Case Files Biochemistry, 3rd Edition (2015)
SECTION II. Clinical Cases
CASE 15
A 59-year-old man is brought to the emergency department (ED) by the emergency medical services after a family member found him extremely confused and disoriented, with an unsteady gait and strange irregular eye movements. The patient has been known in the past to be a heavy drinker. He has no known medical problems and denies any other drug usage. On examination, he is afebrile with a pulse of 110 beats/minute and a normal blood pressure. He is extremely disoriented and agitated. Horizontal rapid eye movement on lateral gaze is noted bilaterally. His gait is very unsteady. The remainder of his examination is normal. The urine drug screen was negative and he had a positive blood alcohol level. The ED physician administers thiamine.
![]() What is the most likely diagnosis?
What is the most likely diagnosis?
![]() What is importance of thiamine in biochemical reactions?
What is importance of thiamine in biochemical reactions?
ANSWERS TO CASE 15:
Thiamine Deficiency
Summary: A 59-year-old man with a history of heavy alcohol use presents with mental confusion, ataxia, and ophthalmoplegia.
• Most likely diagnosis: Wernicke-Korsakoff syndrome (thiamine deficiency) often associated with chronic users of alcohol.
• Importance of thiamine: An important water-soluble vitamin used as a cofactor in enzymatic reactions involving the transfer of an aldehyde group. Without thiamine, individuals can develop dementia, macrocytic anemia (folate deficiency), gastritis, peptic ulcer disease, liver disease, depression, nutritional deficiencies, cardiomyopathy, and pancreatitis.
CLINICAL CORRELATION
Thiamine, also known as vitamin B1, is fairly ubiquitous. Thiamine deficiency is uncommon except in alcoholics as a result of nutritional deficiencies and malabsorption. The classic clinical triad of dementia, ataxia (difficulty with walking), and eye findings may be seen, but more commonly, only forgetfulness is noted. Sometimes, thiamine deficiency can lead to vague symptoms such as leg numbness or tingling. Because thiamine is water soluble, it can be added to intravenous fluids and administered in that way. Other manifestations include beri-beri disease, which is cardiac involvement leading to a high cardiac output, and vasodilation. Affected patients often feel warm and flushed, and they can have heart failure.
APPROACH TO:
Thiamine Pyrophosphate
OBJECTIVES
1. Know about the role of thiamine pyrophosphate (TPP) in pyruvate dehydrogenase.
2. Understand the role of TPP in α-ketoglutarate dehydrogenase and the role of TPP in transketolase in pentose phosphate pathway.
3. Be familiar with how thiamine deficiency results in decreased energy generation and how it results in decreased ribose and NADPH production.
DEFINITIONS
CARBANION: A carbon within a molecule that has a negative charge because of the removal of a proton (hydrogen ion).
DECARBOXYLATION: The process of removing a carboxyl group (–COOH) from a molecule. Frequently this is achieved by oxidizing the compound in a process known as oxidative decarboxylation.
DEHYDROGENASE: An enzyme that oxidizes a molecule by the removal of a pair of electrons and 1 or 2 protons.
NUCLEOPHILIC ADDITION: The process of forming a bond between an electron-rich group (nucleophile) and an electron-deficient atom (electrophile).
OXIDATION: The removal of electrons from an atom or compound.
THIAMINE: Vitamin B1; a water-soluble vitamin containing a thiazolium ring. The active form of the vitamin is thiamine pyrophosphate, which is an important coenzyme for many biochemical reactions.
DISCUSSION
Thiamine (vitamin B1) is an important water-soluble vitamin that, in its active form of thiamine pyrophosphate, is used as a cofactor in enzymatic reactions that involve the transfer of an aldehyde group. Thiamine can be synthesized by plants and some microorganisms, but not usually by animals. Hence, humans must obtain thiamine from the diet, though small amounts may be obtained from synthesis by intestinal bacteria. Because of its importance in metabolic reactions, it is present in large amounts in skeletal muscle, heart, liver, kidney, and brain. Thus, it has a widespread distribution in foods, but there can be a substantial loss of thiamine during cooking above 212°F (100°C).
