Case Files Biochemistry, 3rd Edition (2015)
SECTION II. Clinical Cases
CASE 18
A 27-year-old man presented to the emergency department with the signs and symptoms of acute appendicitis. He was promptly sent to the operating room for emergency appendectomy. The patient was prepped and draped for the surgery, and halothane was given as an inhalation anesthetic. A total of 2 minutes after the anesthetic was given, the patient was noted to have an extremely elevated temperature, muscle rigidity, and tachypnea. Arterial blood gas test revealed metabolic acidosis, and a serum electrolytes study demonstrated hyperkalemia. A nurse quickly went to talk to the family about the events, and the family mentioned that the only other person to have surgery in their family had a similar reaction and died. The physician makes a diagnosis of malignant hyperthermia (MH).
![]() What is the biochemical basis of this disease?
What is the biochemical basis of this disease?
![]() What is the best treatment for this condition?
What is the best treatment for this condition?
ANSWERS TO CASE 18:
Malignant Hyperthermia
Summary: 27-year-old man with acute appendicitis undergoing a halothane inhaled anesthetic with acute onset of hyperthermia, tachypnea, respiratory acidosis, hyperkalemia, and family history of similar events. The tentative diagnosis is MH.
• Biochemical mechanism: Uncoupling of oxidative phosphorylation.
• Treatment: Supportive care with attempts to bring temperature down, correct blood gas and electrolyte abnormalities, and give dantrolene.
CLINICAL CORRELATION
MH is an untoward response of susceptible individuals to preoperative anesthesia utilizing halothane and succinylcholine, although other inhalation anesthetics such as enflurane and isoflurane have been recognized as milder prompts for this complication of anesthesia. The frequency of occurrence is 1 in 15,000 children and 1 in 100,000 adults. The inheritance is dominant in 50% of cases and recessive in 20%, suggesting a more complex basis for this response. The clinical findings are muscle rigidity, hyperthermia, seizure, cardiac arrhythmias, and sometimes death. Prevention is the key, in that every patient should be queried about personal or family history of complications during surgery. Once a patient is found to have MH, the health care professional should alert other family members to the same possibility. The muscle relaxant, dantrolene, is the treatment of choice. Even with prompt recognition and therapy, the mortality rate is as high as 5%.
APPROACH TO:
Oxidative Phosphorylation (Uncoupling)
OBJECTIVES
1. Understand how MH is caused by the uncoupling of oxidative phosphorylation.
2. Understand the biochemical mechanism for the heat production.
3. Be familiar with the mechanism of how dantrolene reverses the effects.
DEFINITIONS
MALIGNANT HYPERTHERMIA (MH): An unusual adverse response to some inhalation anesthetics such as halothane in which there is an acute dramatic elevation in body temperature as well as tachypnea, muscle rigidity, and hyperkalemia.
Ca2+ SIGNALING: Many enzymes in metabolism and signaling pathways are responsive to Ca2+ concentrations. Calcium is sequestered within tissues (eg, within cisternae in the sarcoplasmic reticulum of muscle) and released on signal increasing the Ca2+ concentration in the cytosolic compartment and eliciting Ca2+-induced responses. Increased calcium concentration stimulates the activity of muscle phosphorylase kinase and activates pyruvate dehydrogenase phosphatase to increase the metabolic flow of glucose to CO2 and H2O.
Ca2+ CHANNEL: A transport system allowing passage of the charged calcium ion through a hydrophobic membrane.
DISCUSSION
Hyperthermia is a rare complication of anesthesia not completely understood. Most of the evidence points to the ryanodine receptor (chromosome 19q13.1) as the defective gene product. This receptor is the Ca2+ release channel of muscle sarcoplasmic reticulum. Stimulation of this channel leads to excessive Ca2+ release from the cisternae of the sarcoplasmic reticulum, and that Ca2+ prompts muscle contraction, an increase in body temperature, tachycardia, and subsequent metabolic acidosis.
