5 Steps to a 5 AP Psychology, 2014-2015 Edition (2013)
STEP 4. Review the Knowledge You Need to Score High
Chapter 13. Developmental Psychology
IN THIS CHAPTER
Summary: From the womb to the tomb, developmental psychologists are interested in how we grow up and how we grow old. Developmental psychology is the study of physical, intellectual, social, and moral changes across the life span from conception to death. Developmental psychologists attempt to describe, explain, and predict age-related behaviors.
In this chapter we look at theories proposed by developmental psychologists in each of the four broad topic areas across the periods of infancy, childhood, adolescence, and adulthood.

Key Ideas
![]() Nature vs. Nurture
Nature vs. Nurture
![]() Continuity vs. Discontinuity
Continuity vs. Discontinuity
![]() Stability vs. Change
Stability vs. Change
![]() Research designs—longitudinal, cross-sectional, cohort-sequential, retrospective
Research designs—longitudinal, cross-sectional, cohort-sequential, retrospective
![]() Physical development
Physical development
![]() Cognitive development
Cognitive development
![]() Moral development
Moral development
![]() Social development
Social development
![]() Emotional development
Emotional development
![]() Gender roles and sex differences
Gender roles and sex differences
Key Issues in Development
Nature vs. Nurture
For thousands of years, philosophers and psychologists took sides in the nature versus nurture controversy, dealing with the extent to which heredity and the environment each influences behavior. Today, psychologists agree that both nature and nurture interact to determine behavior, but they disagree as to the extent of each. Many biological psychologists, neuroscientists, and evolutionary psychologists argue the nativist (nature) position that basic structures for our behavior are genetically determined, and their expression depends on interaction with the environment. In other words, development results mostly from genetically determined maturation—biological growth processes that bring about orderly changes in behavior, thought, or physical growth, relatively unaffected by experience. On the other side, behaviorists argue that physical structures are genetically inherited and intellectual structures are learned; the environment shapes us. Developmental psychologists conduct experimental and observational studies on identical twins, for example, to try to determine the relative contributions of nature and nurture. (See Genetics and Behavior in Chapter 7.)
Continuity vs. Discontinuity
A second controversy, continuity versus discontinuity, deals with the question of whether development is gradual, cumulative change from conception to death (continuity), or a sequence of distinct stages (discontinuity). Behaviorists who favor continuity focus on quantitative changes in number or amount, such as changes in height and weight. Vygotsky favored continuity. On the other hand, theorists such as Piaget, Kohlberg, Gilligan, and Erikson who favor distinct stages focus on qualitative changes in kind, structure, or organization. They theorize that the child and growing adult resolve conflicts or develop different abilities in stages through which everyone passes in the same order and that build upon one another; the growth pattern is discontinuous.
Stability vs. Change
A third controversy, stability versus change, deals with the issue of whether or not personality traits present during infancy endure throughout the lifespan. Psychoanalysts, followers of Freud, believe that personality traits developed in the first 5 years predict adult personality. Change theorists argue that personalities are modified by interactions with family, experiences at school, and acculturation. Developmental psychologists research which characteristics are most likely to remain stable and consistent, and which are likely to be more flexible and subject to change. Some aspects of temperament, such as energy level and outgoingness, seem relatively stable, whereas social attitudes are more likely to change.
Methods of Studying Development
Developmental psychologists conduct experiments, naturalistic observations, correlational studies, and case studies that enable them to assess change over time. (See Chapter 6, Research Methods.) They use four basic research designs: longitudinal, cross-sectional, cohort-sequential, and retrospective studies.
Longitudinal Studies
A longitudinal study follows the same group of people over a period of time from months to many years in order to evaluate changes in those individuals. In 1921, Lewis Terman of Stanford University began studying a group of highly intelligent children who have been studied throughout their lives, providing important information about changes in intellectual functioning across the lifespan. Longitudinal studies can be extremely costly to conduct, take a long time to produce results, and typically lose participants over time. If those who drop out differ from the other subjects in significant ways, results of the study may not be generalizable to the original population.
Cross-Sectional Studies
On the other hand, cross-sectional studies cost less, do not lose participants, and produce results quickly, but they have other major weaknesses. In a cross-sectional study, esearchers assess developmental changes with respect to a particular factor by evaluating different age groups of people at the same time. For example, to study lifespan changes in mathematical skills, psychologists could give the same math tests to groups of 15-, 25-, 35-, 45-, 55-, 65-, and 75-year-olds at the same time. Cross-sectional studies can be invalid if a cohort, group of people in one age group, is significantly different in their experiences from other age groups, resulting in the cohort effect, differences in the experiences of each age group as a result of growing up in different historical times. This difference is a confounding variable in the study. Obviously, most younger participants may have been exposed to calculators and computers their whole lives, whereas 65- and 75-year-olds have had fewer opportunities.
Cohort-Sequential Studies
To minimize the major drawbacks of both longitudinal and cross-sectional research designs, some researchers conduct cohort-sequential studies. In cohort-sequential studies, cross-sectional groups are assessed at least two times over a span of months or years, rather than just once. Results from one cohort are compared with other cohorts at the same age to evaluate their similarity; differences indicate a cohort effect. In this way, researchers can separate age-related changes from cohort effects. These studies share disadvantages of longitudinal research, but to a lesser extent.
Retrospective Studies
Biographical or retrospective studies are case studies that investigate development in one person at a time. Typically, a researcher interviews an individual at the older end of the age span of interest. The researcher reconstructs changes that have occurred in the subject’s life through the subject’s self-reports in interviews and examination of available data. Although these studies can be very detailed, they are not always correct because memory is not always accurate, and they may not be generalizable to a larger population.
Physical Development
Physical development focuses on maturation and critical periods. A critical period is a time interval during which specific stimuli have a major effect on development that the stimuli do not produce at other times.
