Case Files Biochemistry, 3rd Edition (2015)
SECTION II. Clinical Cases
CASE 39
The mother of a 16-year-old girl calls the clinic because of concerns about her daughter’s eating habits. The mother states that she will not eat anything and is obsessed with exercise and losing weight. She also states that her daughter has been more withdrawn from friends and family. After discussion with the mother, the patient comes in for a physical examination. The patient is 5 foot 1 inch tall and weighs 85 pounds. She is in no acute distress but appears to have a depressed affect. The patient states she is worried that her friends will think she is fat if she eats more. She denies any binge eating. Her physical examination is normal, other than dry skin and thin fine hair on extremities. Laboratory tests reveal that she is anemic and has a low albumin and magnesium level. She has normal liver and thyroid tests.
![]() What is the most likely diagnosis?
What is the most likely diagnosis?
![]() What potential medical problems may develop in a patient with this disorder?
What potential medical problems may develop in a patient with this disorder?
![]() How can this disorder affect her menstrual cycles?
How can this disorder affect her menstrual cycles?
ANSWERS TO CASE 39:
Anorexia Nervosa
Summary: A thin 16-year-old girl who is obsessed with her body appearance and weight to the point of not wanting to eat and is excessively exercising.
• Diagnosis: Anorexia nervosa. This is differentiated from bulimia because she denies binge eating with associated guilty feelings.
• Medical complications: Dry skin, lanugo, bradycardia, hypotension, dependent edema, hypothermia, anemia, osteoporosis, infertility, cardiac failure, and death.
• Menstrual complications: Amenorrhea secondary to depression of the hypothalamic-pituitary axis. Infertility will result secondary to anovulation.
CLINICAL CORRELATION
Anorexia nervosa is a disease affecting primarily young women who have distorted body images. Although their weight is less than 30% below ideal body weight, they see themselves as overweight. Anorectics often use diuretic and laxative agents to accomplish their weight loss. Patients with bulimia, who usually induce emesis, may be at normal weight or even above ideal body weight; by contrast, anorectics are almost always under ideal body weight. Often, affected individuals become amenorrheic, have fine lanugo hair, and become hypothermic. Therapy must be multifaceted and include family and individual counseling, behavioral modification, and possibly medication. Severe cases may be fatal.
APPROACH TO:
Amino Acid and Negative Protein Balance
OBJECTIVES
1. Describe protein digestion and amino acid absorption.
2. Explain how nitrogen is added and removed from amino acids.
3. Describe amino acid metabolism in various tissues (muscle, gastrointestinal [GI], kidney).
4. List the special products derived from amino acids.
DEFINITIONS
ANOREXIA NERVOSA: A mental disorder in which the patient has an extreme fear of becoming obese and an aversion to food. The disorder usually occurs in young women and can result in death if the condition is not successfully treated.
NITROGEN BALANCE: The condition wherein the amount of nitrogen ingested (via protein) is equal to that excreted. Negative nitrogen balance is a condition wherein more nitrogen is excreted than ingested, usually during prolonged periods of calorie restriction. Positive nitrogen balance results when more nitrogen is ingested than excreted, as in growing children.
PYRIDOXAL PHOSPHATE: The coenzyme that is required for transaminase (aminotransferase) reactions, as well as other enzymes. It is the active form of pyridoxine (vitamin B6).
DISCUSSION
Proteins are polymers of α-amino acids covalently linked via peptide bonds. α-Amino acids consist of a central (α) carbon atom to which an amino group, a carboxylic acid group, a hydrogen atom, and a side-chain group are covalently linked. Twenty different amino acids are used for protein synthesis, each of which is encoded by at least 1 codon (the 3 nucleotide genetic code) and differ only in their side-chain group. Amino acids can be divided into 2 classes, essential and nonessential amino acids. Essential amino acids cannot be synthesized by humans (unlike nonessential amino acids) and, thus, must be ingested to meet the requirements of the organism. Certain nonessential amino acids can become pseudoessential if the starting material from which they are synthesized becomes limiting (eg, methionine-derived cysteine). Amino acids are also used for the synthesis of nonprotein biomolecules (eg, nucleotides, neurotransmitters, antioxidants), as well as participating in critical whole body processes, such as interorgan nitrogen transfer and acid–base balance. Unlike carbohydrate and fatty acids, no storage form of excess amino acids exists per se. Instead, dietary amino acids in excess to the body’s synthetic needs are used as an energy source and/or converted to glycogen and lipid. During periods of insufficient nutrient ingestion(eg, starvation, anorexia nervosa), noncritical skeletal muscle and liver proteins are preferentially degraded to release utilizable amino acids, to meet both the biosynthetic and energy needs of the body (Figure 39-1).