Thiamine is absorbed in the intestine by both active transport mechanisms and passive diffusion. The active form of the cofactor, TPP (thiamine pyrophosphate), is synthesized by an enzymatic transfer of a pyrophosphate group from ATP to thiamine (Figure 15-1). The resulting TPP has a reactive carbon on the thiazole ring that is easily ionized to form a carbanion, which can undergo nucleophilic addition reactions.
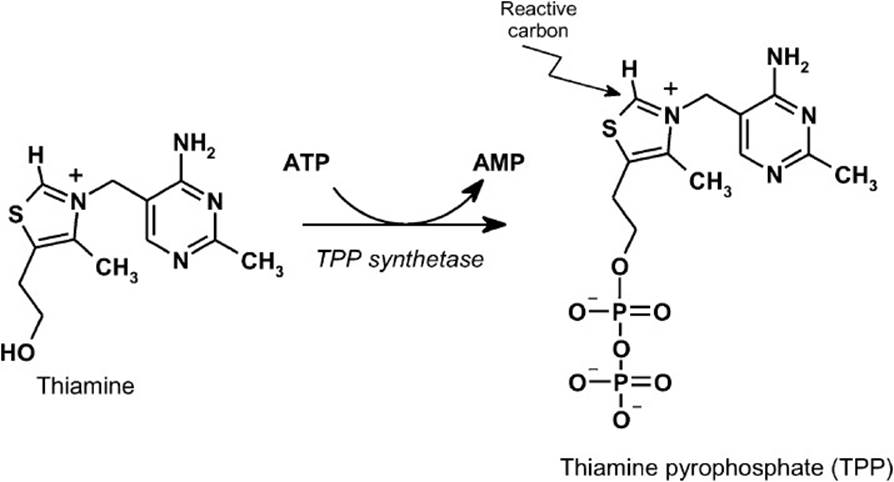
Figure 15-1. Activation of thiamine (vitamin B1) to the active cofactor, thiamine pyrophosphate (TPP) by the enzyme TPP synthetase.
Thiamine pyrophosphate is an essential cofactor for enzymes that catalyze the oxidative decarboxylation of α-keto acids to form an acylated coenzyme A (acyl CoA). These include pyruvate dehydrogenase (pyruvate → acetyl-CoA), α-ketoglutarate dehydrogenase (α-KG → succinyl-CoA) and branched-chain α-keto acid dehydrogenase. These 3 enzymes operate by a similar catalytic mechanism (Figure 15-2). Each of these enzymes is a multi-subunit complex with 3 enzymatic activities that require the participation of several cofactors. The first activity (E1) is the dehydrogenase complex, which has TPP as the enzyme-bound cofactor. The carbanion form of TPP attacks the carbonyl carbon of the α-keto acid, releasing CO2 and leaving a hydroxyalkyl-TPP intermediate. The hydroxyalkyl group reacts with the oxidized form of lipoamide, the prosthetic group of dihydrolipoyl transacetylase (E2), which is the second component of the complex. The resulting acyllipoamide reacts with coenzyme A (HSCoA) to form the product, acyl CoA, and leaving lipoamide in the fully reduced form. To regenerate the fully oxidized form of lipoamide for further rounds of the reaction, it interacts with the third component of the complex, dihydrolipoyl dehydrogenase (E3), which has covalently bound FAD. The FAD accepts the reducing equivalents from the reduced lipoamide to form FADH2 and oxidized lipoamide. The reducing equivalents are then transferred to NAD+ to form NADH, which is regenerated via the electron transport system with the production of ATP.