Prenatal Development
Prenatal development begins with fertilization, or conception, and ends with birth. The zygote is a fertilized ovum with the genetic instructions for a new individual normally contained in 46 chromosomes. (See Genetics and Behavior in Chapter 7.) During the first 2 weeks following conception, the zygote divides again and again forming first a hollow ball of cells that buries itself in the wall of the uterus and then a three-layered inner cell mass surrounded by outer cells attached to the uterine lining. Different genes function in cells of the three different layers; the forming individual is now considered an embryo. During the embryonic period from the third through the eighth weeks following conception, organs start to develop as a result of differentiation and specialization of cells; and the placenta, umbilical cord, and other structures form from the outer cells. As organs develop, the embryo is particularly sensitive to environmental stimuli such as chemicals and viruses. Nutrients, oxygen, wastes, and other substances pass from the woman’s blood into and out of the developing organism through the placenta. By the end of the eighth week, the embryo has a head with partially formed eyes, limbs, and a skeleton composed of cartilage. At this point, all organs are present in rudimentary form, and the developing individual begins to resemble a human; it is a fetus, the developing human organism from about 9 weeks after conception to birth. During the fetal period, the organ systems begin to interact, bone replaces cartilage in the skeleton, and sex organs and sense organs become more refined.
Birth Defects
Birth defects can result from a malfunctioning gene or an environmental stimulus. If the pregnant woman takes in poisonous chemicals or gets infected with a virus, developmental errors can result in birth defects that are not hereditary. Chemicals such as alcohol, drugs, tobacco ingredients, mercury, lead, cadmium, and other poisons; or infectious agents, such as viruses, that cause birth defects are called teratogens. The specific nature of a birth defect depends on which structures are developing at the time of exposure. Most birth defects develop during the embryonic period and are usually more severe than problems that develop later. The critical period for eyes, ears, arms, legs, and the heart is typically the first 3 months (first trimester) of pregnancy, while the critical period for damage to the reproductive system extends across the first and second trimesters of pregnancy. The critical period for the nervous system is all three trimesters. Because of the long critical period for brain development, many kinds of brain damage can result, the most severe during the embryonic and early fetal periods.
Fetal alcohol syndrome (FAS) is a cluster of abnormalities that occurs in babies of mothers who drink alcoholic beverages during pregnancy. Low intelligence, a small head with flat face, misshapen eyes, a flat nose, and thin upper lip characterize children with FAS. Intellectual impairment ranges from minor learning disabilities to severe mental retardation. The more severe mental retardation results from exposure of the embryo/fetus during the early months of pregnancy. Currently, FAS is the leading cause of mental retardation in the United States. Cigarette smoking during pregnancy is associated with miscarriage, stillbirth, premature delivery, and low birth weight. Heroin- and cocaine-exposed fetuses that are born live may undergo withdrawal symptoms, and may be distractable and unable to concentrate. Researchers have difficulty pinpointing other prenatal effects of cocaine and heroin because affected babies are often exposed to additional substances and situations that can account for other symptoms.
Malnutrition, as well as prescription and over-the-counter drugs, can cause birth defects. Even certain nutrients ingested in large quantities can be teratogenic. For example, high doses of vitamin A can cause heart, nervous system, and facial defects. Viruses such as rubella can pass into the placenta and cause birth defects. During the first trimester of pregnancy, rubella can cause cataracts, deafness, and heart defects; during later weeks effects include learning disabilities, speech and hearing problems, and Type 1 diabetes.
Behavior of the Neonate
At birth, neonates, or newborn babies, are equipped with basic reflexes that increase their chances of survival. A sequence of rooting, sucking, and swallowing reflexes enables the neonate to get food. Rooting is the neonate’s response of turning his or her head when touched on the cheek and then trying to put the stimulus into his or her mouth. What touches the newborn’s cheek is frequently a nipple. Sucking is the automatic response of drawing in anything at the mouth. Swallowing is a contraction of throat muscles that enables food to pass into the esophagus without the neonate choking. The lack of some reflexes in a neonate can indicate possible brain damage to neuropsychologists. Among those they test are the grasping reflex, when the infant closes his/her fingers tightly around an object put in his/her hand, and the Moro or startle reflex, in which a loud noise or sudden drop causes the neonate to automatically arch his/her back, fling his/her limbs out, and quickly retract them. As the infant matures, developing voluntary control over behaviors, many of the reflexes disappear.
Neonates’ adaptive behavior is not limited to reflexes; they also show behaviors that facilitate social interactions. Shortly after birth, infants respond to the human face, voice, and touch. They show a preference for the voice and odor of their mothers. Their vision is best for objects normally about the distance from the infant’s eyes to the caretaker’s face. They can track objects with their eyes when they are only a few days old. Infants can distinguish among different colors, and they prefer certain complex patterns, such as the human face. Newborns also prefer sweet and salty tastes. Their sense of hearing is well developed at birth and typically the dominant sense during the baby’s first months. As structures in the eye and brain develop during infancy, visual acuity (clarity of vision) and depth perception improve, so that sight normally becomes a more dominant sense sometime during the second half of the baby’s first year.
How do psychologists know this information if babies can’t talk? Psychologists depend on gazes, sucking, and head turning measured by sophisticated computerized equipment in response to changes in stimuli to reveal abilities of infants. For example, when infants are shown a stimulus for the first time, they gaze at it for a length of time. With repeated presentations of that stimulus, they look away sooner. If a new stimulus is presented, and the infant can remember and discriminate between the two stimuli, the infant will look at the new stimulus longer than if he or she perceives no difference between the first and second stimulus. These are called habituation studies. Habituation is decreasing responsiveness with repeated presentation of the same stimulus.
The First Two Years
An infant’s physical development during the first two years is amazing. Brain development proceeds rapidly from the prenatal period, during which about 20 billion brain cells are produced, through the baby’s first two years, during which dendrites proliferate in neural networks, especially in the cerebellum, then in occipital and temporal lobes as cognitive abilities grow. Body proportions change as the torso and limbs grow more quickly, so that the head is less out of proportion to body size. Physical development of the musculoskeletal system from head to tail, and from the center of the body outward, accompanies nervous system maturation to enable the baby to lift its head, roll over, sit, creep, stand, and walk, normally in that order. Maturation, motor and perceptual skills, motivation, and environmental support all contribute to development of new behaviors. During childhood, proliferation of dendrites proceeds at a rapid rate, especially in the frontal cortex.
