Case Files Biochemistry, 3rd Edition (2015)
SECTION II. Clinical Cases
CASE 51
A 42-year-old woman presents to the clinic with complaints of vague abdominal discomfort, weakness, fatigue, and bone pain. The patient gives no personal or family history of medical problems. The patient did remember that she has had frequent urinary tract infections and has had several episodes of kidney stones. Her physical examination was within normal limits. The patient had a normal complete blood count, and electrolytes revealed a significantly elevated calcium level and low phosphorus level.
![]() What is the most likely diagnosis?
What is the most likely diagnosis?
![]() What is the biochemical secondary messenger activated in this disorder?
What is the biochemical secondary messenger activated in this disorder?
ANSWERS TO CASE 51:
Hyperparathyroidism
Summary: A 42-year-old woman with a history of frequent urinary tract infections and kidney stones is found to have vague abdominal pain and weakness, hypercalcemia, and decreased phosphorus levels.
• Diagnosis: Hyperparathyroidism, leading to hypercalcemia and hyperphosphatemia.
• Biochemical mechanism: Elevated parathyroid hormone level acts by binding its 7-helix plasma membrane receptor to activate the adenylate cyclase/protein kinase A signaling system.
CLINICAL CORRELATION
This patient presents with kidney stones, which causes severe flank pain. The most common causes of hypercalcemia include malignancies or hyperparathyroidism. Other causes include granulomatous disorders such as sarcoid and tuberculosis, and less commonly, hypercalcemia may be the presentation of intoxication with vitamins A or D, or calcium-containing antacids, or occur as a side effect of drug therapies like lithium or thiazide diuretics. Genetic conditions like familial hypocalciuric hypercalcemia and hyperparathyroidism as part of a multiple endocrine neoplasia syndrome are also uncommon. Primary hyperparathyroidism, usually because of a solitary parathyroid adenoma, is the most likely cause when hypercalcemia is discovered in an otherwise asymptomatic patient on routine laboratory screening. Most patients have no symptoms with mild hypercalcemia below 12.0 mg/dL, except perhaps some polyuria and dehydration. With levels above 13 mg/dL, patients begin developing increasingly severe symptoms. These include central nervous system symptoms (lethargy, stupor, coma, mental status changes, psychosis), gastrointestinal symptoms (anorexia, nausea, constipation, peptic ulcer disease), kidney problems (polyuria, nephrolithiasis), and musculoskeletal complaints (arthralgias, myalgias, weakness). The symptoms of hyperparathyroidism can be remembered as: stones (kidney), moans (abdominal pain), groans (myalgias), bones (bone pain), and psychiatric overtones. Diagnosis can be established by finding hypercalcemia and hypophosphatemia, with inappropriately elevated parathyroid hormone (PTH) levels. Symptomatic patients can be treated with parathyroidectomy.
APPROACH TO:
Calcium Metabolism
OBJECTIVES
1. Describe calcium metabolism.
2. Describe the regulation of serum calcium including the roles of PTH and calcitonin.
DEFINITIONS
CALCITONIN: A polypeptide hormone of 32-amino acid residues that is synthesized in the parafollicular cells (C cells) of the thyroid gland. Calcitonin is secreted in response to elevated blood Ca2+ levels.
IP3: Inositol 1,4,5-trisphosphate (inositol trisphosphate); a second messenger released by the action of phospholipase C on phosphatidylinositol 4,5-bisphosphate (PIP2). IP3 will bind to receptors on the endoplasmic reticulum (ER) to cause the rapid efflux of Ca2+ from the ER into the cytoplasm.
PHOSPHOINOSITIDE CASCADE: The sequence of events that follow the binding of a hormone to a receptor that acts via a Gq-protein. Hormone binding to the Gq-coupled receptor activates phospholipase C, which cleaves PIP2 to IP3 and diacylglycerol, both of which are second messengers.
PTH: Parathyroid hormone; an 84-amino acid polypeptide hormone that is synthesized in the parathyroid gland and is secreted in response to low blood Ca2+ levels. PTH acts to increase the Ca2+ concentration in the blood by stimulating osteoclast formation and activity, thus releasing bone calcium and phosphate into the blood.
VITAMIN D: Vitamin D3, a secosteroid (a steroid in which one of the rings has been opened) formed by the action of UV light on 7-dehydrocholesterol. The active form of vitamin D is the hormone 1, 25-dihydroxycholecalciferol (calcitriol), formed in the kidney in response to elevated PTH levels. It binds to nuclear receptors in intestine, bone, and kidney to activate the expression of calcium-binding proteins.