The scheme in Figure 18-1 summarizes the effects of Ca2+ release on processes that bring about the complex of symptoms seen in malignant hyperthermia. Increased Ca2+ release triggers the binding of adenosine triphosphate (ATP)-charged myosin to actin to initiate muscle contraction. This muscle contraction may be repeated to the point of muscle rigidity with attendant muscle damage and release of myoglobin. The sustained muscle contraction uses increased amounts of ATP increasing demands on glycolysis, tricarboxylic acid (TCA) cycle, and oxidative phosphorylation. Ca2+ release serves to activate, at least partially, phosphorylase kinase, which speeds the mobilization of glycogen stores for ATP generation. Sympathetic outflow triggered by these changes leads to increased activation of glycogen breakdown and lipolysis. Fatty acids serve as a signal to increase the levels of uncoupling proteins in various tissues. The uncoupling proteins form channels in mitochondria allowing proton reentry into the mitochondrial matrix. Because the phosphorylation of adenosine diphosphate (ADP) to ATP depends on the proton gradient through the ATP synthase, these channels collapse the proton gradient allowing electron transport to occur without the phosphorylation of ADP (Figure 18-2). Because ATP is being consumed at an elevated rate and mitochondrial production of ATP is compromised, glycolysis increases to compensate for the shortfall in ATP production. Pyruvate and lactate, the end products of glycolysis, increase in concentration, giving rise to the metabolic acidosis observed.
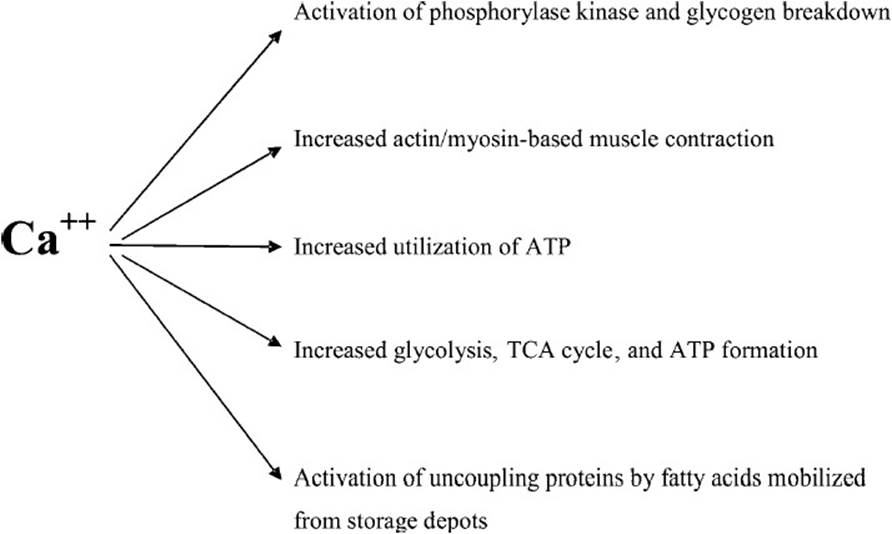
Figure 18-1. Direct and indirect effects of Ca2+ release in aberrant response to anesthetics halothane and succinylcholine.
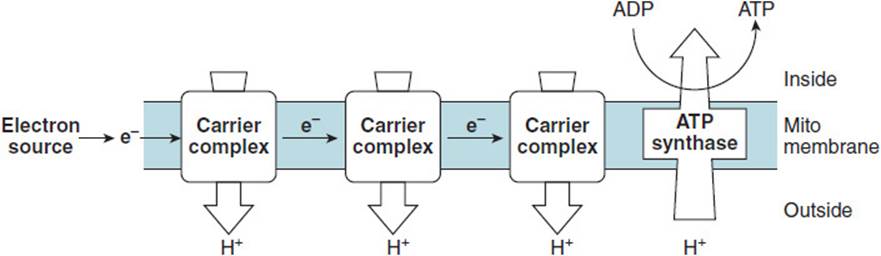
Figure 18-2. Electron transport system showing development of proton gradient outside the mitochondrial membrane by the passage of electrons down the chain.
The uncoupling proteins (UCPs; numbered 1-5) are a physiologic mechanism for maintaining body temperature through selective uncoupling of electron transport from ATP synthesis. The free energy release normally captured in the formation of the high-energy phosphate bond when phosphorylating ADP to ATP is lost as heat and changes body temperature. Physiologically, sympathetic outflow and catecholamine hormone release prompt new synthesis of the uncoupling proteins in response to the hypothalamus sensing lowered body temperature. In the case of malignant hyperthermia, this mechanism is triggered by anesthetic challenge to the calcium release channel, and the subsequent metabolic and signaling changes assembled above unfold.
Treatment of MH depends on cessation of anesthesia, mechanical means to reduce the temperature, and the correction of blood electrolyte and gas parameters to normal. In addition, dantrolene is infused initially intravenously and then may be given orally (Figure 18-3). Dantrolene brings about the reduction in contraction of skeletal muscles by decreasing the amount of Ca2+ released from the sarcoplasmic reticulum. A serious adverse event of dantrolene use is its potential hepatotoxicity. The hepatotoxicity is fatal to 0.1% to 0.2% of patients treated for 60 days or longer. Thus, use of dantrolene for longer than 45 days requires monitoring of hepatic markers.