Adolescence
The next growth spurt comes in adolescence, following a dramatic increase in production of sex hormones. The defining feature of puberty is sexual maturation, marked by the onset of the ability to reproduce. Primary sex characteristics, reproductive organs (ovaries and testes) start producing mature sex cells, and external genitals (vulva and penis) grow. So do secondary sex characteristics—nonreproductive features associated with sexual maturity—such as widening of hips and breast development in females, growth of facial hair, muscular growth, development of the “Adam’s apple,” and deepening of the voice in males, and growth of pubic hair and underarm hair in both. Girls begin their growth spurt about two years before their first menstrual period (menarche), typically at age 12½. Early maturation of females can put them at a social disadvantage, whereas early maturation of males can put them at a social advantage. Boys start their growth spurt about two years later than girls, but about two years before ejaculation of semen with viable sperm. During adolescence, changes in the brain include selective pruning of unused dendrites with further development of the emotional limbic system, followed by frontal lobe maturation.
Aging
By our mid-20s, our physical capabilities peak, followed by first almost imperceptible, then accelerating, decline. According to evolutionary psychologists, peaking at a time when both males and females can provide for their children maximizes chances of survival for our species. Decreased vigor, changes in fat distribution, loss of hair pigmentation, and wrinkling of the skin are changes associated with advances in age. In females at about age 50, menopause—cessation of the ability to reproduce—is accompanied by a decrease in production of female sex hormones. Men experience a more gradual decline in reproductive function as they age. Typically, as adults age, the lenses of their eyes thicken, letting less light reach the retina and worsening vision for near objects; ability to detect high-pitched sounds decreases; and sensitivity to tastes, odors, and temperature may decrease. Neural processes slow and parts of the brain begin to atrophy. Physical signs of aging can be slowed, and to some extent reversed, if we stay physically and mentally active and have a healthy diet. Heart disease, stroke, cancer, Alzheimer’s, and other degenerative diseases are often terminal diseases of old age. Since they do not interfere with reproductive success, genes involved in these diseases do not incur any selective pressures. On average, men die about four years earlier than women.
Theories of Cognitive Development
Theories of cognitive development look at how our patterns of thinking, reasoning, remembering, and problem solving change as we grow. Most developmental theories focus on infancy, childhood, and adolescence.
Jean Piaget’s Theory of Cognitive Development
Swiss psychologist Jean Piaget developed a stage theory of cognitive development based on decades of careful observation and testing of children. His theory has been very influential because Piaget recognized that children think differently from adults. He thought that certain cognitive structures were innate, but only through a child’s interaction with the environment could they grow and develop over time.
Piaget believed that all knowledge begins with building blocks called schemas, mental representations that organize and categorize information processed by our brain. Through the process of assimilation, we fit new information into our existing schemas. Through the process of accommodation we modify our schemas to fit new information. As babies, we learn through accommodation that not all people fit our schema of mommy.
Sensorimotor (First) Stage
Piaget called the first stage of cognitive development, from birth to approximately age 2, the sensorimotor stage, during which the baby explores the world using his or her senses and motor interactions with objects in the environment. The concept of object permanence—that objects continue to exist even when out of sight—to Piaget seemed to develop suddenly between 8 and 10 months. Piaget said that the 5-month-old who sees a toy does not search for it if it disappears, but a 9-month-old does. Recently, psychologists have found that object permanence seems to develop gradually; young infants gaze where they saw a toy that disappeared. According to Piaget, infants at about 8 months of age also seem to develop stranger anxiety, fear of unfamiliar people, indicating that they can differentiate among people they know and people they don’t know.
Preoperational (Second) Stage
To Piaget, attainment of object permanence and stranger anxiety indicated that cognitive structures had matured sufficiently for the typical 2-year-old to represent and manipulate objects with symbols such as words, whether or not the objects were present, which characterizes Piaget’s second stage, the preoperational stage. From approximately age 2 to age 7, language develops with the ability to think. The child is mainly egocentric, seeing the world from his or her own point of view. Egocentrism is consistent with a belief called animism, that all things are living just like him or her; and the belief, called artificialism, that all objects are made by people. While preoperational, a child uses trial and error to figure out how things work and answers questions intuitively rather than logically. He or she sometimes demonstrates magical thinking, reasoning that something happens because he or she wishes it to happen.
Concrete Operational (Third) Stage
During Piaget’s third stage, the concrete operational stage, children between ages 7 and 12 develop simple logic and master conservation concepts, that changes in the form of an object do not alter physical properties of mass, volume, and number. For example, 12 ounces of juice in a tall, thin glass isn’t more than 12 ounces of juice in a short, fat glass. The child now can logically classify objects into categories mentally. Mathematically and logically, the concrete operational child recognizes reversibility (transformations), for example that 3 + 4 = 4 + 3.
Formal Operational (Fourth) Stage
According to Piaget, after about age 12, children reason like adults in the fourth stage, the formal operational stage. In this stage, youngsters are able to think abstractly and hypothetically. They can manipulate more information in their heads and make inferences they were unable to make during the previous stage. Teens are able to consider questions involving abstract concepts, such as truth and justice. Some believe that the ability to think abstractly decreases in older adults partially because these skills are not utilized as often.
Piaget emphasized that increases in reasoning skill over time were punctuated by shifts in perspective, which were qualitative from one stage to the next. For example, in moving from the preoperational stage to the concrete operational stage, children decenter their perspective from egocentric to taking other people’s perspectives. With more experience, concrete operational thinkers cognitively reorganize their thinking to become the abstract thinkers of the formal operational stage. Although psychologists agree with the sequence of cognitive development steps and milestones proposed by Piaget, critics fault him for not acknowledging that children go through the stages at different rates, often more quickly than he predicted, and for not understanding that change is more gradual and continuous.
Vygotsky’s Sociocultural Theory of Cognitive Development
Whereas Piaget emphasized maturation (nature) and development in stages (discontinuity), Russian psychologist Lev Vygotsky emphasized the role of the environment (nurture) and gradual growth (continuity) in intellectual functioning. Vygotsky thought that development proceeds mainly from the outside in by the process of internalization, absorbing information from a specified social environmental context. Children learn from observing the interactions of others and through their own interactions within the environment. Vygotsky’s sociocultural theory of cognitive development assigns a significant role to mentors such as parents, teachers, and other students. A key concept is his zone of proximal development (ZPD), the range between the level at which a child can solve a problem working alone with difficulty, and the level at which a child can solve a problem with the assistance of adults or more-skilled children. Working close to the upper limit of a child’s capability, the instructor and child work closely together to reach that goal, and then through continued practice, the child is able to attain it more and more independently. When the goal is achieved without help, then that goal becomes the lower limit for a new ZPD. Both Piaget and Vygotsky have influenced the ways that teachers are trained to help children learn.
