Case Files Biochemistry, 3rd Edition (2015)
SECTION II. Clinical Cases
CASE 4
A 47-year-old woman is brought to the emergency department with complaints of malaise, nausea, vomiting, and fatigue. The patient reveals a long history of alcohol abuse for the last 10 years and requires drinks daily, especially in the morning as an “eye opener.” She has been to rehabilitation on several occasions for alcoholism but has not been able to stop drinking. She is currently homeless and jobless. She denies cough, fever, chills, upper respiratory symptoms, sick contacts, recent travel, hematemesis, or abdominal pain. She reports feeling hungry and has not eaten very well in a long time. On physical examination, she appears malnourished but in no distress. Other findings on physical exam are normal. Her blood count reveals a normal white blood cell count but does show an anemia with large red blood cells. Her amylase, lipase, and liver function tests were normal.
![]() What is the most likely cause of her anemia?
What is the most likely cause of her anemia?
![]() What is the molecular basis for the large erythrocytes?
What is the molecular basis for the large erythrocytes?
ANSWERS TO CASE 4:
Folic Acid Deficiency
Summary: 47-year-old alcoholic white woman has fatigue, malaise, nausea, vomiting, and poor nutritional intake with macrocytic anemia and no evidence of pancreatitis, liver disease, or peptic ulcer disease.
• Cause of anemia: Folic acid deficiency.
• Molecular basis of macrocytosis: Abnormal proliferation of erythroid precursors in the bone marrow, because folate deficiency encumbers the maturation of these cells by inhibition of DNA synthesis.
CLINICAL CORRELATION
Folate is an essential vitamin, found in green leafy vegetables. It is essential for many biochemical processes in the body, including DNA synthesis and red blood cell synthesis. Recently, folate supplementation has been found to be important in the prevention of fetal neural tube defects, such as anencephaly (absence of brain cerebral cortex and no skull or skin covering the brain) and spina bifida (spinal cord malformation, whereby the meninges are exposed leading to neurologic deficits). In particular, people who abuse alcohol are at risk for folate deficiency because of impaired gastrointestinal absorption and poor nutrition. Macrocytic anemia (large red blood cells) may be seen with folate deficiency. Treatment consists of folic acid replacement (usually 1 mg/day) by mouth with correction of anemia over the following 1 to 2 months. The diet usually requires adjustment, and correctable causes addressed (malnutrition in this case). Notably, folate deficiency in pregnancy has been associated with neural tube defects (NTDs) in fetuses. It is recommended that mothers take at least 400 μg of folic acid 3 months prior to conception to reduce the risk of NTD. At times, more than 400 μg of folic acid per day is recommended prior to conception. Some specific examples include a history of previous NTD, sickle cell disease, multiple gestations, and Crohn disease.
APPROACH TO:
Folate and DNA Synthesis
OBJECTIVES
1. Understand the important metabolic roles of folic acid with production of thymine, purine synthesis, and methionine.
2. Be aware of how folate deficiency causes megaloblastic anemia.
DEFINITIONS
S-ADENOSYL METHIONINE: An important carrier of activated methyl groups. It is formed by the condensation of ATP with the amino acid methionine catalyzed by the enzyme methionine adenosyltransferase in a reaction that releases triphosphate.
DIHYDROFOLATE REDUCTASE: The enzyme that reduces folic acid (folate) first to dihydrofolate and then to the active tetrahydrofolate. Dihydrofolate reductase uses NADPH as the source of the reducing equivalents for the reaction.
FOLIC ACID: An essential vitamin composed of a pteridine ring bound to p-aminobenzoate, which is in an amide linkage to one or more glutamate residues. The active form of the enzyme is tetrahydrofolate (THF; FH4), which is an important carrier of 1-carbon units in a variety of oxidation states.
MEGALOBLASTIC ANEMIA: An anemia characterized by macrocytic (large) erythrocytes produced by abnormal proliferation of erythroid precursors in the bone marrow due to a limitation in normal DNA synthesis. The cytoplasm continues to grow, even though the nucleus cannot due to DNA synthesis problems.
METHOTREXATE: One of a number of antifolate drugs, methotrexate, is an analog of folate that competitively inhibits dihydrofolate reductase. Because a plentiful supply of THF is required for ongoing synthesis of the pyrimidine nucleotide thymidylate, synthesis of this nucleotide is inhibited, resulting in decreased DNA synthesis.
METHYL TRAP: The sequestering of tetrahydrofolate as N5-methyl THF because of decreased conversion of homocysteine to methionine as a result of a deficiency of methionine synthase or its cofactor, cobalamin (vitamin B12).
