubella is now seen only when vaccination cover is poor. The fetus is exquisitely vulnerable to rubella during the first trimester of pregnancy. This is the critical stage in embryonic development when key organs (heart, ear, eye, brain) are being formed, and although the virus does no damage to the cells in which it grows, it interferes with mitosis. Interference with programmed mitosis in these major organs causes the malformations, vasculitis playing a part. The fetus is good at repairing damage but it cannot at a later stage compensate for the failure in basic organ development. The antimitotic action of the virus also means that the total number of cells in the body is reduced, and this is why the rubella-infected infants are smaller. The rubella virus remains in infected organs such as the lens and brain for more than 1 year, but eventually there is an adequate cell-mediated immune response and the virus is eliminated.
![]()
Congenital CMV infection
Mothers with a poor T-cell proliferative response to CMV antigens are more likely to infect their fetus
After primary maternal infection during pregnancy, about 40% of fetuses are infected, and 5% of these show signs at birth. It is not known whether the fetus is especially vulnerable at certain stages of pregnancy. The fetus is also infected following CMV reactivation during pregnancy in women with previous CMV exposure, but fetal damage is then uncommon. As many as 1–2% of infants born in the USA are infected, and up to about 10% of these are symptomatic, with up to 1 million infectious doses of virus present per millilitre of urine. However, the incidence of congenital CMV infection is likely to be an underestimate worldwide. In large cohorts of pregnant women studied it has been shown that 2% develop a primary CMV infection, but over 95% were asymptomatic. Of those women with a primary infection in the first trimester, up to 30% of babies may develop central nervous system (CNS) sequelae including sensorineural hearing loss. Although the percentage is much reduced if the maternal infection is later in pregnancy, a degree of CNS damage still occurs. However, the relationship between a first trimester infection and outcome is much clearer in rubella infections than with CMV. In CMV reactivation or reinfection, partial control of the infection by maternal antibody under these circumstances means that the baby may be infected but not affected, although a small percentage become symptomatic over the next couple of years. The frequency and outcome of congenital CMV infections in reactivation or reinfection in pregnancy is still not well understood. However, the incidence of symptomatic congenital CMV infections has been reported to be similar in pregnant women with primary infections and reactivations or reinfections.
Clinical features of congenital CMV include mental retardation, choroidoretinitis and optic atrophy, hearing defects, hepatosplenomegaly, thrombocytopenic purpura and anaemia (Fig. 23.3). Deafness and mental retardation may not be detectable until later in childhood.

Figure 23.3 Microcephaly with associated severe psychomotor retardation and hepatosplenomegaly in congenital cytomegalovirus infection.
(Courtesy of W.E. Farrar.)
Diagnosis is by detecting CMV-specific IgM antibodies in infant blood within 3 weeks of delivery, and by detecting and quantifying CMV DNA in the blood or urine during this period. Virus can also be isolated from throat swab or urine samples. Live attenuated vaccines have been investigated (AD169 and Towne strains), and in preliminary studies no-one who became pregnant after vaccination transmitted the virus to the infant.
Antiviral drugs such as ganciclovir and valganciclovir can be considered in managing symptomatic babies with congenital CMV infection.
Congenital syphilis
As a result of routine serologic screening for syphilis in antenatal clinics and treatment with penicillin (see Ch. 21), congenital syphilis is now rare, but is more common in resource-poor countries. Clinical features in the infant include rhinitis (snuffles), skin and mucosal lesions, hepatosplenomegaly, lymphadenopathy, and abnormalities of bones, teeth and cartilage (saddle-shaped nose). Pregnancy often masks the early signs of syphilis, but the mother will have serological evidence of treponemal infection, and treponemal IgM will be detected in the fetal blood. Vertical transmission most commonly takes place after 4 months of gestation; therefore treatment of the mother before the fourth month of pregnancy should prevent fetal infection.
Congenital toxoplasmosis
Acute asymptomatic infection by Toxoplasma gondii during pregnancy can cause fetal malformation
Approximately 35% of healthy adults have serological evidence of previous Toxoplasma gondii infection. Clinical features of congenital toxoplasmosis in the infant include convulsions, microcephaly, chorioretinitis, hepatosplenomegaly and jaundice, with later hydrocephaly, mental retardation and defective vision (see Ch. 25). There are often no detectable abnormalities at birth, but signs (e.g. chorioretinitis; see Fig. 25.5) generally appear within a few years. The incidence of fetal infection and damage (leading to abortion, stillbirth or disease in the newborn) increases from 14% when maternal infection is in the first trimester to 59% when in the third trimester. Damage is more severe the earlier in pregnancy infection is contracted.