Cognitive Changes in Adults
Piaget did not study changes in cognition as adults age. Adult thought is frequently richer and more adaptive than adolescent thought. Middle-aged adults tend to reason more globally and make more rational decisions than younger people. Gerontologist Warner Schaie has found that while fluid intelligence—those abilities requiring speed or rapid learning—generally diminishes with aging, crystallized intelligence—learned knowledge and skills such as vocabulary—generally improves with age (at least through the 60s). In situations that access their skills and long-term memories, older adults may show superior functioning to younger people. Decline in mental abilities can be slowed if we stay healthy, live in a favorable environment, engage in stimulating activities, are flexible, have a mentally able partner, maintain perceptual processing speed, and feel satisfied with our earlier accomplishments. Alzheimer’s disease, a fatal degenerative disease in which brain neurons progressively die—causing loss of memory, reasoning, emotion, control of bodily functions, then death—strikes 3% of the world’s population by age 75. Strokes, brain tumors, and alcoholism can result in dementia, the loss of mental abilities.
Theories of Moral Development
Moral development refers to growth in the ability to tell right from wrong, control impulses, and act ethically. Lawrence Kohlberg, like Piaget, thought that moral thinking develops sequentially in stages as cognitive abilities develop. Kohlberg examined moral development by asking boys, male adolescents, and men how they would solve hypothetical moral problems, the most famous one dealing with Heinz, who must decide whether or not to steal a scarce drug he is unable to pay for in order to possibly save his wife’s life. Kohlberg analyzed the reasoning subjects used to arrive at their answers. Kohlberg concluded that our moral reasoning develops from simple and concrete to more abstract and principled. He suggested three basic levels of moral development consisting of two stages each.
• When at the preoperational stage of cognitive development, children tend to be at the preconventional level of morality, in which they do the right thing to avoid punishment (stage 1), or to further their self-interests (stage 2).
• When at the concrete operational stage of cognitive development, people tend to move on to the conventional level of morality, in which they follow rules to live up to the expectations of others, “good boy/nice girl” (stage 3), or to maintain “law and order” and do their duty (stage 4). Most teenagers and adults think morally at the conventional level.
• Some people who are in the formal operational stage of cognitive development progress to Kohlberg’s third or postconventional level of morality, in which they evidence a social contract orientation that promotes the society’s welfare (stage 5), or evidence an ethical principle orientation that promotes justice and avoids self-condemnation (stage 6).
Studies by other researchers show the same sequence of stages in moral development for stages 1 through 4. According to cross-cultural studies, people in individualistic societies, such as North Americans and Europeans, are more likely to show Kohlberg’s postconventional morality than those in collectivistic societies who value community standards over personal standards.
Applying Kohlberg’s scale to women, Carol Gilligan found that women rarely reach the highest stages of morality because they think more about the caring thing to do or following an ethic of care, rather than what the rules allow or following an ethic of justice. She asserted that women are not morally inferior, just different. Subsequent studies by other researchers have found that both men and women use both justice and care dimensions in their moral reasoning. Other critics point out that people are often inconsistent in their moral reasoning, even when dealing with their own moral dilemmas. They also suggest that since both cultural factors and cognitive factors influence moral development, moral ideals are not universal.
Theories of Social and Emotional Development
Theories of social development look at the influence of others on the development of a person. Others include members of the family and other caregivers, peers, and even culture, which consists of the behaviors, ideas, attitudes, and traditions transmitted from one generation to the next within a group of people who share the same language and environment.
Interactions Between Babies and Parents
Interactions aren’t objective; they involve emotions. Bonding is the creation of a close emotional relationship between the mother (or parents) and baby shortly after birth.
Attachment
As the mother (or other caregiver) bonds with the infant, through frequent interactions, the infant gradually forms a close emotional relationship with his or her mother (or other care-givers), a process called attachment. A half century ago, developmental psychologists thought that babies became attached to the caregiver who fed them. Harry Harlow’s experimental research with monkeys disproved that belief when he found that baby monkeys separated from their mothers preferred to spend time with and sought comfort from a soft cloth-covered substitute (surrogate) rather than a bare wire substitute with a feeding bottle. More recent research has revealed that human infants become attached to familiar care-givers, usually parents, who not only provide them with nourishment, but also a soft, warm, reassuring environment where the baby feels safe and secure.
Secure and Insecure Attachment
Mary Ainsworth studied attachment using a “strange situation” where a mother and baby play in an unfamiliar room, the baby interacts with the mother and an unfamiliar woman, the mother leaves the baby with the other woman briefly, the baby is left alone briefly, then the mother returns to the room. A majority of babies played happily when their mothers were present, explored their environment and returned to their mothers periodically, and, when their mothers returned after an absence, they were happy to see them and receptive to their contact, displaying secure attachment. The mothers were generally sensitive and responsive to their babies’ needs. On the other hand, some babies showed insecure attachment. When their mothers were present, they avoided or ignored them, and were upset when they left, but were angry and rejected them when they returned, or they behaved inconsistently. Securely attached babies tend to become socially competent children.
Temperament
The baby’s temperament, or natural disposition to show a particular mood at a particular intensity for a specific period, affects his or her behavior. Both the infant’s heredity and his or her intrauterine environment affect whether the neonate is easy or difficult. Easy babies are cheerful, relaxed, and follow predictable patterns of eating and sleeping, while difficult babies are irritable, intense, and unpredictable. In general, easy babies tend to become sociable children, and difficult babies tend to become less sociable children. How the primary caregiver responds to the baby affects how the baby will react to an extent. Jerome Kagan showed that shy, inhibited babies can become more relaxed and less fearful with responsive parenting.
Awareness of Self and Others
Becoming aware of ourselves and others is crucial to social development. Self-awareness, consciousness of oneself as a person; and social referencing, observing the behavior of others in social situations to obtain information or guidance, both develop between ages 1 and 2. The “rouge test,” in which a red spot is secretly put on a baby’s nose, then the baby is placed in front of a mirror to see if the baby realizes it is his or her own nose with the red spot, has revealed that self-awareness typically develops at age 1½.
