Medical Microbiology
Section 4 Clinical manifestation and diagnosis of infections by body system
25 Infections of the eye
Introduction
Because the outer surface of the eye is exposed to the external world, it is easily accessible to infective organisms. The conjunctiva is particularly susceptible. Not only is it a vulnerable epithelial surface, it is covered by the eyelids, which create a warm, moist, enclosed environment in which contaminating organisms can quickly establish and set up a focus of infection. The eyelids and tears protect the external surfaces of the eye, both mechanically and biologically; any interference with their function increases the chance of a pathogen becoming established.
Eyelid infections are generally due to Staphylococcus aureus, with involvement of the lid margins, causing blepharitis, and eyelid glands or follicles causing styes or hordeolums.
The conjunctiva can be invaded by other routes, such as the blood or nervous system. The deeper tissues of the eye can also be invaded from within, particularly by protozoan and worm parasites. Differentiating between the different causes of conjunctivitis on the basis of clinical signs and symptoms can be difficult.
Conjunctivitis
A wide variety of viruses and bacteria can cause conjunctivitis or pinkeye (Table 25.1). Conjunctivitis can start in one eye and then progress to the other. The eye will be red, irritated and there will be a lot of tear fluid. A sticky discharge is likely to be secondary to a bacterial infection. Some infections are common in children and resolve quickly, others are potentially more serious. Keratoconjunctivitis from adenovirus, herpes simplex virus or varicella-zoster virus infection can result in severe damage. An acute haemorrhagic conjunctivitis is highly contagious and outbreaks have been reported around the world. It presents as a pink eye, fast-onset eye pain with tear formation and light sensitivity or photophobia. It can follow infection with enterovirus 70 and coxsackievirus A24.
Table 25.1 Microbial infections of the conjunctiva
|
Organism |
Comments |
|
Adenovirus |
Especially types 3, 7, 8, 19 |
|
Measles virus |
Infection of conjunctiva via blood |
|
Herpes simplex virus |
Virus reactivating in ophthalmic division of trigeminal ganglia causes corneal lesion (dendritic ulcer) |
|
Varicella-zoster virus |
May involve conjunctiva |
|
Enterovirus 70, coxsackievirus A24 |
Acute haemorrhagic conjunctivitis |
|
Chlamydia trachomatis |
Cause of trachoma and commonly blindness |
|
Neisseria gonorrhoeae |
Infection of newborn via birth canal |
|
Staphylococcus aureus |
Cause eyelid infection (styes) and ‘sticky eye’ in neonates |
Chlamydial infections
Different serotypes of Chlamydia trachomatis cause inclusion conjunctivitis and trachoma
To establish infection on the conjunctiva, microorganisms must avoid being rinsed and wiped away in tears. The best way of achieving this is to have a specific mechanism of attachment to conjunctival cells. Chlamydia, for example, has surface molecules that bind specifically to receptors on host cells. This is one of the reasons that, of all the organisms infecting the conjunctiva (Table 25.1), they are among the most successful. There are eight different serotypes of Chlamydia trachomatis responsible for inclusion conjunctivitis (D–K) (Fig. 25.1) and another four serotypes responsible for trachoma (A, B, Ba and C), which, globally, is the most important eye infection in the world.

Figure 25.1 Chlamydial conjunctivitis is the most common form of neonatal conjunctivitis.
(Courtesy of G. Ridgway.)
Eight million people worldwide are visually impaired because of trachoma
Approximately 84 million people worldwide are affected by trachoma. Of these, about 8 million have some degree of visual impairment and the disease accounts for more than 3% of the world’s blindness. Trachoma is endemic in resource-poor countries where prevalence rates in pre-school children can reach 60–90%. Trachoma was known in ancient Egypt 4000 years ago, and tweezers to remove in-turned eyelashes (Fig. 25.2) have been found in royal tombs. Transmission of C. trachomatis is by contact, for example, by contaminated flies, fingers and towels.