DISCUSSION
Owing to the critical importance of calcium ion in a wide range of physiologic processes, blood calcium ion concentrations are tightly regulated. Hypocalcemia rapidly leads to muscle spasm, tetany, cardiac dysfunction, and numerous other symptoms. About half of the calcium ions in blood are bound to protein, and one-half are in the unbound state. Blood calcium ion concentrations are close to 1 mM, a value 10,000 times higher than free calcium ion concentrations in the cytoplasm. Normal calcium and phosphate concentrations in blood are near their solubility limit. Thus, elevation in these levels leads to precipitate formation and organ damage.
Intracellular calcium ion is largely sequestered within mitochondria and the lumen of the endoplasmic reticulum. Inositol trisphosphate (IP3)—a second messenger of hormones that acts via stimulation of the phosphoinositide cascade (Figure 51-1)—binds its receptor on the endoplasmic reticulum membrane, triggering a rapid efflux of calcium ion from this intracellular store into the cytoplasm. The calcium-binding protein calmodulinsenses fluctuations in intracellular calcium ion concentration by altering its conformation, thus influencing activities of its numerous enzyme ligands, including the calcium ATPase. This spike in intracellular calcium concentration is restored to the resting level by the activity of calcium transporters including the calcium ATPase and the sodium/calcium exchanger.
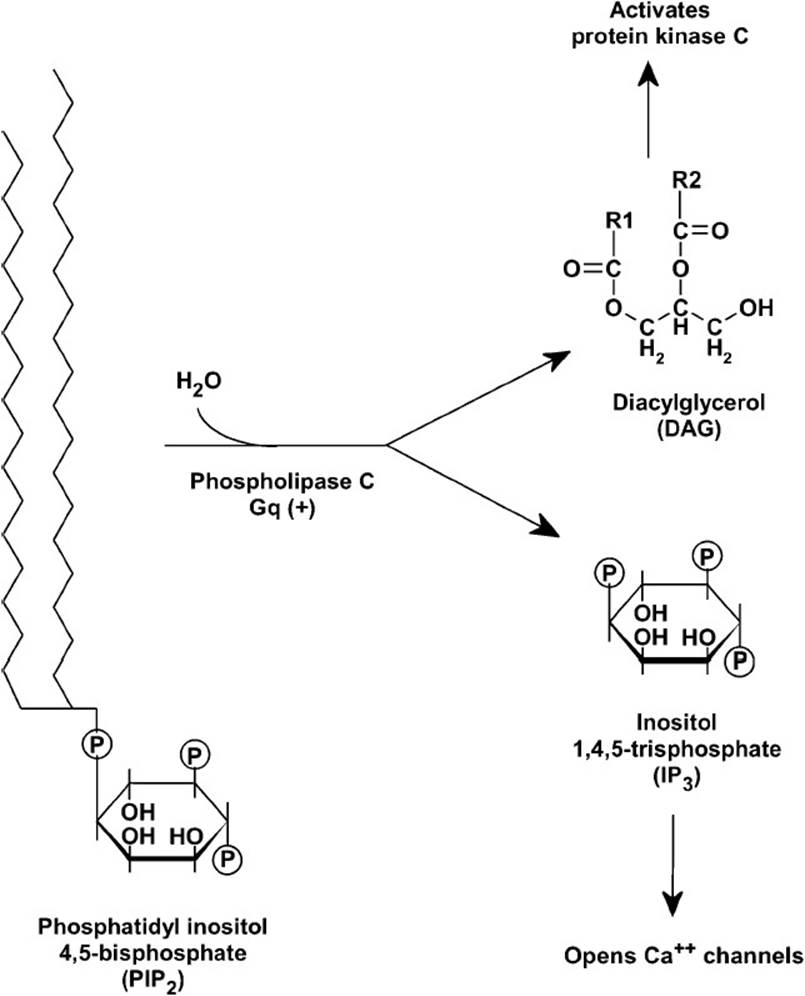
Figure 51-1. The phosphoinositide cascade. Binding of hormone to the Gq-coupled receptor leads to the activation of phospholipase C, which hydrolyzes PIP2 in the membrane to release the 2-second messengers, DAG and IP3.
PTH plays a crucial role in regulating concentrations of calcium and phosphorus in the extracellular fluid. The major signal for parathyroid hormone release is low extracellular levels of free calcium ion. PTH acts on 3 major targets—small intestine, kidney, and bone—to restore calcium ion concentrations in the extracellular fluid to the normal range if they fall too low.