“So that you don’t get authoritarian and authoritative parenting mixed up, remember authoritarian is like totalitarian (that we learned about in social studies). Both authoritarians and totalitarians exercise complete control and authority over people’s lives.”
— Shereen, AP student
Parenting Styles
Diana Baumrind studied how parenting styles affect the emotional growth of children. Authoritarian parents set up strict rules, expect children to follow them, and punish wrongdoing. In contrast, more democratic authoritativeparents set limits, but explain the reasons for rules with their children, and make exceptions when appropriate. Permissive parents tend not to set firm guidelines, if they set any at all. They tend to be more responsive than demanding. Uninvolved parents make few demands, show low responsiveness, and communicate little with their children. While these parents fulfill the children’s basic needs, they are generally detached from their children’s lives. In extreme cases, these parents may even reject or neglect the needs of their children. Baumrind and other researchers found that for European and American families, the most self-reliant, socially competent children with the highest self-esteem have warm, authoritative parents. Since these findings come from correlational studies, they do not establish cause and effect.
Erikson’s Stage Theory of Psychosocial Development
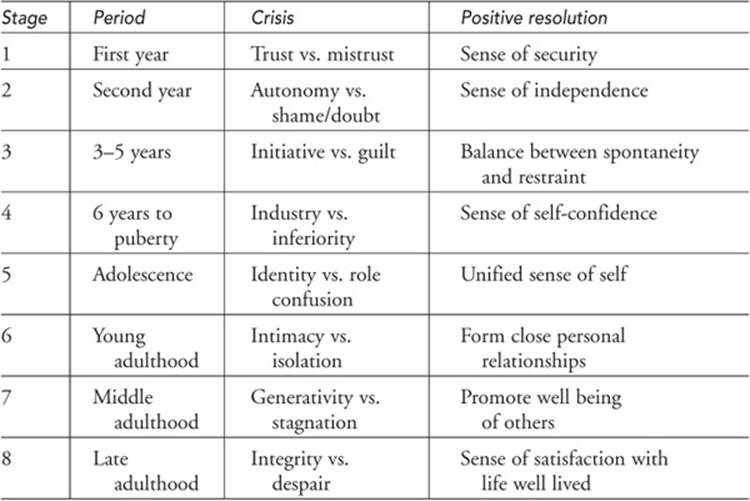
Parents are not the only people who interact with children; each stage of development requires a new level of social interaction. Starting with kindergarten, frequent peer interactions become more complex and structured and lead to friendships. Peer interactions help children develop social skills such as cooperation, empathy, and self-regulation. Erik Erikson was an influential theorist partly because he examined development across the life span in a social context, rather than just during childhood, recognizing that we continue to grow beyond our teenage years, and our growth is influenced by others. His stage theory of psychosocial development identifies eight stages during which we face an important issue or crisis. How we resolve each crisis shapes our personality and affects our relationships with others.
• Stage One: Infants (newborn to 1 year old) face the crisis of trust vs. mistrust. Parents must provide a safe, consistent, and loving environment for children to leave this stage healthily with a strong trust that others care and will always be there for them. Mistrust, based on inconsistent, cold, or abusive situations, prevents children from leaving this stage ready to form lasting and close relationships in the future.
• Stage Two: Toddlers (2 years old) face the crisis of autonomy vs. shame and doubt. The nickname “terrible twos” comes from children’s needs to develop self-control and do things for themselves, which can often result in spills, falls, wetting, and other accidents. Children who are encouraged to try new skills develop autonomy, while those who are ridiculed or overprotected may doubt their abilities and feel ashamed of their actions.
• Stage Three: Children (3–5 years of age) face the crisis of initiative vs. guilt. Children need to learn to make plans and carry out tasks through play, asking questions, making choices, and using their imaginations to develop initiative. If they are severely criticized, discouraged from asking questions, not permitted to make choices, or prevented from playing, children feel guilty.
• Stage Four: School-aged children (6–12 years of age) face the crisis of industry vs. inferiority. Children need to be positively reinforced for productive activities, such as achieving in the classroom, on the sports field, or artistically or musically, in order to develop a healthy self-concept and a sense of industry. If children’s efforts are considered inadequate, feelings of social or mental inferiority in this stage can carry over to a poor self-concept in the future.
• Stage Five: The crisis of stage five for adolescents (about 12–20 years of age) is identity vs. role confusion. Answering the question, “Who am I?” is the major task, which involves building a consistent identity, a unified sense of self. Failure of teens to achieve a sense of identity results in role confusion and uncertainty about who they are and where they are going.
• Stage Six: Young adults (about 21–40 years of age) face the crisis of intimacy vs. isolation. Intimacy involves deeply caring about others and sharing meaningful experiences with them, especially a life partner. Without intimacy, people feel alone and uncared for in life; they experience isolation.
• Stage Seven: In middle adulthood (about 40–65 years of age), the crisis is generativity vs. stagnation. During this period, adults need to express their caring about the next and future generations by guiding or mentoring others or producing creative work that enriches the lives of others. People who fail to achieve generativity can become stagnant and preoccupied with their own needs and comforts.
• Stage Eight: In late adulthood (about age 65 to death), the crisis is integrity vs. despair. Those who look back on their lives with satisfaction that they have lived their lives well develop a sense of wholeness and integrity. Those in despair look back with regrets and disappointment in the lives they’ve led.
Erikson’s theory most accurately describes development in individualistic societies.
Middle Age and Death
Daniel Levinson described a midlife transition period at about age 40, seen by some as a last chance to achieve their goals. People who experience anxiety, instability, and change about themselves, their work, and their relationships during this time have a challenging experience sometimes termed the mid-life crisis.
Death marks the end of life. Psychiatrist Elisabeth Kubler-Ross’ studies of death and dying have focused attention on the end of life, encouraging further studies of death and dying, and growth of the hospice movement that treats terminal patients and their families to alleviate physical and emotional pain. Based on her observations and interviews with hundreds of dying hospital patients, Kubler-Ross concluded that terminally ill patients pass through five stages of coping: denial, anger, bargaining, depression, and acceptance. Subsequent research has revealed that not all terminal patients pass through all of the stages nor do they necessarily go through the stages in the order indicated.
