Medical Microbiology
Section 1 The adversaries – microbes
6 The helminths and arthropods
Introduction
The term ‘helminth’ is used for all groups of parasitic worms. Three main groups are important in humans: the tapeworms (Cestoda), the flukes (Trematoda or Digenea) and the roundworms (Nematoda). The first two belong to the Platyhelminths or flatworms; the third are included in a separate phylum. Platyhelminths have flattened bodies with muscular suckers and/or hooks for attachment to the host. Nematodes (roundworms) have long cylindrical bodies and generally lack specialized attachment organs. Helminths are generally large organisms with a complex body organization. Although invading larval stages may measure only 100–200 μm, adult worms may be centimetres or even metres long. Infections are commonest in warmer countries, but intestinal species also occur in temperate regions. The arthropods are the largest and arguably most successful single group of animals. Those of most relevance to human disease are the insects, ticks and mites. Many of these have adapted to live on humans or use humans as sources of food (blood and tissue fluid). Linked with these feeding habits is the ability of many arthropods to transmit a very wide variety of microbial pathogens. Others, acting as intermediate hosts, may transmit helminth parasites when eaten, and yet other species can inflict dangerous bites and stings.
The helminths
Transmission of helminths occurs in four distinct ways
Transmission routes are summarized in Figure 6.1. Infection can occur after:
• swallowing infective eggs or larvae via the faecal–oral route
• swallowing infective larvae in the tissues of another host
• active penetration of the skin by larval stages
• the bite of an infected blood-sucking insect vector.
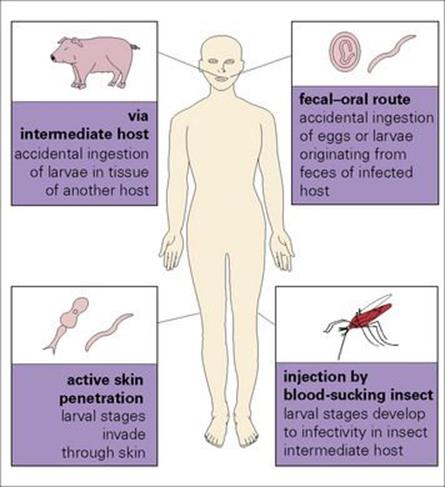
Figure 6.1 How helminth parasites enter the body.
The greater frequency of helminths in tropical and subtropical regions reflects the climatic conditions that favour survival of infective stages, the socioeconomic conditions that facilitate faecal–oral contact, the practices involved in food preparation and consumption, and the availability of suitable vectors. Elsewhere, infections are commonest in children, in individuals closely associated with domestic animals and in individuals with particular food preferences.
Many helminths live in the intestine, while others live in the deeper tissues. Almost all organs of the body can be parasitized. Flukes and nematodes actively feed on host tissues or on the intestinal contents; tapeworms have no digestive system and absorb predigested nutrients.
The majority of helminths do not replicate within the host, although certain tapeworm larval stages can reproduce asexually in humans. In most, sexual reproduction results in the production of eggs, which are released from the host in faecal material. In others, reproductive stages may accumulate within the host, but do not mature. The nematode Strongyloides is exceptional in that eggs produced in the intestine can hatch there, releasing infective larvae, which re-invade the body – the process of ‘autoinfection’.
The outer surfaces of helminths provide the primary host–parasite interface
In tapeworms and flukes, the surface is a complex plasma membrane, and in both there are protective mechanisms to prevent the host damaging the outer surface. The nematode outer surface is a tough collagenous cuticle, which, although antigenic, is largely resistant to immune attack. However, smaller larval stages may be damaged by host granulocytes and macrophages. Worms release large amounts of soluble antigenic material in their excretions and secretions, and this plays an important role both in immunity and pathology.
Life cycles
Many helminths have complex life cycles
In direct life cycles, reproductive stages produced by sexually mature adults in one host are released from the body and can develop directly to adult stages after infection of another host via the faecal–oral route (Ascaris) or by direct penetration (hookworms). Indirect cycles are those where reproductive stages must undergo further development in an intermediate host (tapeworms) or vector (filarial worms) before sexual maturity can be achieved in the final host.