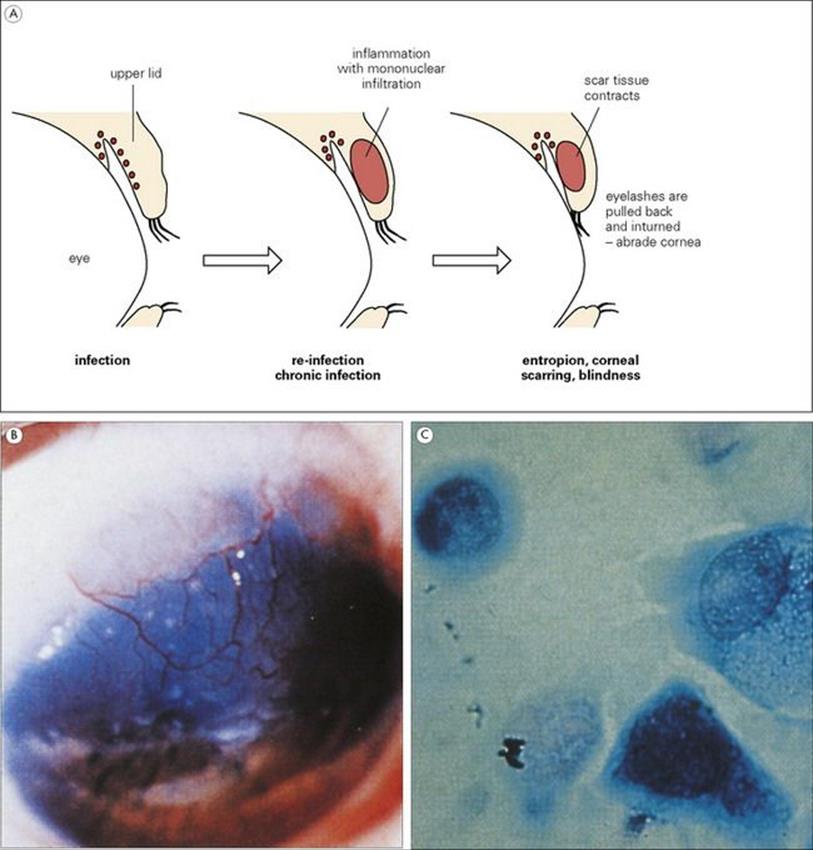
Figure 25.2 Chlamydia trachomatis and blindness. The pathogenesis is outlined in (A). Scarring of the cornea (B) results from long-standing ocular trachoma. (Courtesy of R.C. Barnes.) Giemsa stain of an ocular scraping from trachoma (C) shows C. trachomatis as an intracellular inclusion.
(Courtesy of G. Ridgway.)
Trachoma itself is the result of chronic repeated infections (Fig. 25.2), which are especially prevalent when there is poor access to water, preventing regular washing of the hands and face. Under these circumstances, chlamydial infection is frequently spread from one conjunctiva to another and this can be referred to as ‘ocular promiscuity’, comparable with the spread of genital secretions in non-specific urethritis (see Ch. 21). Some chlamydial serotypes can infect the urogenital tract (see Ch. 21) as well as the conjunctiva, and the conjunctiva or lungs of a newborn infant may become infected after passage down an infected birth canal (see Ch. 23). In this situation, systemic treatment with erythromycin is generally needed.
Chlamydial infections are treated with antibiotic and prevented by face washing
Laboratory diagnosis of chlamydial infections (see Chs. 21 and 32) can be carried out using conjunctival fluid or scrapings. Point-of-care tests for rapid diagnosis in the field are available but there are issues regarding sensitivity. Treatment is with topical or oral antibiotics (e.g. azithromycin, doxycycline, etc.). Because infection and reinfection are facilitated by overcrowding, shortage of water and abundant fly populations, the disease can be prevented by improvements in standards of hygiene. In many areas with high rates of endemic trachoma, disease leading to blindness has been sharply reduced or eliminated by socioeconomic development and specific intervention steps (e.g. face washing). This has led the World Health Organization to establish an international alliance for the global elimination of blinding trachoma by the year 2020.
In spite of many decades of research, there are still no vaccines for chlamydial infections. This is partly because immunopathology itself makes a major contribution to the disease, and vaccine-induced immune responses could be harmful.
Other conjunctival infections
In resource-rich countries, conjunctivitis is caused by a variety of bacteria
Several bacteria (especially Haemophilus influenzae, Staphylococcus aureus, and Streptococcus pneumoniae) can cause conjunctivitis (Fig. 25.3).
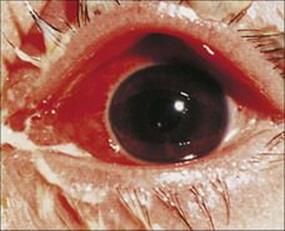
Figure 25.3 Purulent discharge in bacterial conjunctivitis is often associated with infections by Streptococcus pneumoniae, Haemophilus influenzae or Staphylococcus aureus.
(Courtesy of M. Tapert.)
Infection by Neisseria gonorrhoeae is a hazard of birth through an infected birth canal, and can result in a severe purulent condition. It is seen on the first or second day of life (ophthalmia neonatorum) and requires urgent treatment with ceftriaxone (penicillin resistance is widespread). Staph. aureus also produces infections in newborns as well as in adults. The eyes of infants may be invaded by this organism if the organism is transferred from the child’s own body or from an infected adult. Despite vaccine development, Haemophilus influenzae continues to be a significant cause of conjunctivitis in children since the strains are non-typeable (nonencapsulated).
