5 Steps to a 5 AP Psychology, 2014-2015 Edition (2013)
STEP 4. Review the Knowledge You Need to Score High
Chapter 16. Abnormal Behavior
IN THIS CHAPTER
Summary: What is the first thing that comes to mind when you think about psychology? Before you took a psychology course, it was probably mental health, especially abnormal behavior. Actually, 90% of what psychologists study is about normal behavior. As president of the American Psychological Association, Martin Seligman promoted the positive psychology movement, an emphasis on the study of human strengths, fulfillment, and optimal living to help us improve our lives. Although this movement is gaining in strength and popularity, mental health professionals are still needed to help people suffering from psychological problems.
This chapter looks at definitions, causes, and types of psychological disorders.

Key Ideas
![]() Defining abnormal behavior
Defining abnormal behavior
![]() Causes of abnormal behavior
Causes of abnormal behavior
![]() Anxiety disorders
Anxiety disorders
![]() Somatoform disorders
Somatoform disorders
![]() Dissociative disorders
Dissociative disorders
![]() Mood disorders
Mood disorders
![]() Schizophrenia
Schizophrenia
![]() Personality disorders
Personality disorders
Defining Abnormal Behavior
Defining abnormal behavior and showing how it is different from normal behavior is difficult and controversial. A common definition of abnormal behavior is behavior that is personally disturbing or disabling, or culturally so deviant that others judge it as maladaptive, inappropriate, or unjustifiable. Atypical or deviant means that, statistically, the behavior is rare and has a very low probability of occurring. Legally, insanity is an inability to determine right from wrong. This may result in commitment because insane individuals are frequently a threat to themselves or to the community.
Psychiatrist Thomas Szasz sees classification of mental illness as reason to justify political repression, an extreme position that causes us to examine assumptions about what’s normal and what isn’t. David Rosenhan of Stanford University demonstrated that ideas of normality and abnormality are not as clear and accurate as people think. He and colleagues faked the single symptom of hearing voices to gain admission to mental hospitals in five states. They abandoned the symptom once admitted. They found hospitalization to be dehumanizing. Admitted with the diagnosis of paranoid schizophrenia, they were discharged with the diagnosis of paranoid schizophrenia in remission (under control).
Causes of Abnormal Behavior
What causes abnormal behavior? Each perspective of psychology assigns different reasons. The psychoanalytic perspective believes abnormal behavior results from internal conflict in the unconscious stemming from early childhood traumas. The behavioral approach says abnormal behavior consists of maladaptive responses learned through reinforcement of the wrong kinds of behavior. Humanists believe abnormal behavior results from conditions of worth society places upon the individual, which cause a poor self-concept. Since behavior is influenced by how we perceive the world, the cognitive approach sees abnormal behavior as coming from irrational and illogical perceptions and belief systems. Evolutionary psychologists consider mental disorders as harmful evolutionary dysfunctions that occur when evolved psychological mechanisms do not perform their naturally selected functions effectively. Finally, the biological approach explains abnormal behavior as the result of neurochemical and/or hormonal imbalances, genetic predispositions, structural damage to brain parts, or faulty processing of information by the brain.
The Medical Model
Abnormal behavior is often talked about as mental illness. The medical model looks at abnormal behavior as a disease, using terms such as psychopathology, which is the study of the origin, development, and manifestations of mental or behavioral disorders; etiology, which is the apparent cause and development of an illness; and prognosis, which forecasts the probable course of an illness. The American Psychiatric Association used a medical model for the Diagnostic and Statistical Manual (DSM-IV) that classifies psychological disorders by their symptoms. This guidebook for mental health professionals lists diagnostic criteria for 17 major categories of mental disorders, subdivided into about 400 disorders. DSM-IV enables mental health professionals to communicate information about individuals who suffer from abnormalities, and helps them decide how to treat an individual. DSM-IV is the 1994 revision (DSM-IV-TR, 2000) of DSM-III-R published in 1987. Early versions (DSM-I and II) were unreliable and invalid, but beginning with DSM-III, diagnostic categories have been clearly listed, assumptions about suspected causes of disorders have been eliminated, numbers of disorders have been increased, and diagnoses are given on five axes (dimensions). Axis I: Clinical Syndromes contains all of the major disorders including anxiety, depression, schizophrenia, substance abuse, and organic mental disorders. Axis II: Personality Disorders and Mental Retardation contains disorders such as obsessive-compulsive and mild retardation that could be overlooked when focus is on Axis I. Individuals can have diagnoses on both Axes I and II. The other axes deal with general medical conditions, psychosocial and environmental problems, and global assessment of functioning. Reliability of diagnoses has improved significantly and validity is considered to have been improved. Most North American third-party providers (medical insurance companies) require diagnoses from DSM-IV for payment of mental health benefits. Criticisms of the use of DSM-IV include the thought that “labeling is disabling,” whereby diagnostic labels are applied to the whole person (e.g., John’s a schizophrenic) rather than used to mean the individual is suffering from a particular disorder; and that categorization results in attributing characteristics to the individual that he or she doesn’t possess, or in missing something important about the individual.