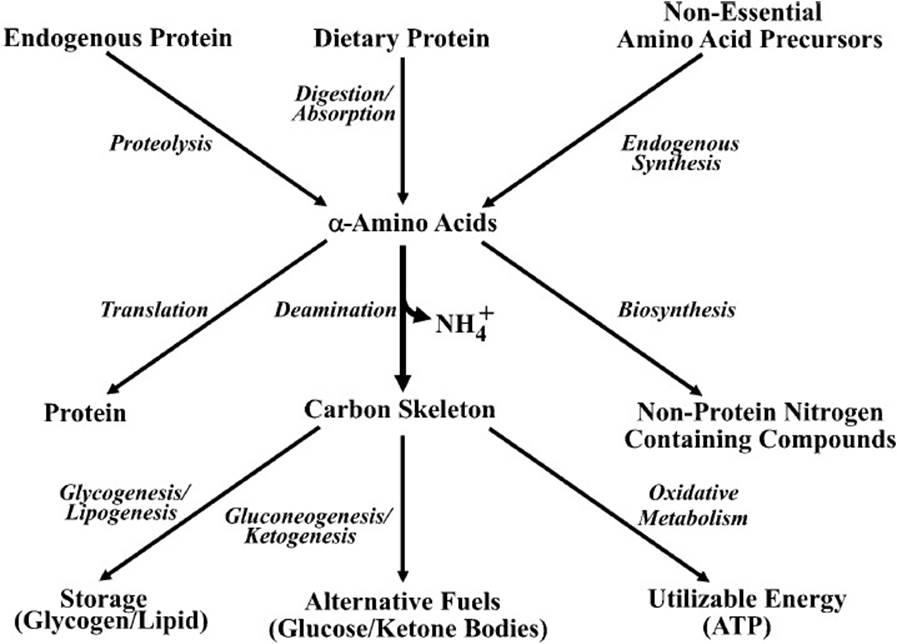
Figure 39-1. Schematic diagram showing the source and utilization of α-amino acids in metabolic processes.
The major sites of ingested protein digestion are the stomach and the small intestine. Gastric, pancreatic, and intestinal peptidases hydrolytically cleave peptide bonds. The released amino acids, dipeptides, and tripeptides are transported into small intestinal epithelial cells, wherein dipeptides and tripeptides are further degraded to free amino acids. The latter are subsequently released into the circulation. A healthy, well-fed adult is generally in nitrogen balance. This means that the amount of nitrogen ingested (as protein) is equal to that excreted (primarily as urea). When rates of dietary amino acid incorporation into new protein exceed rates of amino acid degradation and nitrogen excretion, the individual is said to be in positive nitrogen balance. Growing children are normally in positive nitrogen balance. By contrast, an individual is said to be in negative nitrogen balance when more nitrogen is excreted than ingested. This occurs during prolonged periods of calorie restriction (eg, starvation, anorexia nervosa), when protein is degraded to release amino acids as an utilizable energy source.
A general tactic employed during catabolism of amino acids is the removal of the α-amino group, followed by conversion of the remaining carbon skeleton into a major metabolic intermediate. The main way in which α-amino groups are removed is through transamination, the transfer of an amino group from an α-amino acid to an α-keto acid. This transamination reaction is catalyzed by a class of enzymes called transaminases (or aminotransferases). These enzymes use pyridoxal phosphate, a vitamin B6 derivative, during the catalytic process. Pyridoxal phosphate acts as an initial acceptor of the α-amino group, forming a Schiff base (–CH = N–) intermediate. The pyridoxamine phosphate intermediate subsequently donates the amino group to an acceptor α-keto acid, forming a new α-amino acid. The acceptor α-keto acid is most often α-ketoglutarate, thus resulting in glutamate generation. Not all amino acids are substrates for transaminases. Certain amino acids are initially converted into an intermediate that is subsequently transaminated (eg, asparagine is hydrolyzed to aspartate, the latter of which is transaminated by aspartate aminotransferase, forming oxaloacetate). Given that the majority of amino acids use transaminases in their pathways of degradation (although a select few amino acids can also be directly deaminated, eg, threonine), glutamate formation increases markedly during periods of increased amino acid catabolism. Ultimately, the majority of this glutamate is oxidatively deaminated in the liver, where the released ammonium is incorporated into urea, via the urea cycle, and subsequently excreted in urine (Figure 39-2).