Gender Roles and Sex Differences
The first thing many people ask when they hear about the birth of a baby is, “Is it a boy or a girl?” Gender matters. Gender is the sociocultural dimension of being biologically male or female. We have different expectations for boys and girls. Gender roles are sets of expectations that prescribe how males and females should act, think, and feel. Gender identity is our sense of being male or female, usually linked to our anatomy and physiology.
• The Biological Perspective. The biological perspective attributes differences between the sexes to heredity. Males have 44 chromosomes, plus sex chromosomes X and Y. Females have 44 chromosomes, plus sex chromosomes X and X. The sex chromosomes determine the anatomical differences between the sexes. The Y chromosome contains the instructions for the growth of male sex organs and synthesis of male sex hormones. Male sex hormones influence brain development. Typically, the female’s corpus callosum is larger than males’, which might influence lateralization in the brain. Hormonal differences at puberty not only influence boys’ greater height, but also their added musculature and more aggressive tendencies.
• The Evolutionary Perspective. According to the evolutionary perspective, our behavioral tendencies prepare us to survive and reproduce. Males are more likely than females to be risk takers, show dominance, and achieve high status. Females are more likely to be concerned with their appearance in order to attract high-status, protective males.
• The Psychoanalytic Perspective. According to Freud’s psychoanalytic perspective, young girls learn to act feminine from their mothers, and young boys learn to act masculine from their fathers when they identify with their same-sex parent as a result of resolving either the Electra or Oedipal complex at about age 5.
• The Behavioral Perspective. According to (the behavioral perspective) social learning theory, children respond to rewards and punishments for their behavior, and they observe and imitate significant role models, such as their parents, to acquire their gender identity.
• The Cognitive Perspective. According to the cognitive perspective, children actively engage in making meaning out of information they learn about gender. Sandra Bem’s gender schema theory says that children form a schema of gender that filters their perceptions of the world according to what is appropriate for males and what is appropriate for females. Bem acknowledges that social learning contributes to her cognitive developmental theory. Gender role stereotypes, which are broad categories that reflect our impressions and beliefs about males and females, have typically classified instrumental traits, such as self-reliance and leadership ability, as masculine and expressive traits, such as warmth and understanding, as feminine. Rather than seeing masculinity and femininity as alternatives, many psychologists now recognize androgyny, the presence of desirable masculine and feminine characteristics in the same individual.
Set Differences in Cognition
Meta-analysis of research on gender comparisons indicates that, for cognitive skills, the differences within either gender are larger than the differences between the two genders. Males tend to have better ability to perform mental rotation tasks. The only evidence that males show higher achievement in mathematics than females is on the math section of the SAT; females receive higher grades in mathematics courses than males. Recent findings suggest that females who get better grades in high school and college may test more poorly because of a phenomenon known as stereotype threat, anxiety that influences members of a group concerned that their performance will confirm a negative stereotype. According to Claude Steele, when they know that their performance is being compared to that of males, girls tend to do less well than if they are not being compared.
![]() Review Questions
Review Questions
Directions: For each question, choose the letter of the choice that best completes the statement or answers the question.
1. What is the response pattern of securely attached children in the Strange Situation when their mothers return?
(A) They tend to ignore their mothers because they are secure about her care.
(B) Sometimes they run over to their mothers and sometimes they do not; there’s no consistent pattern in their responses.
(C) They tend to run over to their mothers and beg them not to leave again.
(D) They tend to go to their mothers for comfort.
(E) They hit their mothers.
2. In the nature versus nurture controversy, “nature” refers to
(A) heredity
(B) plants and animals
(C) all living things we interact with
(D) constituents of the problem
(E) the environment
3. Researchers were interested in studying the effects of divorce on children. Their study included 250 4-year-olds. Interviews and family observations were conducted 6 months, 2 years, 5 years, and 10 years after the initial interviews and observations. Which method did the researcher use?
(A) cohort sequential
(B) cross-sectional
(C) longitudinal
(D) experimental
(E) quasi-experimental
4. Object permanence is
(A) the belief that all objects have life just like humans do
(B) the idea that gender does not change by putting on the clothes of the opposite sex
(C) the understanding that a tall beaker and a short beaker can hold the same amount of water
(D) a belief that all objects in the world, including mountains and streams, are made by people
(E) the understanding that things continue to exist even when they are out of sight
5. The rooting reflex is a neonate’s tendency to
(A) open its mouth and turn its head when touched on the cheek
(B) throw out its arms and legs and quickly retract them when startled
(C) explore the world through sucking objects
(D) look longer at round shapes that look like faces than square shapes that do not
(E) grasp nearby objects
6. Dorothy just celebrated her 90th birthday with her close friends, and is excited about a visit from her grandchildren. According to Erikson, she has probably most recently achieved
(A) isolation
(B) integrity
(C) despair
(D) autonomy
(E) industry
7. Mr. Hernandez explains to his son that the speed limit is 55 mph. He tells him to stay under the speed limit when driving because it’s the law and will probably prevent accidents. Kohlberg’s level of morality illustrated by this example is
(A) preconventional
(B) concrete operational
(C) conventional
(D) egocentric
(E) postconventional
8. A critical period is a stage in development when
(A) specific stimuli have a major effect on development that they do not produce at other times
(B) children are resistant to any kind of discipline by their parents
(C) new learning is prevented by older learning
(D) bonding between the child and parent first takes place
(E) the child first enters elementary school and needs positive reinforcement
9. Which of the following is a similarity between the cognitive developmental theory of Piaget and the moral developmental theory of Kohlberg?
(A) Both theories stress the importance of changes in thinking in their stages.
(B) Both believe personality is formed in the first 5 years.
(C) Both theories stress the importance of the third stage in the developmental process.
(D) Both developed a life span theory and had eight stages.
(E) Both believe that libido fixated in childhood cannot be changed.
10. Harlow’s experiment with rhesus monkeys and surrogate mothers emphasized the importance of
(A) contact comfort
(B) feeding
(C) aesthetic needs
(D) incentive theory
(E) gender schema
11. According to Diana Baumrind, which of the following parental styles results in the most socially competent and responsible adults?
(A) authoritarian
(B) authoritative
(C) uninvolved
(D) permissive
(E) indulgent
12. The child was born with widely spaced eyes, a thin upper lip, and a short flat nose. Chances are that he will later suffer from mental retardation. To which teratogen was this child most likely exposed during the prenatal period?