Direct infection of the eye may be associated with wearing contact lenses
Excessive wearing of contact lenses can lead to a reduction in the effectiveness of the eye’s defence mechanisms, allowing pathogens to become established, but more likely hazards are the use of contaminated eye drops or cleaning solutions and the insertion of contaminated lenses. A number of bacteria can be transmitted directly in this way. Species of the free-living amoeba Acanthamoeba can multiply in unchanged lens cleaning fluids and be transferred when the lens is inserted, causing corneal ulceration. Diagnosis is by microscopy and culture of corneal scrapings. PCR can be used to type isolates.
Conjunctival infection may be transmitted by the blood or nervous system
Several organisms invade the superficial tissues of the eye after transport through the blood or, in the case of herpes simplex virus (HSV), by movement along the trigeminal nerve. Reactivation of this virus can result in the development of a keratitis with the formation of dendritic ulcers (Fig. 25.4). The keratitis can lead to corneal scarring with new blood vessel formation, neovascularization, resulting in loss of sight. Antiviral drugs such as aciclovir and famciclovir, combined with steroid treatment, may be effective. However, if uncontrolled, corneal transplantation may be necessary. Varicella-zoster virus may cause conjunctivitis associated with chickenpox or as a secondary infection. Overall, viral conjunctivitis is most commonly caused by adenovirus infections. Many years ago, due to the strong occupational association, shipyard eye was the name given to adenoviral conjunctivitis seen in shipbuilders and other workers exposed to the risk of eye injuries that could then result in an adenovirus infection. These viruses also cause pharyngoconjunctival fever, which includes, as one might expect, pharyngitis, fever and an acute follicular conjunctivitis that clears within a few weeks.
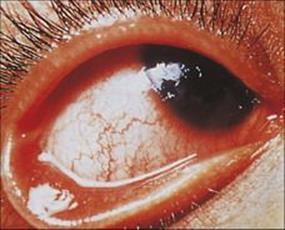
Figure 25.4 Herpes simplex virus (HSV) keratitis. Dendritic ulcers, seen here on the cornea, are common in recurrent HSV infections.
(Courtesy of M.J. Wood.)
Infection of the deeper layers of the eye
The spectrum of organisms causing disease in the deeper layers of the eye is wider than that associated with the conjunctiva (Table 25.2).
Table 25.2 Infections of the deep layers of the eye
|
Organism |
Disease |
Route of infection |
|
Rubella virus |
Cataracts, microphthalmia |
Infection in utero |
|
Cytomegalovirus |
Chorioretinitis |
Infection in utero; may occur in AIDS and other immunocompromised individuals |
|
Pseudomonas aeruginosa |
Serious inner eye infection |
After trauma; foreign bodies in eye; eye operations; bacteria can contaminate eye drops |
|
Toxoplasma gondii (toxoplasmosis) |
Chorioretinitis |
Infection in utero |
|
Echinococcus granulosus (hydatid disease) |
Distortion of the eye by growth of larval tapeworm in hydatid cyst |
Transmission by eggs passed by dogs |
|
Toxocara canis (ocular toxocariasis) |
Chorioretinitis, posterior pole granuloma, blindness |
Transmission by eggs passed by dogs |
|
Onchocerca volvulus (river blindness) |
Sclerosing keratitis, chorioretinitis |
Larvae transmitted by blood-feeding Simulium flies |
Entry into the deeper layers occurs by many routes
Trauma to the eye may result in the opportunistic establishment of a Pseudomonas aeruginosa infection, giving rise to serious inner eye infection. This organism may also be introduced via contaminated eye drops. Congenital syphilis produces a retinopathy with quiescent lesions, and keratitis may appear in later life. Secondary syphilis is also associated with ocular inflammation.
Rubella virus and cytomegalovirus (CMV) may invade the fetal eye in utero, the former causing cataracts and microphthalmia, the latter a severe chorioretinitis. CMV can also cause chorioretinitis in AIDS patients, although highly active antiretroviral therapy has resulted in a large reduction of eye disease (see Fig. 21.26E). Ocular complications have been reported in patients with West Nile virus infection.
Toxoplasmosis
Toxoplasma gondii infection can cause retinochoroiditis leading to blindness
Infection with this protozoan is widespread in adults and children (see Ch. 5), and is normally acquired by swallowing oocysts released by infected cats (the definitive host) or by eating meat containing tissue cysts. Women who become infected in pregnancy may transmit the infection to the fetus, as tachyzoites can cross the placenta. Tissue cysts can form in the retina of the fetus and undergo continuous proliferation, producing progressive lesions, particularly when levels of immunity are low. These lesions may also involve the choroid (Fig. 25.5) and lead ultimately to blindness. One or both eyes may be affected.