Types of Disorders
Anxiety Disorders
Anxiety is the primary symptom, or the primary cause of other symptoms, for all anxiety disorders. Anxiety is a feeling of impending doom or disaster from a specific or unknown source that is characterized by mood symptoms of tension, agitation, and apprehension; bodily symptoms of sweating, muscular tension, and increased heart rate and blood pressure; as well as cognitive symptoms of worry, rumination, and distractibility. Anxiety disorders include panic disorder, generalized anxiety disorder, phobias, obsessive-compulsive disorder, and post-traumatic stress disorder.
• Panic disorder is the diagnosis when an individual experiences repeated attacks of intense anxiety along with severe chest pain, tightness of muscles, choking, sweating, or other acute symptoms. These symptoms can last anywhere from a few minutes to a couple of hours. Panic attacks have no apparent trigger and can happen at any time. Since these are statistically rare, having perhaps three of these in a 6-month period of time would be cause for alarm.
• Generalized anxiety disorder is similar to a panic disorder. Symptoms must occur for at least 6 months and include chronic anxiety not associated with any specific situation or object. The person frequently has trouble sleeping, is hypervigilant and tense, has difficulty concentrating, and can be irritable much of the time.
Panic disorder has acute symptoms short in duration, whereas generalized anxiety disorder has less intense symptoms for a longer period of time.

• Phobias are intense, irrational fear responses to specific stimuli. Nearly 5% of the population suffers from some mild form of phobic disorder. A fear turns into a phobia when it provokes a compelling, irrational desire to avoid a dreaded situation or object, disrupting the person’s daily life. Common phobias include:
agoraphobia—fear of being out in public
acrophobia—fear of heights
claustrophobia—fear of enclosed spaces
zoophobia—fear of animals (such as snakes, mice, rats, spiders, dogs, and cats)
• Obsessive-compulsive disorder (OCD) is a compound disorder of thought and behavior. Obsessions are persistent, intrusive, and unwanted thoughts that an individual cannot get out of his or her mind. Obsessions are different from worries; they generally involve a unique topic (such as dirt or contamination, death, or aggression), are often repugnant, and are seen as uncontrollable. If a person were frequently bothered by thoughts of wanting to harm others, this would be called an obsession. Obsessions are often accompanied by compulsions, ritualistic behaviors performed repeatedly, which the person does to reduce the tension created by the obsession. Common compulsions include handwashing, counting, checking, and touching.
• Post-traumatic stress disorder (PTSD) is a result of some trauma experienced (natural disaster, war, violent crime) by the victim. Victims reexperience the traumatic event in nightmares about the event, or flashbacks in which the individual relives the event and behaves as if he or she is experiencing it at that moment. Victims may also experience reduced involvement with the external world, and general arousal characterized by hyperalertness, guilt, and difficulty concentrating.
The behavioral perspective says that anxiety responses are acquired through classical conditioning and maintained through operant conditioning. The cognitive perspective attributes anxiety disorders to misinterpretation of harmless situations as threatening, focusing excessive attention on perceived threats, and selectively recalling threatening information. The biological perspective attributes anxiety disorders at least partly to neurotransmitter imbalances. Generalized anxiety disorder, often treated with benzodiazepines (Valium, Xanax), is associated with too little availability of the inhibitory neurotransmitter GABA in some neural circuits, while obsessive-compulsive disorder and panic disorder, often treated with antidepressants (Prozac, Paxil, Zoloft), are associated with low levels of serotonin. The evolutionary perspective attributes the presence of anxiety to natural selection for enhanced vigilance that operates ineffectively in the absence of real threats.
Somatoform Disorders
Somatoform disorders are characterized by physical symptoms such as pain, paralysis, blindness, or deafness without any demonstrated physical cause. Somatoform disorders are different from psychosomatic disorders such as ulcers, tension headaches, and cardiovascular problems. Although the causes of both somatoform and psychosomatic disorders are psychological and the symptoms are physical, with somatoform disorders, no physical damage is done. Somatoform disorders include somatization disorder, conversion disorder, and hypochondriasis.
• Somatization disorder is characterized by recurrent complaints about usually vague and unverifiable medical conditions such as dizziness, heart palpitations, and nausea, which do not apparently result from any physical cause. To be classified as having a somatization disorder, an individual needs to have complained about, taken medicine for, changed lifestyle because of, or seen a physician regarding many different symptoms.