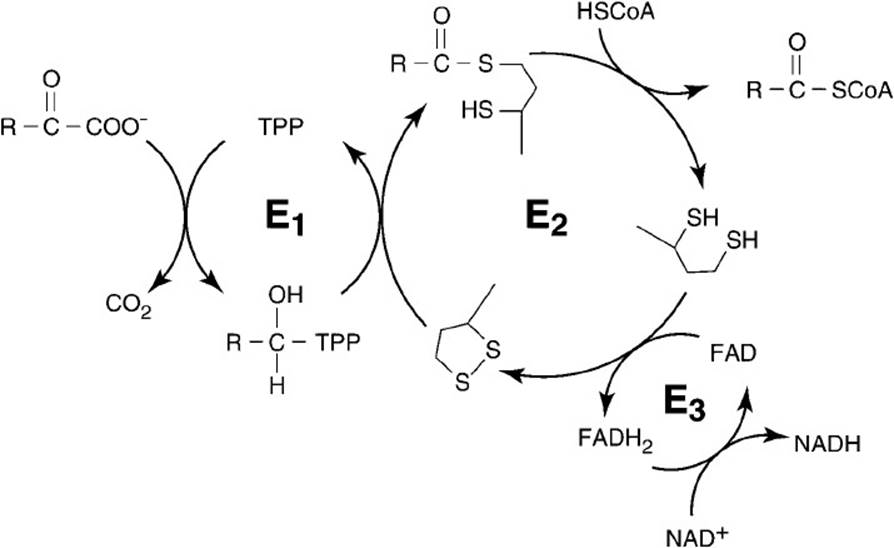
Figure 15-2. The catalytic mechanism shared by the enzymes pyruvate dehydrogenase, α-ketoglutarate dehydrogenase, and branched-chain α-ketoacid dehydrogenase. E1 is the dehydrogenase complex; E2 is the dihydrolipoyl transacetylase subunit; and E3 is the dihydrolipoyl dehydrogenase component. E1 and E2 are specific to each enzyme, and E3 is common to all 3 enzymes.
The E1 and E2 components are specific for each of the pyruvate dehydrogenase, α -ketoglutarate dehydrogenase, and branched-chain α -keto acid dehydrogenase complexes. However, the E3 component is identical for all of the enzymes.
Thiamine pyrophosphate is also an important cofactor for the transketolase reactions in the pentose phosphate pathway of carbohydrate metabolism (Figure 15-3). These reactions are important in the reversible transformation of pentoses into the glycolytic intermediates fructose 6-phosphate and glyceraldehyde 3-phosphate. Again, it is the reactive carbon on the thiazole ring of TPP that reacts with a ketose phosphate (xylulose 5-phosphate) to cause the release of an aldose phosphate with 2 fewer carbons (glyceraldehyde 3-phosphate). The TPP-bound glycoaldehyde unit is then transferred to a different aldose phosphate (ribose 5-phosphate or erythrose 4-phosphate) to produce a ketose phosphate that has 2 carbons more (sedoheptulose 7-phosphate or fructose 6-phosphate).
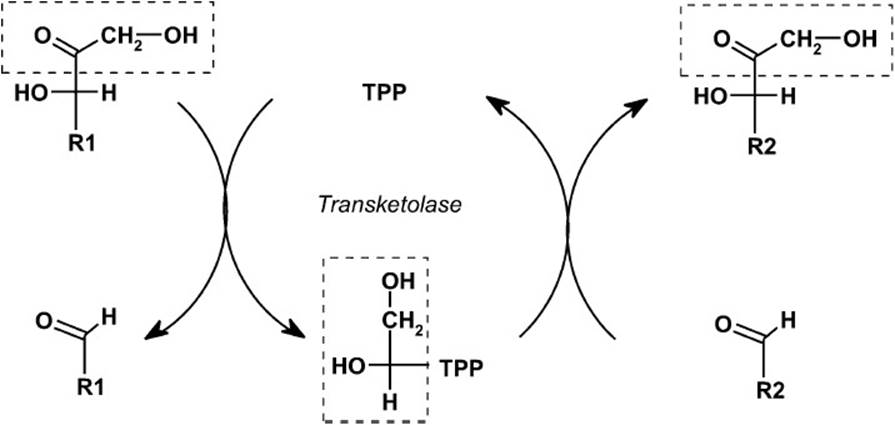
Figure 15-3. The reaction catalyzed by the enzyme transketolase, which transfers a glycoaldehyde group from a ketose to an aldose.