DISCUSSION
Folate (folic acid) is an essential vitamin, which, in its active form of THF(Figure 4-1), transfers 1-carbon groups to intermediates in metabolism. Folate plays an important role in DNA synthesis. It is required for the de novo synthesis of purines and for the conversion of deoxyuridine 5-monophosphate (dUMP) to deoxythymidine 5′-monophosphate (dTMP). In addition, folate derivatives participate in the biosynthesis of choline, serine, glycine, and methionine. However, in situations of folate deficiency, symptoms are not observed from the lack of these products, as adequate levels of choline and amino acids are obtained from the diet (see also Case 3).
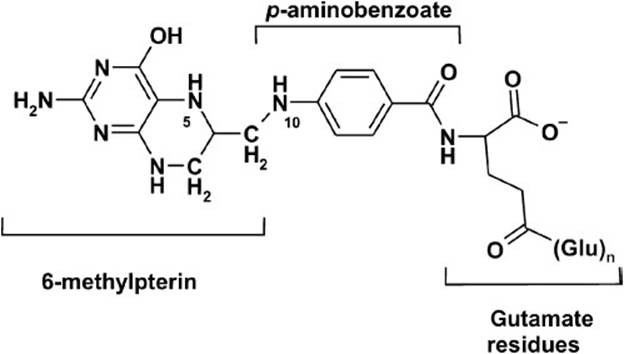
Figure 4-1. Structure of tetrahydrofolate, the active form of folic acid.
Folate deficiency results in megaloblastic anemia. Megaloblastic anemia is characterized by macrocytic erythrocytes produced by abnormal proliferation of erythroid precursors in the bone marrow. Folate deficiency encumbers the maturation of these cells by inhibition of DNA synthesis. Without an adequate supply of folate, DNA synthesis is limited by decreased purine and dTMP levels.
Folate exists in a pool of interconvertible intermediates, each carrying a 1-carbon fragment in several different oxidation states (Figure 4-2). The total body stores of folate is approximately 110 mg/70 kg, and approximately 420 μg/70 kg is lost each day via the urine and feces. A total of 2 different forms of folate are required for different aspects of nucleotide biosynthesis. N10-formyl THF provides the C-2 and C-8 carbons for the de novo synthesis of purine rings and, thus, is critical for DNA metabolism.
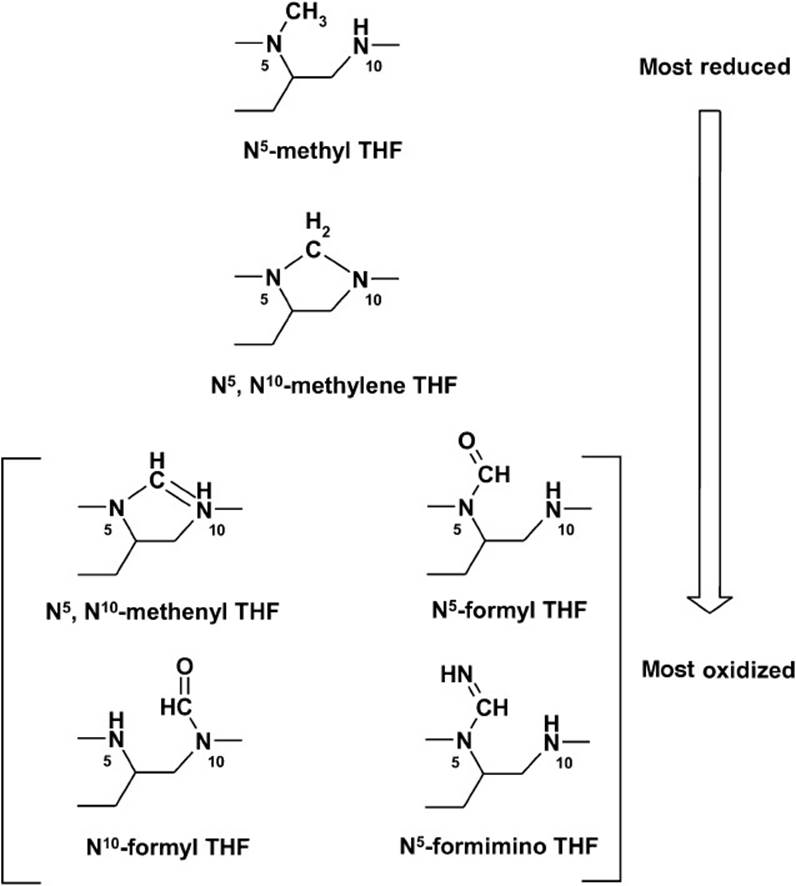
Figure 4-2. Structures of the various 1-carbon carriers of tetrahydrofolate (THF). THF can carry 1-carbon units in the oxidation states of methanol (N5-methyl THF), formaldehyde (N5, N10-methylene THF) or formic acid (remaining structures).