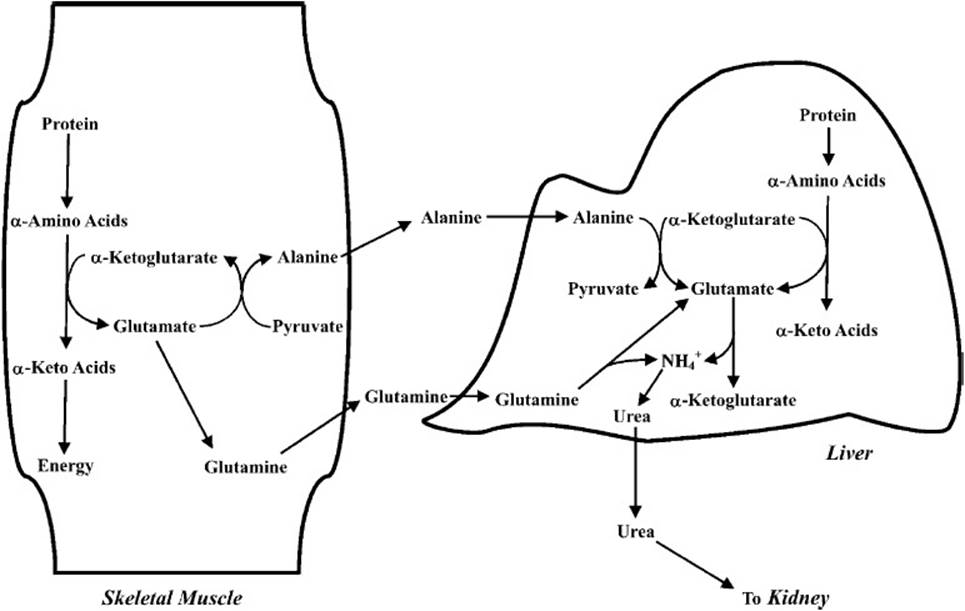
Figure 39-2. General pathway for the degradation of amino acids showing the relationship between extrahepatic tissues and the liver, which is the site of the formation of urea.
The carbon skeleton released during amino acid catabolism can undergo multiple fates, depending on the metabolic situation during which it was formed, the cell type within which it was generated, and the amino acid from which it is derived. For example, during periods of excess amino acid ingestion, the amino acid–derived carbon skeleton is either used as a metabolic fuel or converted to glycogen or lipid. By contrast, when rates of amino acid catabolism are increased as a result of prolonged caloric insufficiency, a large portion of the carbon skeleton is used by the liver for the synthesis of either glucose or ketone bodies, depending on the specific amino acid. Indeed, glucogenic amino acids (those amino acids whose carbon skeleton can generate net glucose through gluconeogenesis) are essential for maintenance of blood glucose levels during prolonged caloric insufficiency. Maintenance of blood glucose is also made possible by increased reliance of skeletal muscle on amino acids as a fuel source, thereby decreasing glucose utilization.
Certain amino acids are preferentially used in a tissue-specific manner. For example, skeletal muscle has a relatively high capacity for branched-chain amino acid (leucine, isoleucine, and valine) utilization. Following transamination, the carbon skeleton is oxidatively metabolized as an energy source during situations such as sustained exercise and caloric insufficiency. The amino group is transported in the circulation to the liver as either glutamine (formed by the enzymatic addition of an amino group to the side-chain group of glutamate) or alanine (formed by enzymatic transfer of the α-amino group from glutamate to pyruvate). Once at the liver, the transferred amino groups are ultimately used in urea synthesis, as described above (see Figure 39-2).