A deficiency in thiamine will decrease the efficiency of the enzymes for which TPP is required as a cofactor. Thus, the rate of conversion of pyruvate to acetyl-CoA and the flow of acetyl-CoA through the tricarboxylic acid cycle will be depressed as a result of the inefficiency of the TPP-requiring enzymes pyruvate dehydrogenase and α-ketoglutarate dehydrogenase. The production of the reduced electron carrier, NADH, and the ATP produced from it via oxidative phosphorylation will be decreased as a consequence. Because nervous tissue and heart use at high rates ATP synthesized from the oxidation of NADH produced from pyruvate conversion to acetyl-CoA and from the tricarboxylic acid (TCA) cycle, these tissues are most affected by a deficiency in thiamine. When deficient in thiamine, the brain can no longer efficiently metabolize pyruvate through the TCA cycle to produce ATP and thus must convert it to lactate to produce ATP. This increased conversion of pyruvate to lactate decreases the pH in areas of the brain that have rapid ATP turnover rates and leads to cellular destruction.
A deficiency in thiamine also adversely affects the flux of glucose metabolized by the pentose phosphate pathway. Transketolase activity requires the cofactor TPP to transfer the glycoaldehyde unit from a ketose to an aldose in the remodeling reactions of the pathway. When these reactions cannot proceed, precursor metabolites build up, and the flow through the pathway is decreased. This results in a decreased production of NADPH and decreased conversion of glucose to pentose, including ribose. This can lead to decreased regeneration of reduced glutathione and susceptibility to oxidative stress.
Thiamine turnover is rapid because of the ubiquitous presence of thiaminase enzymes that hydrolyze thiamine into its pyrimidine and thiazole components. Thus, symptoms of thiamine deficiency can appear within 2 weeks of a diet depleted in thiamine. In Western societies, severe thiamine deficiency is most frequently found in alcoholics. Patients who chronically misuse alcohol are prone to thiamine deficiency arising from a number of factors including poor nutrition and poor absorption and storage, as well as an increased breakdown of TPP. Alcohol is known to inhibit the active absorption of thiamine.
Thiamine deficiency is most frequently assessed by assaying erythrocyte transketolase activity in the presence as well as the absence of added TPP. If the red blood cells have sufficient thiamine, then the transketolase will be fully saturated with TPP, and no increase in activity will be observed when TPP is added to the assay system. An increase in transketolase activity indicates that the patient is thiamine deficient.
COMPREHENSION QUESTIONS
15.1 A full-term female infant failed to gain weight and showed metabolic acidosis in the neonatal period. A physical examination at 6 months showed failure to thrive, hypotonia, small muscle mass, severe head lag, and a persistent acidosis (pH 7.0–7.2). Blood lactate, pyruvate, and alanine were greatly elevated. Treatment with thiamine did not alleviate the lactic acidosis.
Which of the following enzymes is most likely deficient in this patient?
A. Alanine aminotransferase
B. Phosphoenolpyruvate carboxykinase
C. Pyruvate carboxylase
D. Pyruvate dehydrogenase
E. Pyruvate kinase
15.2 A 3-month-old male infant developed seizures and progressively worsened, showing hypotonia, psychomotor retardation, and poor head control. He had lactic acidosis and an elevated plasma pyruvate level, both of which were more than 7 times the normal amount. Pyruvate carboxylase activity was measured using extracts of fibroblasts and was found to be less than 1% of the normal level. Oral administration of which of the following amino acids would you recommend as the best therapy for this patient?