The methylene form, N5, N10-methylene THF, is required for the production of dTMP from dUMP. This reaction involves the transfer of a CH2 group and a hydrogen from N5, N10-methylene THF. In this process, THF is oxidized to dihydrofolate (DHF). For subsequent dTMP production, THF must be regenerated. THF is produced from DHF by the enzyme DHF reductase (DHFR) in a reaction requiring NADPH. DHFR is the target of methotrexate, an antifolate cancer chemotherapeutic, which, by limiting the available pool of N5, N10-methylene THF inhibits DNA synthesis in rapidly dividing cancer cells. Methotrexate therapy can produce adverse events resembling folate deficiency. In addition, bacterial DHFR is a target for antimicrobials.
Outside of DNA synthesis, folate plays a role in methylation metabolism. The major methyl donor is S-adenosyl methionine (SAM), which is required for many reactions. For example, SAM is needed for the production of norepinephrine from epinephrine and for DNA methylation, which can influence gene transcription. After methyl group transfer, SAM is converted to S-adenosyl homocysteine (SAH), which is hydrolyzed to homocysteine and adenosine. To restore the levels of methionine (an essential amino acid), homocysteine must be methylated (Figure 4-3). This reaction is dependent on N5-methyl THF and vitamin B12. Methionine levels can be limiting,making the availability of N5-methyl THF for conversion of homocysteine to methionine critical. Further, in the absence of B12, THF can be trapped in the N5-methyl THF form and thus be removed from the THF pool. This is referred to as the “methyl trap,” which can impact other areas of 1-carbon metabolism, such as dTMP production.
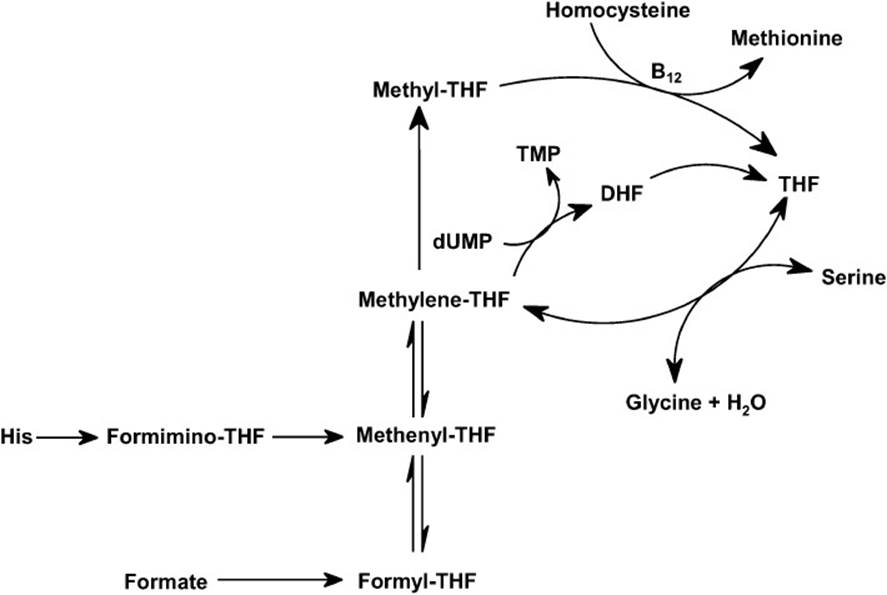
Figure 4-3. Reaction pathways showing the interconversion of 1-carbon carriers of tetrahydrofolate (THF). Note that all interconversions are reversible, except for the conversion of N5, N10-methylene THF to N5-methyl THF.
Folate deficiency perturbs DNA metabolism and methylation reactions. Leafy green vegetables are good sources of folate; however, folate is labile and may be damaged during food preparation. Another dietary source of folate is cereal products, especially breads and breakfast cereals that have been fortified with folic acid. Folate is also produced within the gut lumen by certain intestinal bacteria; however, the amount of folate absorbed from this source is minor in humans. In its simplest form, folate consists of 3 connected chemical moieties: a pteridine ring (6-methylpterin), p-aminobenzoic acid (PABA), and glutamate. In nature, folate is generally polyglutamated (decorated by two to seven additional glutamic acid residues). Conjugases (γ-glutamyl carboxypeptidases) in the intestinal lumen cleave off extra glutamic acid residue, and folate is absorbed by the mucosa of the small intestine (Figure 4-4). In cases of chronic alcoholism, folate deficiency may result from poor nutrition or from poor absorption of folate secondary to a conjugase deficiency. Once folate deficiency occurs, abnormal megaloblastic replication of epithelial mucosa can occur, which further impairs folate uptake.