By contrast to skeletal muscle, which is the primary site of endogenous glutamine synthesis, rapidly dividing cells (eg, lymphocytes, enterocytes) preferentially use glutamine. The reason for this is that rapidly dividing cells require both energy as well as precursors for biosynthetic reactions. The carbon skeleton of glutamine enters intermediary metabolism via α-ketoglutarate, a Krebs cycle intermediate, providing the required energy for cellular processes. In addition, the amino groups of glutamine are used in purine and pyrimidine biosynthesis, which in turn are required for the synthesis of both RNA and DNA. Indeed, lymphocyte proliferation is greatly accelerated when glutamine is used as a metabolic substrate (as opposed to glucose), leading to suggestions that glutamine deficiency may result in immunosuppression and therefore increased susceptibility to infection. An additional reason for high rates of glutamine utilization in enterocytes appears to be for the synthesis of citrulline. The latter is transported to the kidney, where it is converted to arginine. Arginine is not only important in protein synthesis but also essential in cellular signaling (via nitric oxide production) and in maintaining adequate levels of urea cycle intermediates (Figure 39-3).
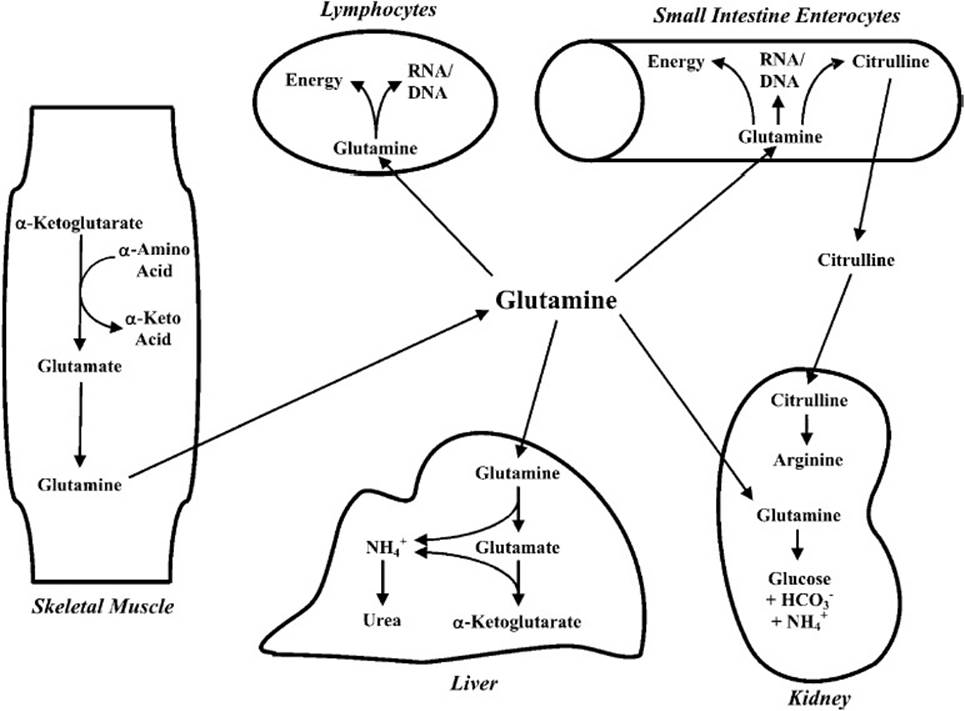
Figure 39-3. Schematic diagram showing the central role of glutamine as a transporter of amino acid nitrogen to various tissues.
Glutamine also plays an important role in maintenance of whole body acid–base balance. High rates of catabolism of positively charged and sulfur-containing amino acids result in the net formation of hydrogen ions. To maintain an acid–base balance, the kidney uses glutamine as a gluconeogenic precursor, resulting in the formation of glucose, bicarbonate ion, and ammonium (NH4+) ion formation. The bicarbonate is released into the circulation, where it associates with a proton (forming CO2 and H2O), thereby increasing blood pH. By contrast, the ammonium ion is excreted (see Figure 39-3).
As noted above, amino acids are not only used for protein synthesis but are also essential for the biosynthesis of other biomolecules. These include carnitine (a derivative of lysine), creatine (a derivative of glycine and arginine), glutathione (a derivative of glutamate, cysteine, and glycine), serotonin and melatonin (derivatives of tryptophan), dopamine, norepinephrine, and epinephrine (derivatives of tyrosine), as well as purines and pyrimidines (requiring aspartate and glutamine for biosynthesis). Alterations in dietary intake of amino acids can influence the rates at which these macromolecules are synthesized. For example, ingestion of a tryptophan-rich meal elevates neuronal serotonin synthesis, resulting in lethargy. Tryptophan crosses the blood–brain barrier via a transporter that is also specific for the branched-chain amino acids. Conditions that influence the tryptophan-to-branched-chain amino acid ratio in the circulation have been shown to affect serotonin levels in the brain because of competition for this transporter. For example, increased skeletal muscle branched-chain amino acid catabolism during starvation is associated with an increase in the blood tryptophan-to-branched-chain amino acid ratio, increased tryptophan uptake in the brain, and increased serotonin synthesis. The latter then influences wakefulness.