Toxoplasma-specific IgM antibodies may be detected in cord blood. Treatment of a pregnant woman or an infected infant is with spiramycin or (with care to avoid toxicity) sulphadiazine plus pyrimethamine plus folinic acid.
There is no vaccine. Prevention is by avoidance of primary infection which occurs via ingesting cysts from cat faeces or lightly cooked meat during pregnancy.
Congenital HIV infection
In resource-poor countries, approximately one-quarter of infants born to mothers with HIV are infected: about one-third of these in utero and the rest perinatally
Clinically, congenital HIV infection manifests as poor weight gain, susceptibility to sepsis, developmental delays, lymphocytic pneumonitis, oral thrush, enlarged lymph nodes, hepatosplenomegaly, diarrhea and pneumonia, and some infants develop encephalopathy and AIDS by 1 year of age. Since most infections take place during late pregnancy or during delivery, transmission rates are reduced by lowering the HIV load by offering antiretroviral drugs during pregnancy, especially during the last trimester or during labour, carrying out an elective caesarean section, and avoiding breastfeeding.
IgG antibodies present in the neonatal blood sample may be maternal in origin and can persist for at least 1 year. The mainstay of laboratory diagnosis therefore involves detection of HIV-1 proviral DNA or HIV-1 RNA by polymerase chain reaction (PCR), although these tests may not be positive until several months after birth, in conjunction with HIV antibody and antigen detection using the combination assay.
Congenital and neonatal listeriosis
Maternal exposure to animals or foods infected with Listeria can lead to fetal death or malformations
Listeria monocytogenes is a small Gram-positive rod, which is motile and beta-haemolytic. It is distributed worldwide in a great variety of animals including cattle, pigs, rodents and birds, and the bacteria occur in plants and in soil. Listeria can grow at regular refrigeration temperatures (e.g. 3–4 C). Transmission to humans is by:
• contact with infected animals and their faeces
• consumption of unpasteurized milk or soft cheeses or contaminated vegetables.
In the USA, there are about 2000 reported cases of listeriosis each year; about one-third of them in newborn infants. Faecal carriage is uncommon, except in contacts of cases.
L. monocytogenes in the pregnant woman causes a mild influenza-like illness or is asymptomatic, but there is a bacteraemia which leads to infection of the placenta and then the fetus. This may cause abortion, premature delivery, neonatal septicaemia or pneumonia with abscesses or granulomas. The infant can also be infected shortly after birth, for instance, from other babies or from hospital staff, and this may lead to a meningitic illness.
L. monocytogenes is isolated from blood cultures, cerebrospinal fluid (CSF) or newborn skin lesions.
Treatment is with ampicillin, which may need to be combined with gentamicin to achieve a bactericidal effect. There are no vaccines.
Pregnant women should avoid exposure to infected material, but the exact source of infection is generally unknown.
Infections occurring around the time of birth
Effects on the fetus and neonate
The routes of infection in the fetus and neonate are shown in Figure 23.4
Viral infections (e.g. rubella, CMV) are generally less damaging to the fetus when the maternal infection occurs late in pregnancy. Primary infection with varicella-zoster virus (VZV) in the first 20 weeks of pregnancy can lead to limb deformities and other severe lesions in the newborn. HSV infection in this setting is underdiagnosed and can lead to neonatal morbidity and mortality.
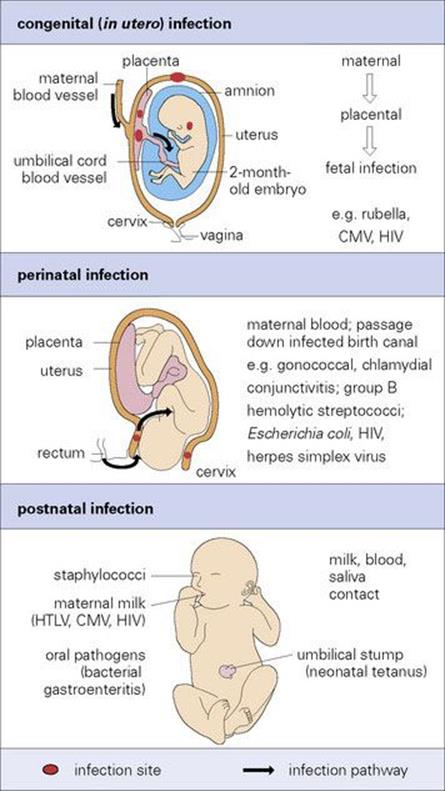
Figure 23.4 Routes of infection in the fetus and neonate. CMV, cytomegalovirus; HIV, human immunodeficiency virus; HTLV, human T-cell lymphotropic virus.