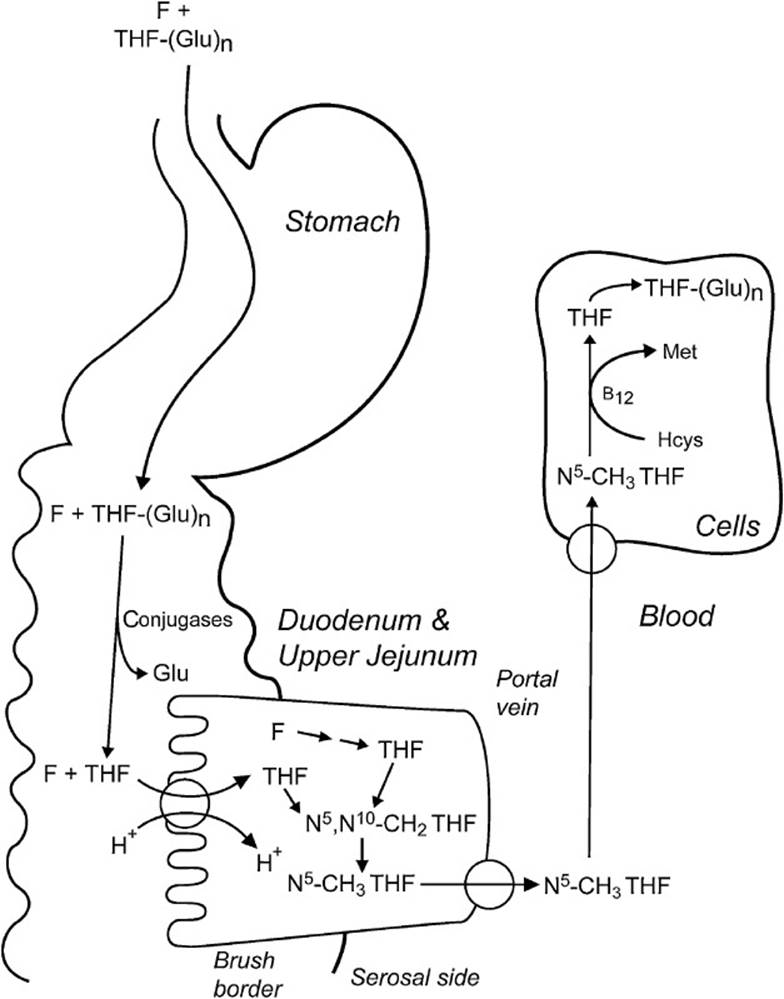
Figure 4-4. Intestinal absorption of dietary folates (THF-[Glu]n) and folic acid (F) from fortified cereal products and vitamin supplements. In the duodenum and upper jejunum, extra glutamate residue is cleaved by conjugases (γ-glutamyl carboxypeptidases). Both folate (F) and reduced folate (THF) are absorbed by a proton-coupled, high-affinity, folate transporter into the mucosal cell, converted to N5-methyl THF, and then exported into the portal circulation. N5-methyl THF is taken up into cells by facilitative diffusion, converted to THF by the B12-requiring methionine synthase, and then converted to a polyglutamate.
After absorption, folate is reduced to THF by dihydrofolate reductase. The majority of circulating folate is in the form of N5-methyl THF. Cells use specific transporters for THF uptake, and cellular machinery polyglutamates the folate to aid in cellular retention.
In summary, folate is a vitamin acquired from the diet essential for 1-carbon metabolism. Inadequate folate levels inhibit DNA synthesis by limiting purine nucleotide and dTMP levels, which results in the abnormal cellular proliferation observed in megaloblastic anemia. Folate is also required to replenish the methionine pool for SAM-dependent methylation reactions.
COMPREHENSION QUESTIONS
4.1 A 35-year-old woman is noted to have a hemoglobin level of 9 g/dL (normal range: 12-14 g/dL). The red cell size is enlarged. Which of the following tests would best help distinguish between a folate and vitamin B12deficiency?
A. Activity of methionine synthase
B. Blood level of cystathionine
C. Blood level of homocysteine
D. Blood level of methionine
E. Blood level of methylmalonate
4.2 A muscular 25-year-old man presents with dermatitis and an inflamed tongue. A history reveals that he has been consuming raw eggs as part of his training regimen for the past 6 months. Which of the following vitamins is most likely to be deficient in this patient?