The larvae of flukes and tapeworms must pass through one or more intermediate hosts, but those of nematodes can develop to maturity within a single host
Most flukes are hermaphrodites, except the schistosomes, which have separate sexes. The reproductive organs of tapeworms are replicated along the body (the strobila) in a series of identical segments or ‘proglottids’. The terminal ‘gravid’ proglottids become filled with mature eggs, detach and pass out in the faeces. The eggs of both flukes and tapeworms develop into larvae that must pass through one or more intermediate hosts and develop into other larval stages before the parasite is again infective to humans. The tapeworm Hymenolepis nana, occasionally found in humans, is exceptional and can go through a complete cycle from egg to adult in the same host.
In nematodes, the sexes are separate. Most species liberate fertilized eggs, but some release early-stage larvae directly into the host’s body. Development from egg or larva to adult can be direct and occur in a single host, or may be indirect, requiring development in the body of an intermediate host. Classification of nematodes is complex, and for practical purposes only two categories of human-specific nematodes are considered here:
• those that mature within the gastrointestinal tract, some of which may migrate through the body during development (e.g. Ascaris, hookworms, Trichinella, Strongyloides, Trichuris)
• those that mature in deeper tissues (e.g. the filarial nematodes).
In addition, humans can be infected with the larvae of species that mature in other hosts (e.g. the dog parasites Toxocara canis and Ancylostoma brasiliense).
Helminths and disease
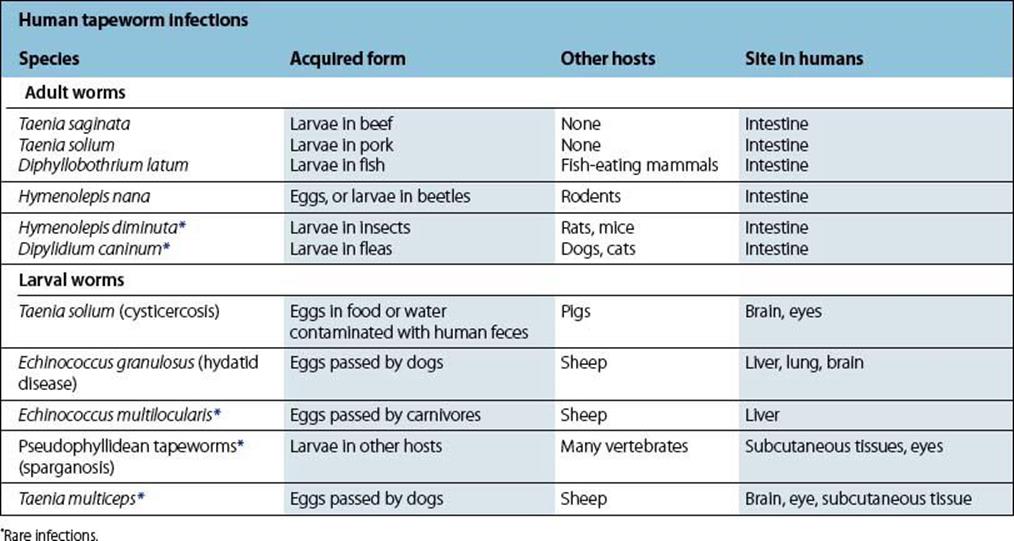
Adult tapeworms are acquired by eating undercooked or raw meat containing larval stages
Tapeworms frequently infect humans, but are relatively harmless despite their potential for reaching a large size. Humans can also act as the intermediate hosts for certain species, and the development of larval stages in the body can cause severe disease (Table 6.1).
Table 6.1 Summary of the location, transmission and other hosts used by tapeworms that infect humans
The most important flukes are those causing schistosomiasis
Several species of fluke can mature in humans, developing in the intestine, lungs, liver and blood vessels. The most important, both in terms of prevalence and pathology, are the blood flukes or schistosomes, the cause of schistosomiasis or bilharzia. Three main species, Schistosoma haematobium, Schistosoma japonicum and Schistosoma mansoni, infect many millions and are responsible for severe disease (Table 6.2). Like all flukes, schistosomes have an indirect life cycle involving stages of larval development in the body of a snail, in this case aquatic snails. Humans become infected when they come into contact with water containing infective larvae released from the snails, the larvae penetrating through the skin. Other important species are Clonorchis sinensis, a liver fluke, and Paragonimus westermani, the lung fluke, transmitted by eating infected fish or crabs, respectively.