A. Alanine
B. Glutamine
C. Leucine
D. Lysine
E. Serine
15.3 A deficiency in thiamine (vitamin B1) would most likely lead to which of the following clinical manifestations?
A. Decrease in carboxylase enzyme activity
B. Decrease in serum lactate concentrations
C. Decrease in red blood cell transketolase activity
D. Increase in urinary methylmalonate
E. Increase in prothrombin time
ANSWERS
15.1 D. The increased concentrations of pyruvate, lactate, and alanine indicate that there is a block in the pathway leading from pyruvate toward the TCA cycle. A deficiency in pyruvate dehydrogenase would lead to a buildup of pyruvate. Pyruvate has 3 fates other than conversion to acetyl-CoA by pyruvate dehydrogenase: conversion to oxaloacetate by pyruvate carboxylase, reduction to lactate by lactate dehydrogenase, and transamination to the amino acid alanine. Thus, because pyruvate builds up, an increase in lactate and alanine would be expected if pyruvate dehydrogenase was deficient.
15.2 B. A deficiency in pyruvate carboxylase results in a diminution of oxaloacetate, the C4 acid that acts as the acceptor for an acetyl group from acetyl-CoA. In order for the TCA cycle to continue efficiently, C4 acids must be replenished. Amino acids whose carbon skeletons feed into the TCA cycle and increase the C4 pool will accomplish this. Glutamine, which is converted to α-ketoglutarate, will lead to an increase in all of the C4 acids (succinate, fumarate, malate, and oxaloacetate). Alanine and serine are converted to pyruvate, which as a result of the deficiency in pyruvate carboxylase will not increase the C4 pool. Lysine and leucine are ketogenic amino acids and thus also do not increase the C4 pool.
15.3 C. In addition to being an important cofactor for the enzymes involved in the oxidative decarboxylation of pyruvate, α-ketoglutarate, and branched-chain α-ketoacids, thiamine is also a cofactor for the enzyme transketolase, the enzyme that transfers a glycoaldehyde group from a ketose sugar to an aldose sugar in the pentose phosphate pathway. One of the diagnostic tools in determining thiamine deficiency is determination of the activity of red blood cell transketolase in the presence and absence of added thiamine. Thiamine deficiency would be expected to increase blood lactate concentrations. Biotin deficiency would lead to decreased carboxylase activity, whereas an increased methylmalonate concentration would be observed with vitamin B12 deficiency. Vitamin K deficiency would lead to an increase in prothrombin time.
BIOCHEMISTRY PEARLS
![]() Thiamine (vitamin B1) is an important water-soluble vitamin that, in its active form of TPP, is used as a cofactor in enzymatic reactions that involve the transfer of an aldehyde group.
Thiamine (vitamin B1) is an important water-soluble vitamin that, in its active form of TPP, is used as a cofactor in enzymatic reactions that involve the transfer of an aldehyde group.
![]() Thiamine deficiency is uncommon except in people who abuse alcohol who, as a consequence of nutritional deficiencies and malabsorption, may become deficient.
Thiamine deficiency is uncommon except in people who abuse alcohol who, as a consequence of nutritional deficiencies and malabsorption, may become deficient.
![]() The classic clinical triad of dementia, ataxia (difficulty with walking), and eye findings may be seen, but more commonly, forgetfulness alone is noted.
The classic clinical triad of dementia, ataxia (difficulty with walking), and eye findings may be seen, but more commonly, forgetfulness alone is noted.
![]() Thiamine pyrophosphate is also an important cofactor for many dehydrogenase reactions as well as the transketolase reactions in the pentose phosphate pathway of carbohydrate metabolism.
Thiamine pyrophosphate is also an important cofactor for many dehydrogenase reactions as well as the transketolase reactions in the pentose phosphate pathway of carbohydrate metabolism.
REFERENCES
Murray RK, Bender DA, Botham KM, et al, eds. Harper’s Illustrated Biochemistry. 29th ed. New York: Lange Medical Books/McGraw-Hill; 2012.
Wilson JD. Vitamin deficiency and excess. In: Longo D, Fauci AS, Kaspar D, et al, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2011.