A. Ascorbic acid (vitamin C)
B. Biotin
C. Cobalamin (vitamin B12)
D. Folic acid
E. Niacin (vitamin B3)
F. Pantothenic acid
G. Riboflavin (vitamin B2)
H. Thiamine (vitamin B1)
4.3 A 30-year-old man goes to his dentist complaining of loosening teeth. Examination also reveals his gums are swollen, purple, and spongy. The dentist also notes that the patient’s fingers have multiple splinter hemorrhages near the distal ends of the nail and that a wound on the patient’s forearm has failed to heal properly. Which of the following vitamins is most likely to be deficient in this patient?
A. Ascorbic acid (vitamin C)
B. Biotin
C. Cobalamin (vitamin B12)
D. Folic acid
E. Niacin (vitamin B3)
F. Pantothenic acid
G. Riboflavin (vitamin B2)
H. Thiamine (vitamin B1)
4.4 A female neonate is found to have a small spina bifida in her lower spinal column that could affect bladder and lower limb function. Which of the following vitamins is most likely to be deficient in this patient?
A. Ascorbic acid (vitamin C)
B. Biotin
C. Cobalamin (vitamin B12)
D. Folic acid
E. Niacin (vitamin B3)
F. Pantothenic acid
G. Riboflavin (vitamin B2)
H. Thiamine (vitamin B1)
ANSWERS
4.1 E. Vitamin B12 is a cofactor in 2 biochemical reactions, the conversion of homocysteine to methionine by the enzyme methionine synthase and the conversion of L-methylmalonyl-CoA to succinyl-CoA by methylmalonyl-CoA mutase. N5-methyl THF is a methyl donor in the methionine synthase reaction. Folate deficiency would result in decreased methionine synthase activity and decreases in methionine and cystathionine concentrations, while homocysteine levels would be increased. A vitamin B12 deficiency would also yield these same results, but, in addition, methylmalonate levels would increase as a consequence of a decrease in the activity of methylmalonyl-CoA mutase activity.
4.2 B. Raw eggs contain avidin, a protein that strongly binds biotin. Because native avidin is resistant to hydrolysis by digestive proteases, when it binds biotin it prevents its absorption. Avidin that has been denatured by cooking will be broken down during the digestive process. Biotin deficiency manifests itself as an erythematous, scaly skin eruption, and can also cause hair loss and conjunctivitis. Biotin deficiency can also occur following prolonged total parenteral nutrition if biotin is not supplemented.
4.3 A. The patient exhibits the classic symptoms of scurvy, a deficiency in vitamin C. In addition to being an important biologic antioxidant, ascorbic acid is required for the hydroxylation of proline and lysine residues of procollagen in the synthesis of collagen. A deficiency leads to defects in collagen synthesis, which adversely affects the intercellular cement substances in connective tissue, bones, and dentin.
4.4 D. The fetus needs a constant supply of cofactors for normal development. Folic acid supplements of 400 μg/day prior to conception have been shown to decrease the incidence of neural tube defects such as spina bifida.
BIOCHEMISTRY PEARLS
![]() Folate (folic acid) is an essential vitamin that, in its active form of tetrahydrofolate, transfers 1-carbon groups to intermediates in metabolism and plays an important role in DNA synthesis.
Folate (folic acid) is an essential vitamin that, in its active form of tetrahydrofolate, transfers 1-carbon groups to intermediates in metabolism and plays an important role in DNA synthesis.
![]() THF is necessary for the de novo synthesis of purines and the conversion of dUMP to dTMP.
THF is necessary for the de novo synthesis of purines and the conversion of dUMP to dTMP.
![]() The major metabolic perturbation in folate deficiency occurs in megaloblastic anemia.
The major metabolic perturbation in folate deficiency occurs in megaloblastic anemia.
REFERENCES
Devlin TM, ed. Textbook of Biochemistry with Clinical Correlations. 7th ed. New York: Wiley-Liss; 2010.
Frenkel EP, Yardley DA. Clinical and laboratory features and sequelae of deficiency of folic acid (folate) and vitamin B12 (cobalamin) in pregnancy and gynecology. Hematol Oncol Clin North Am. 2000;14(5):1079-1100.
Lin Y, Dueker SR, Jones AD, et al. Quantitation of in vivo human folate metabolism. Am J Clin Nutr. 2004;80(3):680-691.
Que A, et al. Identification of an intestinal folate transporter and the molecular basis for hereditary folate malabsorption. Cell. 2006;127(5):917-928.
Murray RK, Bender DA, Botham KM, et al, eds. Harper’s Illustrated Biochemistry. 29th ed. New York: Lange Medical Books/McGraw-Hill; 2012.