(A) tobacco
(B) German measles
(C) heroin
(D) alcohol
(E) cocaine
13. According to social learning theory, gender identity is
I. a process which occurs when young children unconsciously identify with the same-sex parent.
II. a result of being positively reinforced for acting in ways that conform to male and female roles.
III. learned through observing and imitating role models like their parents.
(A) I only
(B) II only
(C) III only
(D) II and III only
(E) I, II, and III
14. Which of the following theories best exemplifies continuity?
(A) Erikson’s psychosocial theory
(B) Vygotsky’s sociocultural theory
(C) Piaget’s cognitive development theory
(D) Kohlberg’s theory of moral development
(E) Gilligan’s theory of moral development
15. According to Kohlberg’s theory, postconventional morality requires thinking at Piaget’s
(A) sensorimotor level
(B) preoperational level
(C) concrete operational level
(D) formal operational level
(E) universal principle level
![]() Answers and Explanations
Answers and Explanations
1. D—Securely attached kids tend to come to their mother for comfort when their mothers return. They are not necessarily clingy as choice C suggests.
2. A—Nature refers to our heredity, and nurture refers to environmental factors.
3. C—Longitudinal research. If an experimenter is interested in looking at the long-term effects of divorce on children like Mavis Hetherington did, follow-up visits and observations would be made periodically. The disadvantage of this research method is how costly it is to conduct these follow-up visits and how long it takes to analyze the results to reach conclusions.
4. E—Object permanence occurs as a milestone in the sensorimotor stage when children can picture objects in their heads. When an experimenter hides a cookie behind a newspaper and the child uncovers it and says “cookie,” the child has achieved object permanence and is capable of representational thought.
5. A—The rooting reflex can be seen when someone puts a finger on the baby’s cheek and the baby turns its head.
6. B—Dorothy is experiencing the positive side of Erikson’s eighth stage of integrity. People like Dorothy tend to enjoy their golden years and continue to develop their interests.
7. C—Conventional. Mr. Hernandez’s moral reasoning conforms with Kohlberg’s stage 4 “Law and Order” morality, which is a stage of the conventional level.
8. A—Specific stimuli have a major effect on development that they do not produce at other times. Konrad Lorenz demonstrated the “critical period” for imprinting in goslings. Newly hatched babies first exposed to Lorenz followed him rather than their natural mothers if they had not been exposed to her soon after birth. Some theorists argue that mother–infant bonding and language development have critical periods.
9. A—Both Piaget and Kohlberg stressed the importance of changes in thinking in their developmental stages. For example, both recognized that egocentric young children see the consequences of their actions from their own perspectives.
10. A—Contact comfort. Harlow’s work with rhesus monkeys and surrogate mothers showed that even when food-deprived and anxious, monkeys preferred the terrycloth monkey to the wire monkey with food.
11. B—The authoritative style of parenting is seen as the “best” style for nurturing independent, responsible, and socially competent teens and adults.
12. D—Alcohol. The child’s mother likely drank alcohol throughout the pregnancy, producing the baby born with fetal alcohol syndrome. The effects of alcohol on prenatal brain development can be devastating.
13. D—Both reinforcement and observing and imitating role models like parents contribute to the development of gender identity, according to some (behavioral) social learning theorists.
14. B—Vygotsky’s sociocultural theory. Vygotsky advocated continuous cognitive growth. Vygotsky believed that with a mentor’s help, children can progress more rapidly through the same milestones they would achieve without a mentor’s help.
15. D—Formal operational level. Kohlberg modeled his stages of moral development after Piaget’s stages of cognitive development. Those in Piaget’s formal operational stage have developed the ability to think abstractly and, thus, have the ability to move to the postconventional moral thinking of Kohlberg’s stages 5 and 6.
![]() Rapid Review
Rapid Review
Developmental psychology—study of physical, intellectual, social, and moral changes across the lifespan from conception to death.
Three controversies of developmental psychology are:
1. Nature–nurture controversy—deals with the extent to which heredity and the environment each influence behavior.
2. Continuity–discontinuity controversy—deals with the issue of whether development is a gradual, continuous process or a sequence of separate stages.
3. Stability–change controversy—deals with the issue of whether or not personality traits present during infancy endure throughout the lifespan.
Research methods of developmental psychologists include experiments, naturalistic observations, correlational studies, and case studies. These designs are conducted to assess change over time:
• Cross-sectional—different age groups are tested at the same time.
• Longitudinal—same participants are tested multiple times with the same or similar tests.
• Cohort sequential—combines cross-sectional and longitudinal to correct for cohort effect.
Cohort effect—observed group differences based on the era when people were born and grew up, exposing them to particular experiences that may affect results of cross-sectional studies.
Physical Development
Critical period—a time interval during which specific stimuli have a major effect on development that the stimuli do not produce at other times.
Prenatal development—period of development that begins with fertilization, or conception, and ends with birth.
Zygote—a fertilized ovum with the genetic instructions for a new individual, normally contained in 46 chromosomes.
Embryo—the developmental prenatal stage (from about 2 weeks through 2 months after fertilization) when most organ development begins.
Fetus—the developing human organism from about 9 weeks after conception to birth when organ systems begin to interact; sex organs and sense organs become refined.
Teratogen—harmful substances (drugs or viruses) during the prenatal period that can cause birth defects.
Fetal alcohol syndrome (FAS)—a cluster of abnormalities that occurs in babies of mothers who drink alcoholic beverages during pregnancy, which includes low intelligence, small head with flat face, misshapen eyes, flat nose, and thin upper lip, as well as some degree of intellectual impairment.
Neonate—newborn baby from birth to 1 month old; shows reflexive behavior.
Reflex—the simplest form of behavior. Reflexes of neonate include:
• Rooting reflex—the newborn’s tendency to move its head when stroked on the cheek, turn toward the stimulus as if searching for a nipple, and open its mouth.
• Sucking—the automatic response of drawing in anything at the mouth.
• Swallowing—automatic contraction of throat muscles that enables food to pass into the esophagus without choking.
• Grasping reflex—infant closes his or her fingers tightly around an object put in hand.
• Moro or startle reflex—when exposed to a loud noise or sudden drop, the neonate automatically arches his or her back, flings his or her limbs out, and quickly retracts them.
As the infant matures, developing voluntary control over behaviors, many reflexes disappear.