Bacterial infections originating from the vagina and perineum late in pregnancy, especially those occurring when the fetal membranes have been ruptured for more than 1–2 days, may result in chorioamnionitis, maternal fever, premature delivery and stillbirth. Infants of low birth weight (< 1500 g) tend to be more severely affected. Bacteria involved include:
• group B haemolytic streptococci; 10–30% of pregnant women are colonized in the rectum or vagina
• E. coli
• Klebsiella
• Proteus
• Bacteroides
• staphylococci
• Mycoplasma hominis.
These infections may also be acquired after delivery to give later-onset disease.
Neonatal septicaemia often progresses to meningitis
Bacterial meningitis (see Table 24.5) is frequently fatal unless treated. Clinical diagnosis is difficult because the infant shows generalized signs such as respiratory distress, poor feeding, diarrhea and vomiting, but early diagnosis is essential and emergency treatment is required. ‘Blind’ antibiotic treatment should be started as soon as cerebrospinal fluid (CSF) (Gram stain and culture) and blood samples have been taken.
Fetal infection with herpes simplex must be considered in a baby who is acutely ill within a few weeks of birth
Fetal infection during labour results from direct contact with the infecting microorganism as the fetus passes down an infected birth canal (Table 23.5). For instance, cutaneous lesions of herpes simplex may develop 1 week after delivery, with generalized infection and severe CNS involvement. Approximately 80% of mothers with primary HSV infection (only about 10% with recurrent HSV) have cervical lesions and about a third of their infants are infected. Babies < 4 weeks of age may present with neonatal HSV as acutely ill and ‘septic’ but classically there are three well-defined clinical presentations. Those with infection affecting the skin, eye and/or mouth (SEM); encephalitis with or without skin involvement; and disseminated disease involving the lungs, liver, central nervous system, adrenal glands and SEM. The diagnosis may be missed as neonatal HSV infection may present without skin lesions in up to 39% of babies. Therefore, there must be a low threshold for considering this diagnosis and acyclovir therapy should be started as soon as possible. Treatment could be started at the same time as samples are collected for HSV DNA detection that include swabs of the SEM and vesicles, if present, EDTA whole blood samples and cerebrospinal fluid. Morbidity and mortality rates are higher in those with encephalitis and disseminated disease.
Table 23.5 Neonatal infections acquired during passage down an infected birth canal
|
Infectious agent |
Site of infection |
Phenomenon |
|
Neisseria gonorrhoeae |
Conjunctiva |
Neonatal conjunctivitis (ophthalmia neonatorum) |
|
Chlamydia trachomatis |
Conjunctiva, respiratory tract |
Neonatal conjunctivitis (ophthalmia neonatorum), neonatal pneumonia |
|
Herpes simplex virus |
Skin, eye, mouth |
Neonatal herpetic infectiona |
|
Genital papillomavirus |
Respiratory tract |
Laryngeal warts in young children |
|
Group B streptococcib, Gram-negative bacilli (E. coli etc.) |
Respiratory tract |
Septicaemia; death if not treated |
|
Candida albicans |
Oral cavity |
Neonatal oral thrush |
a Although preventable by caesarean section, it is often difficult to detect maternal genital infection; infants can be treated prophylactically with acyclovir.
b Up to 30% of women carry these bacteria in the vagina or rectum.
Gonococci (Fig. 23.5), chlamydia or staphylococci (see Ch. 25) can infect the eye to cause ophthalmia neonatorum. Infection with group B streptococci generally occurs at this time.

Figure 23.5 Gonococcal ophthalmia neonatorum. Signs appear 2–5 days after birth. The inflammation and oedema are more severe than with chlamydia infection.
(Courtesy of J.S. Bingham.)
In countries with high hepatitis B carrier rates, maternal blood is a major source of infection during or shortly after birth. More than 90% of infants from carrier mothers become infected and then carry the virus. This is preventable by giving the vaccine plus specific immunoglobulin to the newborn. Hepatitis C, in contrast, is not usually transmitted in this way, and < 5% of children with carrier mothers are infected.