Table 6.2 Summary of the location and transmission of flukes that infect humans
|
Human fluke infections |
||
|
Species |
Acquired form |
Site in humans |
|
Schistosoma haematobium |
|
Blood vessels of bladder |
|
Clonorchis sinensis |
Ingesting fish infected with larval stages |
Liver |
|
Fasciola hepatica |
Ingesting vegetation (cress) with larval stages |
Liver |
|
Paragonimus westermani |
Ingesting crabs infected with larval stages |
Lungs |
Certain nematodes that infect humans are highly specific; others are zoonoses
Several of the many species of nematode that infect humans are highly specific and can mature in no other host. Others have a much lower host specificity, being acquired accidentally as zoonoses, with humans acting either as the intermediate or the final host after picking up infection from domestic animals or in food (Table 6.3).
Table 6.3 Summary of the location and transmission of nematodes that infect humans
|
Human nematode infections |
||
|
Species |
Acquired by |
Site in humans |
|
Transmitted person to person |
||
|
Ascaris lumbricoides |
Ingestion of eggs |
Small intestine |
|
Enterobius vermicularis |
Ingestion of eggs |
Large intestine |
|
Hookworms |
Skin penetration by infective larvae |
Small intestine |
|
Strongyloides stercoralis |
Skin penetration by infective larvae; autoinfection |
Small intestine (adults), general tissues (larvae) |
|
Trichuris trichiura |
Ingestion of eggs |
Large intestine |
|
Transmitted person to person via arthropod vector |
||
|
Brugia malayi |
Bite of mosquito carrying infective larvae |
Lymphatics (adults), blood (larvae) |
|
Onchocerca volvulus |
Bite of Simulium fly carrying infective larvae |
Skin (larvae, adults), eye (larva) |
|
Wuchereria bancrofti |
Bite of mosquito carrying infective larvae |
Lymphatics (adults), blood (larvae) |
|
Loa loa |
Bite of deer-fly carrying infective larvae |
Tissues |
|
Zoonoses transmitted from animals |
||
|
Angiostrongylus cantonensis |
Ingestion of larvae in snails, crustacea |
CNS (larvae) |
|
Anisakis simplex |
Ingestion of larvae in fish |
Stomach, small intestine (larvae) |
|
Capillaria philippinensis |
Ingestion of larvae in fish |
Small intestine (adults, larvae) |
|
Toxocara canis* |
Ingestion of eggs passed by dogs |
Tissues, CNS (larvae) |
|
Trichinella spiralis* |
Ingestion of larvae in pork, meat of wild mammals |
Small intestine (adults), muscles (larvae) |
* These species are the commonest in this group.
Survival of helminths in their hosts
Many helminth infections are long lived, the worms surviving in their hosts for many years, despite living in parts of the body where there are effective immune defences. How this is achieved has been worked out in several species. Some, such as the schistosomes, disguise themselves from the immune system by acquiring host molecules on their outer surface, so they are less easily recognized as foreign invaders. Others actively suppress the host’s immune responses by releasing factors that interfere with, or divert, protective responses. The ability of worms to do this is being actively investigated as a potential therapeutic approach to the control of immunologically mediated conditions such as allergy and autoimmunity. It may one day be possible to protect patients at risk from these conditions by giving them a parasite infection!
The arthropods
Arthropods cause disease directly by their feeding and indirectly by transmitting infections.