PTH acts by binding its 7-helix plasma membrane receptor to activate the adenylate cyclase/protein kinase A signaling system. In some tissues, receptor binding is also coupled to the phosphoinositide signaling system to activate protein kinase C.
PTH is synthesized as a 115-amino acid preprohormone in the chief cells of the parathyroid gland, where it is processed by proteolysis to an active 84-amino acid polypeptide and packaged in secretory vesicles. When blood calcium ion levels fall below normal, the active hormone is secreted by exocytosis into the blood. The parathyroid cell monitors calcium ion levels by means of a calcium-sensing receptor in the plasma membrane. Phosphate ion is a much less significant regulator of PTH secretion and does so by an indirect mechanism. Within seconds of calcium binding its receptor on the chief cells of the parathyroid gland, PTH secretion is decreased. Within a matter of hours, transcription of the preprohormone messenger RNA diminishes. If hypocalcemia persists over days and months, then the parathyroid gland enlarges in an effort to increase PTH production.
Bone serves as a vast reservoir of calcium in the body. Approximately 1% of calcium in bone can rapidly exchange with extracellular calcium ion. PTH stimulates demineralization of bone and release of calcium and phosphate into the blood by stimulating osteoclast formation and activity. This process is synergistically enhanced by vitamin D.
PTH also acts to increase absorption of calcium ion by the small intestine. It does this indirectly by promoting the formation of active vitamin D in the kidney. PTH acts on the final, rate-limiting step in vitamin D synthesis, the formation of 1, 25-dihydroxycholecalciferol in the kidney. If PTH is low, then formation of the inactive derivative, 24, 25-dihydroxycholecalciferol, is stimulated instead. Vitamin D acts on intracellular receptors in the small intestine to increase transcription of genes encoding calcium uptake systems, to upregulate their expression.
The kidney plays a critical role in calcium homeostasis. PTH acts directly on the kidney to suppress calcium ion excretion in the urine by maximizing tubular calcium reabsorption. It increases phosphate ion excretion in the kidney (phosphaturic effect) to prevent excessive accumulation of this anion released during bone demineralization.
Hyperparathyroidism results from oversecretion of PTH. This condition leads to excessive bone turnover and demineralization and must be treated by removal of the parathyroid gland. The disorder is classified into primary, secondary, and tertiary hyperparathyroidism. Sporadic primary hyperparathyroidism is the third most common endocrine disorder, after diabetes and hyperthyroidism. It is most common in women older than 55 years of age and the leading cause is a single adenoma, which secretes the hormone constitutively, without regulation. Symptoms can include osteopenia and bone fractures, renal stones (resulting from hypercalciuria), peptic ulcer disease, and pancreatitis. In milder cases, patients are asymptomatic or have only muscle weakness, fatigue, and/or depression.
Secondary hyperparathyroidism arises from chronic hypocalcemia. This condition can result from renal failure leading to poor reabsorption of calcium from the urinary filtrate. It can also arise from poor nutrition or malabsorption of vitamin D by the intestine. In response, parathyroid glands increase their secretion of PTH. This condition also leads to decalcification of bone. Tertiary hyperparathyroidism is often seen after renal transplantation. In these patients, the parathyroid gland secretes the hormone independently of blood calcium levels.
Paradoxically, although chronic exposure to high PTH levels leads to bone decalcification, administration in pulses, as a once-a-day injection, stimulates an increase in bone mass. This treatment is now used as an effective therapy for osteoporosis. Calcitonin, secreted by the parafollicular C cells of the thyroid gland, opposes effects of PTH. Calcitonin is secreted when blood levels of calcium are too high, and it acts to suppress reabsorption of calcium in the kidney and inhibit bone demineralization. However, in humans, it plays a minor role in regulating blood levels of calcium ion.
COMPREHENSION QUESTIONS
51.1 A 54-year-old patient complained of muscle weakness, fatigue, and depression. She had a recent episode of renal stones and a bone scan revealed osteopenia. She had not yet entered menopause. She has taken a daily multivitamin tablet plus an additional 500 mg of calcium citrate for the last 20 years. Results from blood chemistry analysis indicated elevated levels of serum calcium ion. Urinalysis indicated phosphaturia. The patient’s symptoms are most likely caused by which of the following?