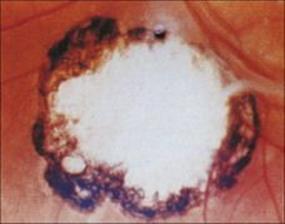
Figure 25.5 Congenital toxoplasmosis. Fundal photograph showing the scar of healed chorioretinitis.
(Courtesy of M.J. Wood.)
Infection is not serious unless:
• acquired in utero, when the organism invades all tissues, especially the central nervous system (CNS)
• acquired (or reactivated) under immunosuppression.
Damage to the eye occurs both in congenital (Fig. 25.5) and in postnatally acquired toxoplasmosis and may present at any age. Ocular toxoplasmosis may present years after the initial infection, whether congenital or acquired postnatally, and can be more serious in the elderly population.
Parasitic worm infections
Toxocara canis larvae cause an intense inflammatory response and can lead to retinal detachment
Larval tapeworms (e.g. the hydatid cyst stage of Echinococcus granulosus transmitted by eggs passed from infected dogs) occasionally enter the eye, with growth of the cysts causing severe mechanical damage. Invasion by migratory larvae of the nematode Toxocara canis is more common. This parasite occurs naturally in the intestines of dogs, releasing thick-shelled resistant eggs into the environment. The eggs can hatch if swallowed by humans, the larvae initiating, but failing to complete, their customary migration through the tissues. In the canine host, migration results in the worms re-entering the intestine where they mature. In humans, larvae can enter almost any organ, often the CNS or eye (Fig. 25.6), triggering an intense eosinophilic inflammatory response. In the eye, Toxocara larvae may lead to posterior uveitis, localized retinal granuloma, traction bands and retinal detachment. The misdiagnosis of retinal granuloma as retinoblastoma has led to enucleation. Serology on serum samples may give false-negative results in ocular toxocariasis; serology may need to be performed on vitreous samples to make the diagnosis. Anthelmintic treatment is not routinely given as it may lead to worsening of inflammation; corticosteroids are used to suppress the inflammatory response. Laser photocoagulation has also been used to destroy Toxocara larvae.

Figure 25.6 Toxocara. Granuloma in the posterior pole of an infected eye. The larval nematode is clearly visible in the centre of the granuloma.
(Courtesy of D. Spalton.)
Onchocerca volvulus infection causes ‘river blindness’ and is transmitted by Simulium flies
Onchocerca volvulus infection, the cause of ‘river blindness’ in Africa and Central America, is transmitted by biting Simulium flies, which take up microfilariae larvae from the skin of infected hosts and reintroduce the larvae after they have further developed to become infective, at a future feed. Adult worms live in subcutaneous nodules, and are comparatively harmless. The microfilariae, released by the females in enormous numbers, induce intense inflammatory reactions in the skin (see Ch. 26). The larvae migrate through the subcutaneous tissue, and invasion of the eye has been particularly common in certain regions of Africa as well as Central America.
The inflammatory responses in the eye cause a number of pathologic changes, which may affect both the anterior and posterior chambers (Fig. 25.7). These include:
• punctate and sclerosing keratitis
• iridocyclitis
• chorioretinitis
• optic atrophy.
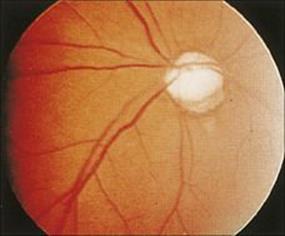
Figure 25.7 Onchocerciasis. Sclerosis of the choroidal vessels caused by invading microfilaria of Onchocerca volvulus.
(Courtesy of J. Anderson.)
The disease is called river blindness because the Simulium flies develop in fast flowing rivers, and people living near these sites are most affected. In the past, blindness rates have reached 40% of the adult population in endemic areas, but vector control and especially ivermectin treatment have dramatically reduced the incidence of new infections in many African countries. Unfortunately, the blindness is irreversible.
![]()
 Key Facts
Key Facts
• The external surfaces of the eye are vulnerable to infection. It is protected by the eyelids and by factors such as lysozyme in tears.
• It can be difficult to make a diagnosis regarding the aetiology of conjunctivitis on clinical signs and symptoms alone.
• The consequences of eye infection are always potentially serious given that sight is dependent upon the presence of an intact transparent cornea.
• Microbes infecting the conjunctiva have specific attachment mechanisms.
• Inflammatory responses, though ‘designed’ to limit invasion and repair damage, can irreversibly damage conjunctival and corneal surfaces.
• Relatively few organisms invade the retina, and those that do are potentially sight-threatening.
• Some of the most serious infection-related diseases of the eye involve invasion by protozoan or helminth parasites. The diagnosis then often follows rather than precedes the development of visual impairment.
![]()