Amino acids also play an important role in cellular signaling. The guanidino group from arginine is used in the synthesis of nitric oxide, a ubiquitous, highly reactive signaling molecule that regulates multiple physiologic processes, including blood pressure, immune response, learning, and metabolism. Much less understood is the mechanism by which leucine affects cellular signaling. This amino acid has been termed a “pseudohormone” following the observations that one or more of its early metabolites (eg, α-ketoisocaproate) are among the strongest regulators of protein turnover identified to date.
COMPREHENSION QUESTIONS
For questions 39.1 to 39.3 refer to the following case: A 12-year-old girl is presented at the clinic with reports of frequent fainting and lethargy. The girl is 5 foot tall and weighs 80 pounds. Skin fold tests show an abnormally low percentage of body fat mass.
39.1 Which of the following is least likely to be consistent with the patient’s symptoms?
A. Anorexia nervosa
B. Bulimia
C. Type 1 diabetes
D. Type 2 diabetes
39.2 Which of the following hormones is likely to be severely diminished in the patient described above?
A. Cortisol
B. Epinephrine
C. Glucagon
D. Insulin
39.3 Which of the following metabolic fluxes would be most consistent in this patient?
A. Protein → amino acids
B. Glucose → fatty acids
C. Glucose → glycogen
D. Fatty acids → triacylglycerol
ANSWERS
39.1 D. Individuals with type 2 diabetes tend to be either overweight (a body mass index [BMI] between 25 and 30 kg/m2) or obese (BMI > 30 kg/m2). This may be due in part to chronic hyperinsulinemia. By contrast, decreased insulin levels associated with type 1 diabetes, anorexia, and bulimia will promote lipolysis and, thus, decreased adipose mass.
39.2 D. The low body weight and fat mass observed in the patient are consistent with a metabolically “fasted” state. During such a condition, circulating insulin levels will be low, whereas counter-regulatory hormones (eg, glucagon, epinephrine, and cortisol) will be elevated.
39.3 A. Consistent with a metabolically fasted state, decreased circulating insulin levels will signal attenuation of biosynthetic reaction and augmentation of catabolic reactions. The latter will provide necessary fuels to sustain the energetic needs of the body. Elevation of counter-regulator hormones (eg, glucagon, epinephrine, and cortisol) will synergistically stimulate catabolic processes. Increased proteolysis (protein → amino acids) in tissues such as skeletal muscle and the liver provide amino acids as a direct fuel source, as well as ketogenic and gluconeogenic precursors (depending on the individual amino acid).
BIOCHEMISTRY PEARLS
![]() Twenty different amino acids are used for protein synthesis, each of which is encoded by at least 1 codon (the 3-nucleotide genetic code) and differ only in their side-chain group.
Twenty different amino acids are used for protein synthesis, each of which is encoded by at least 1 codon (the 3-nucleotide genetic code) and differ only in their side-chain group.
![]() Amino acids can be divided into one of 2 classes, essential and nonessential amino acids. Humans cannot synthesize essential amino acids.
Amino acids can be divided into one of 2 classes, essential and nonessential amino acids. Humans cannot synthesize essential amino acids.
![]() Nitrogen balance refers to whether there is more or less nitrogen (protein) ingested than excreted.
Nitrogen balance refers to whether there is more or less nitrogen (protein) ingested than excreted.
![]() With prolonged caloric insufficiency, a large portion of the carbon skeleton is used by the liver for the synthesis of either glucose or ketone bodies, depending on the specific amino acid.
With prolonged caloric insufficiency, a large portion of the carbon skeleton is used by the liver for the synthesis of either glucose or ketone bodies, depending on the specific amino acid.
![]() Rapidly dividing cells (eg, lymphocytes, enterocytes) preferentially use glutamine for energy and biosynthetic purposes.
Rapidly dividing cells (eg, lymphocytes, enterocytes) preferentially use glutamine for energy and biosynthetic purposes.
REFERENCE
Newsholme EA, Leech AR. Biochemistry for the Medical Sciences. New York: Wiley; 1983.