A. Excessive intake of vitamin D
B. Excess synthesis of parathyroid hormone
C. Excessive intake of calcium
D. Excess synthesis of calcitonin
E. Excess intake of phosphate
51.2 Before the introduction of vitamin D-fortified milk, children who spent most of their time indoors often developed rickets. In these vitamin D-deficient children, the most likely explanation for their bone malformations is which of the following?
A. Excessive renal excretion of calcium
B. Excessive renal excretion of phosphate ion
C. Inadequate uptake of calcium in the intestine
D. Lack of weight-bearing exercise
E. Excessive renal tubular reabsorption of calcium
51.3 Why can excessive ingestion of a phosphate-containing soft drink in otherwise well-nourished individuals lead to decreased bone density?
A. Increased levels of blood phosphate ion interact with sensors on the membrane of parathyroid cells to stimulate parathyroid hormone release.
B. Phosphate ion binds the active site on calcium transporters in the intestine, thus inhibiting their ability to transport calcium.
C. Phosphate ion depletes cellular levels of ATP, thus resulting in inhibition of Ca2+–ATPase calcium transporters.
D. Phosphate ion spontaneously forms an insoluble precipitate with calcium ion, thus decreasing its absorption in the intestine.
E. Phosphate ion is excessively incorporated into bone, thus weakening its structure.
ANSWERS
51.1 B. Hyperparathyroidism is the likely cause of all of the patient’s symptoms. Increased parathyroid hormone leads to bone demineralization, increased calcium uptake from the intestine, increased blood levels of calcium, decreased calcium ion excretion by the kidney, and increased phosphate excretion in the urine. Increased blood calcium levels caused renal stones, while bone demineralization progressed to osteopenia. The patient’s intake of calcium and vitamin D are not excessive. Calcitonin acts to decrease bone demineralization. Muscle weakness and depression reflect the widespread role of calcium ion in many physiologic processes.
51.2 C. The major action of vitamin D is to increase absorption of calcium from the small intestine. Deficiency of the vitamin leads to low blood calcium levels, stimulation of parathyroid hormone secretion, and acting synergistically, promotion of bone demineralization. Renal excretion of calcium is decreased by hypocalcemia but elevated parathyroid hormone levels promote renal excretion of phosphate, to prevent excessive accumulation of this product of bone demineralization. Although lack of exercise decreases bone density, it does not lead to rickets if vitamin D is sufficient.
51.3 D. Precipitate formation effectively decreases available calcium ion. Because of widespread consumption of soft drinks rather than water by school age children aided by school vending machines, this consequence is of concern.
BIOCHEMISTRY PEARLS
![]() Intracellular calcium ion is largely sequestered within mitochondria and the lumen of the endoplasmic reticulum.
Intracellular calcium ion is largely sequestered within mitochondria and the lumen of the endoplasmic reticulum.
![]() PTH acts on 3 major targets—small intestine, kidney, and bone—to restore calcium ion concentrations in the extracellular fluid to the normal range if they fall too low.
PTH acts on 3 major targets—small intestine, kidney, and bone—to restore calcium ion concentrations in the extracellular fluid to the normal range if they fall too low.
![]() Hyperparathyroidism causes elevated levels of calcium and phosphate.
Hyperparathyroidism causes elevated levels of calcium and phosphate.
![]() PTH acts by binding its 7-helix plasma membrane receptor to activate the adenylate cyclase/protein kinase A signaling system.
PTH acts by binding its 7-helix plasma membrane receptor to activate the adenylate cyclase/protein kinase A signaling system.
![]() PTH stimulates demineralization of bone and release of calcium and phosphate into the blood by stimulating osteoclast formation and activity, increases small bowel absorption of calcium ion, and acts directly on the kidney to suppress calcium ion excretion in the urine.
PTH stimulates demineralization of bone and release of calcium and phosphate into the blood by stimulating osteoclast formation and activity, increases small bowel absorption of calcium ion, and acts directly on the kidney to suppress calcium ion excretion in the urine.
REFERENCES
Chaney SG. Principles of nutrition II: micronutrients. In: Devlin TM, ed. Textbook of Biochemistry with Clinical Correlations. 7th ed. New York: Wiley-Liss; 2010.
Bowen RA, Austgen L, Rouge M. Pathophysiology of the Endocrine System. Colorado State University, 2006. http://arbl.cvmbs.colostate.edu/hbooks/pathphys/endocrine/.
Litwack G, Schmidt TJ. Biochemistry of hormones I: polypeptide hormones. In: Devlin TM, ed. Textbook of Biochemistry with Clinical Correlations. 7th ed. New York: Wiley-Liss; 2010.