Habituation—decreasing responsiveness with repeated presentation of the same stimulus.
Development proceeds from head to tail, from the center of the body outward, enabling baby to lift its head, roll over, sit, creep, stand, and walk—usually in that order. Proliferation of dendrites at a rapid rate is a major way the brain changes during childhood.
Puberty—the early adolescent period, marked by accelerated growth and onset of the ability to reproduce.
Primary sex characteristics—the reproductive organs (ovaries, uterus, and testes) and external genitals (vulva and penis).
Secondary sex characteristics—the nonreproductive sexual characteristics including developed breasts in females; facial hair, Adam’s apple, and deepened voice in males; and pubic hair and underarm hair in both.
Menarche—first menstrual period at about age 12½, marks female fertility. Male fertility is marked by ejaculation of semen with viable sperm at about age 14. Adolescent brain changes include selective pruning of dendrites and development of emotional limbic system and frontal lobes.
Our physical abilities peak by our mid-20s.
Menopause—the cessation of the ability to reproduce accompanied by a decrease in production of female sex hormones; occurs at about age 50.
Cognitive Development
Schema—framework of basic ideas and preconceptions about people, objects, and events based on past experience in long-term memory.
Assimilation—process by which we incorporate new information into our existing cognitive structures or schemas.
Accommodation—process by which we modify our schemas to fit new information.
Piaget’s theory of cognitive development involves four sequential and discontinuous stages:
1. Sensorimotor stage—Piaget’s first stage (0–2 years) during which the infant experiences the world through senses and action patterns; progresses from reflexes to object permanence (awareness that objects still exist when out of sight) and symbolic thinking.
2. Preoperational stage—Piaget’s second stage of cognitive development (2–7 years) during which the child represents and manipulates objects with symbols (language) and is egocentric.
• Egocentrism—seeing the world from one’s own perspective; the inability to see reality from the perspective of another person, characteristic of the preoperational child.
• Animism—belief of a preoperational child that all things are living.
• Artificialism—the belief of the preoperational child that all objects are made by people.
3. Concrete operational stage—Piaget’s third stage of cognitive development (7–12 years) during which the child develops simple logic and masters conservation concepts.
• Conservation concepts—changes in the form of an object do not alter physical properties of mass, volume, and number.
4. Formal operational stage—Piaget’s fourth stage of cognitive development (12+ years) during which the child begins to think logically about abstract concepts and engages in hypothetical thinking.
Lev Vygotsky’s sociocultural theory of cognitive development emphasized the role of the environment (nurture) and gradual growth (continuity) in intellectual functioning.
Internalization—the process of absorbing information from a specified social environmental context.
Zone of proximal development (ZPD)—the range between the level at which a child can solve a problem working alone with difficulty, and the level at which a child can solve a problem with the assistance of adults or more-skilled children.
Alzheimer’s disease—a fatal degenerative disease in which brain neurons progressively die, causing loss of memory, reasoning, emotion, control of bodily functions, and then death.
Moral Development
Moral development—growth in the ability to tell right from wrong, control impulses, and act ethically.
Lawrence Kohlberg’s theory of moral development: moral thinking develops in stages as cognitive abilities develop, with 3 levels divided into 6 sequential stages:
• Preconventional level—when at the preoperational stage of cognitive development, individuals do the right thing to:
stage 1—avoid punishment, obey authority
stage 2—further self-interests, gain reward
• Conventional level—when at the concrete operational stage of cognitive development or formal operational stage for most people:
stage 3—conform, live up to expectations of others
stage 4—maintain law and order, do your duty
• Postconventional level—reached by only some people in the formal operational stage.
stage 5—social contract, to promote society’s welfare
stage 6—to promote justice
Carol Gilligan criticized Kohlberg’s study because it focused on males, and women rarely reach Kohlberg’s highest stage. She said women follow an ethic of care, rather than justice.
Social Development
Social development looks at the influence of others on the development of a person.
Culture—behaviors, ideas, attitudes, and traditions transmitted from one generation to the next within a group of people who share a common language and environment.
Bonding—creation of close emotional relationship between mother (or parents) and baby shortly after birth.
Attachment—a close emotional bond or relationship between the infant and the caregiver.
Harry Harlow found monkeys separated from their mothers sought comfort from a soft cloth-covered substitute (surrogate) rather than a bare wire substitute with a feeding bottle, showing attachment isn’t based on feeding.
Mary Ainsworth’s “strange situation” research categorized a type of attachment based on how a baby reacted to, and after, temporary absence of mother:
• Secure attachment—after absence baby is happy to see mother, receptive to her contact. Securely attached babies tend to become socially competent children.
• Insecure attachment—after absence baby is angry and rejecting of mother, avoids her, ignores her, or behaves inconsistently.
Temperament—an infant’s natural disposition to show a particular mood at a particular intensity for a specific period.
Self-awareness—consciousness of oneself as a person.
Social referencing—observing the behavior of others in social situations to obtain information or guidance.
Diana Baumrind identified four parenting styles that affect emotional growth of children:
1. Authoritarian parenting style—sets up absolute and restrictive rules accompanied by punishment for disobedience.
2. Authoritative parenting style—focuses on flexible rules for which reasons are generally given. Parents are warm and nurture independence within guidelines.
3. Permissive parenting style—sets no firm guidelines for behavior and tends to give in to demands of the child.
4. Uninvolved parenting style—makes few demands, shows low responsiveness and little communication.
For individualistic cultures, the most self-reliant, socially competent children with the highest self-esteem tend to have warm, authoritative parents.
Erik Erikson’s Theory of Psychosocial Development looks at development across the life span in a social context in 8 sequential stages during which we are faced with a crisis to resolve:
Table 13.1 Erik Erikson’s Theory of Psychosocial Development
Gender Development
Gender—the sociocultural dimension of being biologically male or female.
Gender roles—sets of expectations that prescribe how males and females should act, think, feel.
Gender identity—person’s sense of being male or female.
Gender stability—child’s understanding that sex identity is stable over time.
Gender consistency—child’s understanding that his or her sex won’t change even if he or she acts like the opposite sex.
Gender schema—mental set of what society considers appropriate behavior for each of the sexes.
Gender role stereotypes—broad categories that reflect our impressions and beliefs about males and females.
Androgyny—the presence of desirable masculine and feminine characteristics in one individual.