Human milk may contain rubella virus, CMV, human T-cell lymphotropic virus (HTLV) and HIV. The amount of virus detectable in milk is low and, except in the case of HTLV and HIV, milk is not thought to be an important source of infection. However, it makes sense to pasteurize milk in human milk banks, just as we pasteurize cows’ milk.
Effects on the mother
Puerperal sepsis is prevented by aseptic techniques
After delivery (or abortion), a large area of damaged vulnerable uterine tissue is exposed to infection. Puerperal sepsis (childbed fever) was a major cause of maternal death in Europe in the nineteenth century. In 1843, Oliver Wendell Holmes made the unpopular suggestion that it was carried on the hands of doctors, and 4 years later, Ignaz Semmelweiss in Vienna showed how it could be prevented if doctors and midwives washed their hands before attending a woman in labour and practiced aseptic techniques. This is because:
• Group A beta-haemolytic streptococci were the major culprits and came from the nose, throat or skin of hospital attendants.
• Other possible organisms include anaerobes such as Clostridium perfringens or Bacteroides, E. coli and group B streptococci and originate from the mother’s own faecal flora.
Puerperal sepsis carried a mortality rate of up to 10% until the 1930s, but, like septic abortion, is now uncommon in resource-rich countries. Predisposing factors include premature rupture of the membranes, instrumentation and retained fragments of membrane or placenta. High vaginal swabs and blood cultures should be taken if there is postnatal pyrexia or an offensive discharge.
Other neonatal infections
Infection may be transmitted to the newborn infant during the first 1–2 weeks after birth, rather than during delivery as follows:
• Group B beta-haemolytic streptococci and Gram-negative bacilli (see above) acquired by cross-infection in the nursery can still cause serious infection at this time, often with meningitis (see Ch. 24).
• Herpes simplex virus from cold sores or herpetic whitlows of attending adults.
• Staphylococci from the noses and fingers of adult carriers may cause staphylococcal conjunctivitis or ‘sticky eye’ (see Ch. 25), skin sepsis in the neonate, and sometimes the staphylococcal ‘scalded skin’ syndrome (Fig. 23.6) due to a specific ‘epidermolytic’ staphylococcal toxin.

Figure 23.6 Staphylococcal scalded skin syndrome. There are large areas of epidermal loss where bullae have burst.
(Courtesy of L. Brown.)
During the first 1–2 weeks of life, the nose of the neonate becomes colonized with Staphylococcus aureus, which can enter the nipple during feeding to cause a breast abscess. These infections are preventable if hospital staff pay vigorous attention to handwashing and aseptic techniques.
If hygienic practices are poor, the umbilical stump, especially in resource-poor countries, may be infected with Clostridium tetani, usually because instruments used to cut the cord are contaminated with bacterial spores, resulting in neonatal tetanus (Fig. 23.7). It can be prevented by immunizing mothers with tetanus toxoid.

Figure 23.7 Tetanus. Risus sardonicus in a newborn infant.
(Courtesy of W.E. Farrar.)
In resource-poor countries, gastroenteritis is an important problem during the neonatal period as well as during infancy.
Diarrhea leading to water and electrolyte depletion is particularly serious in low birth weight infants. Causative agents include strains of E. coli and salmonellae rather than rotaviruses (Ch. 22). Breastfeeding gives some protection by supplying specific antibodies and other less well-characterized protective factors.
![]()
 Key Facts
Key Facts
• During pregnancy, certain infections (coccidioidomycosis, influenza) can be more severe than usual, and there can be reactivation of certain persistent infections (HSV, CMV).
• A few infections are able to pass to the fetus via the placenta and cause damage. These infections are generally mild or subclinical in the mother (rubella, CMV, toxoplasmosis), but this is not always the case (syphilis).
• Once infected, the fetus may die, but if the baby survives it may be born with the infection (HIV, toxoplasmosis), often showing characteristic malformations (rubella, syphilis).
• Infection of the infant during birth or shortly afterwards can cause local disease (conjunctivitis due to gonococci or chlamydia) or occasionally severe life-threatening illness (E. coli meningitis, herpes simplex virus or group B streptococcal infection).
• Life-threatening bacterial infection of the mother via the postpartum uterus (puerperal sepsis) used to be common but is now rare in resource-rich countries.
![]()