Figure 18-3. Structure of dantrolene (1-{[5-(4-nitrophenyl)-2-furyl]methylideneamino}imidazolidine-2, 4-dione).
COMPREHENSION QUESTIONS
18.1 A young and otherwise healthy student undergoing preparation for a simple surgical procedure was noticed to have an elevating temperature and respiratory rate with muscle rigidity following the onset of anesthesia using halothane and succinylcholine. Laboratory findings revealed elevated levels of calcium, hydrogen ion, pyruvate, and lactate. The diagnosis was MH. The muscle rigidity observed in this patient is most likely prompted by which of the following?
A. Patient’s fear of surgery
B. Increased levels of hydrogen ion, causing the muscles to become immobile
C. Increased Ca2+ levels in muscle tissue, triggering muscle contraction
D. Increased pyruvate and lactate, causing precipitation of muscle protein
E. Increased body temperature
18.2 Rapidly elevating body temperature was observed in the patient in question 18.1. The underlying cause for this pyretic episode is which of the following?
A. Hypothalamic upward adjustment of body temperature set point in response to cold operating room temperature
B. Muscles producing heat from exertion of contraction
C. Uncoupling proteins allowing dissipation of the mitochondrial hydrogen ion gradient releasing energy as heat
D. Metabolism of fatty acids from lipid storage depots releasing heat
E. Elevated consumption of ATP to support muscle contraction releasing heat
18.3 Which of the following best describes the mechanism of action of dantrolene in the treatment of MH?
A. Decrease of Ca2+ release
B. Reduction of body temperature with hypothalamic set temperature
C. Effect on mitochondrial ATP production
D. Nuclear transcription attenuation
E. Recoupling of the sodium and ATP channels
ANSWERS
18.1 C. Release of Ca2+ triggers actin–myosin reaction, prompting muscle contraction. Neither fear of surgery nor hydrogen ion levels causes concerted muscle contraction. Increased pyruvate/lactate or temperature tends to counteract contraction.
18.2 C. MH does not involve central brain control of temperature but is caused by metabolic alterations. Regardless of the source of energy—whether fatty acids or the utilization of ATP to support muscle contraction—the electron transport chain is involved. Uncoupling of oxidation from ADP phosphorylation is caused by uncoupling proteins that dissipate energy as heat. This causes the elevation of body temperature seen in this patient.
18.3 A. Dantrolene brings about reduction in contraction of skeletal muscles by decreasing the amount of Ca2+ released from the sarcoplasmic reticulum. In addition, supportive care is aimed at decreasing body temperature and correcting the metabolic acidosis and electrolyte balance.
BIOCHEMISTRY PEARLS
![]() MH is most likely, given that anesthetic agents stimulate a calcium release channel, leading to excessive Ca2+ release from the cisternae of the sarcoplasmic reticulum, in turn causing muscle contraction, increased body temperature, tachycardia, and subsequent metabolic acidosis–“most likely” at beginning makes this a pearl about this case, not about MH in general.
MH is most likely, given that anesthetic agents stimulate a calcium release channel, leading to excessive Ca2+ release from the cisternae of the sarcoplasmic reticulum, in turn causing muscle contraction, increased body temperature, tachycardia, and subsequent metabolic acidosis–“most likely” at beginning makes this a pearl about this case, not about MH in general.
![]() Although the UCPs 1 to 5 are a physiologic mechanism for maintaining body temperature through selective uncoupling of electron transport from ATP synthesis, MH is a pathologic exaggeration of this process.
Although the UCPs 1 to 5 are a physiologic mechanism for maintaining body temperature through selective uncoupling of electron transport from ATP synthesis, MH is a pathologic exaggeration of this process.
![]() The treatment of MH includes stopping the anesthesia, cooling the patient, and administration of dantrolene, which reduces muscle contractions by decreasing the amount of Ca2+ released from the sarcoplasmic reticulum.
The treatment of MH includes stopping the anesthesia, cooling the patient, and administration of dantrolene, which reduces muscle contractions by decreasing the amount of Ca2+ released from the sarcoplasmic reticulum.
REFERENCE
Brunton L, Chabner B, Bjorn Knollman, eds. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill; 2010.