Many arthropods feed on human blood and tissue fluids
Blood feeders include mosquitoes, midges, biting flies, bugs, fleas and ticks. Some mites also feed in this way, chiggers, the larvae of trombiculid mites, being a familiar example. Contact may be temporary or permanent. Mosquitoes are temporary ectoparasites, feeding for only a few minutes; ticks feed for much longer. The head and body forms of the louse Pediculus humanus, and the crab louse Phthirus pubis, spend almost all of their lives on humans, feeding on blood and reproducing on the body or in clothing. The scabies mite Sarcoptes scabiei lives permanently on humans, burrowing into the superficial layers of skin to feed and lay eggs. Heavy infections can build up, particularly on individuals with reduced immune responsiveness, causing a severe inflammatory condition (see Ch. 26).
Arthropod infestation carries the additional hazard of disease transmission
Arthropods transmit pathogens of all major groups, from viruses to worms and some (e.g. mosquitoes and ticks) transmit a wide variety of organisms (Table 6.4). The ability to transmit infections acquired from animals to humans poses a constant threat of acquiring zoonoses. Some vector-borne infections, such as yellow fever, have been known for centuries, whereas others, such as the viral encephalitides and Lyme disease, have been recognized more recently (1920s and 1975, respectively). Mosquito-transmitted West Nile virus has become a significant threat in North America, with sporadic cases and outbreaks reported from Europe (see Ch. 27).
Table 6.4 Summary of infectious diseases transmitted by arthropods
|
Infectious diseases transmitted by arthropods |
||
|
Disease |
Arthropod vector |
|
|
Viruses |
||
|
Arboviruses |
|
MosquitoesMosquitoesMosquitoes, ticksTicks, mosquitoes |
|
Bacteria |
||
|
Yersinia pestis |
Plague |
Fleas |
|
Borrelia recurrentis |
Relapsing fever |
Soft ticks |
|
Borrelia burgdorferi |
Lyme disease |
Hard ticks |
|
Rickettsias |
||
|
R. prowazekii |
Epidemic typhus |
Lice, ticks |
|
R. mooseri |
Endemic (murine) typhus |
Fleas |
|
R. rickettsia |
Spotted fever |
Ticks |
|
R. akari |
Rickettsial pox |
Mites |
|
Protozoa |
||
|
Trypanosoma cruzi |
American trypanosomiasis (Chagas disease) |
Reduviid bugs |
|
T.b. rhodesiense |
|
Tsetse flies |
|
T.b. gambiense |
||
|
Plasmodium spp. |
Malaria |
Mosquitoes |
|
Leishmania spp. |
Leishmaniasis |
Sandflies |
|
Worms |
||
|
Wuchereria and Brugia |
Lymphatic filariasis |
Mosquitoes |
|
Onchocerca |
Onchocerciasis |
Simulium flies |
![]()
 Key Facts
Key Facts
• Helminths are multicellular worms that parasitize many organs of the body, most commonly the gastrointestinal tract.
• Transmission may be direct, through swallowing infective stages or by larvae penetrating the skin, or indirect via intermediate hosts or insect vectors.
• The most serious helminth infection is schistosomiasis, caused by infection with blood flukes. The pathology is primarily due to hypersensitivity reactions to eggs as they pass through tissues.
• Arthropods of importance in human disease are those that feed on blood or body tissues (insects, ticks, mites) and those which transmit other infections, particularly viruses, bacteria and protozoa.
![]()
![]()
 Conflicts
Conflicts
Helminths are typically large parasites, often covered by a protective outer layer, so they are difficult for the immune system to deal with – too big for phagocytosis or cytotoxic T cells and unaffected by direct antibody activity. They are often active and mobile and can move away from host defences, damaging host tissues as they do so. Many disguise their outer surfaces or produce immunosuppressive factors. Because they are long-lived and able to survive despite immune responses, they can produce chronic disease, either as a consequence of their activity or because of misdirected and pathological host immune responses. Reliance on direct infection through faecal–oral contact, or transmission by vectors, makes it difficult to avoid infection when climate and low standards of hygiene combine to tilt the balance in favour of the parasite. Treatment with anthelmintics works against many intestinal worms, but re-infection is almost routine in areas of poor sanitation, necessitating regular re-treatment programmes. Those living in the tissues are much more difficult to deal with, e.g. hydatid cysts may require major surgery as well as antiparasitic drugs, and there are still no effective drugs for the treatment of Guinea Worm.
![]()