• Conversion disorder (known as hysteria in the Freudian era) is characterized by loss of some bodily function, such as becoming blind, deaf, or paralyzed, without physical damage to the affected organs or their neural connections. It is often marked by indifference and quick acceptance on the part of the patient. The symptoms usually last as long as anxiety is present.
• Suffering from hypochondriasis, a person unrealistically interprets physical signs—such as pains, lumps, and irritations—as evidence of serious diseases. The person consequently becomes anxious and upset about the symptoms. You probably know someone who thinks a headache is a sign that he or she is developing a brain tumor or that a bit of scar tissue is the beginning of cancer. Hypochondriasis differs from somatization in that those with hypochondriasis show excessive anxiety about only one or two symptoms and the implications they could have for potential future diseases.
Psychoanalyst Sigmund Freud’s explanation attributes somatoform disorders to bottled-up emotional energy that is transformed into physical symptoms. Behaviorists explain that operant responses are learned and maintained because they result in rewards. Cognitive behaviorists continue that the rewards enable individuals with somatoform disorders to avoid some unpleasant or threatening situation, provide an explanation or justification for failure, or attract concern, sympathy, and care. Social cognitive theorists think that individuals with somatoform disorders focus too much attention on their internal physiological experiences, amplifying their bodily sensations, and forming disastrous conclusions about minor complaints.
Dissociative Disorders
Dissociative disorders are psychological disorders that involve a sudden loss of memory (amnesia) or change in identity. If extremely stressed, an individual can experience separation of conscious awareness from previous memories and thoughts. Dissociative disorders include dissociative amnesia, dissociative fugue, and dissociative identity disorder.
• Dissociative amnesia is a loss of memory for a traumatic event or period of time that is too painful for an individual to remember. The person holds steadfast to the fact that he or she has no memory of the event and becomes upset when others try to stimulate recall. In time, parts of the memory may begin to reappear. A woman whose baby has died in childbirth may block out that memory and perhaps the entire period of her pregnancy. When more emotionally able to handle this information, the woman may gradually come to remember it.
• Dissociative fugue is a memory loss for anything having to do with personal memory. It is accompanied by flight from the person’s home, after which the person establishes a new identity. All skills and basic knowledge are still intact. The cause of the fugue is often abundant stress or an immediate danger of some news coming out that would prove embarrassing to the individual.
• Dissociative identity disorder (DID), formerly called multiple personality disorder, is diagnosed when two or more distinct personalities are present within the same individual. Although extremely unusual, it is most common in people who have been a victim of physical or sexual abuse when very young. Amnesia is involved when alternate personalities “take over.” Missing time is one of the clues to this diagnosis. Each alternate personality has its own memories, behaviors, and relationships, and might have different prescriptions, allergies, and other physical symptoms. Although there has been some interesting work done by the National Institute for Mental Health that lends credibility to this diagnosis, many professionals are still skeptical about it.
Psychoanalysts explain dissociative disorders as repression of anxiety and/or trauma, caused by such disturbances of home life as beatings, rejection from parents, or sexual abuse. Many social learning theorists are skeptical about DID, and think that individuals displaying the disorder are role playing. They question why dissociative identity disorder, also known as multiple personality, has become so much more prevalent since publication of books and production of films dealing with the disorder, and why different personalities pop out, in contrast to years ago when alternate personalities emerged very slowly.
Mood Disorders
Mood disorders are psychological disorders characterized by a primary disturbance in affect or mood that colors the individual’s entire emotional state. This disrupts the person’s normal ability to function in daily life. Two types of mood disorders are unipolar (depressive) and bipolar (manic-depressive) disorders. Most are treated at least in part by drugs, suggesting a biological etiology or cause. The prevalence of depression has been increasing, affecting at least twice as many women as men.
Because it occurs so often, depression has been called the “common cold of psychological disorders.”
• Major depressive disorder, or unipolar depression, involves intense depressed mood, reduced interest or pleasure in activities, loss of energy, and problems in making decisions for a minimum of 2 weeks. The individual feels sad, hopeless, discouraged, “down,” and frequently isolated, rejected, and unloved. In addition to this sadness, there are a series of changes in eating, sleeping, and motor activity, and a lack of pleasure in activities that usually caused pleasure in the past. Cognitive symptoms include low self-esteem, pessimism, reduced motivation, generalization of negative attitudes, exaggeration of seriousness of problems, and slowed thought processes. Suicidal thoughts, inappropriate guilt, and other faulty beliefs may also be present.
• Depression with seasonal pattern, also known as seasonal affective disorder, is a type of depression that recurs, usually during the winter months in the northern latitudes. One hypothesis as to why this happens is that shorter periods of and less direct sunlight during winter disturbs both mood and sleep/wake schedules, bringing on the depression.
• Bipolar disorder is characterized by mood swings alternating between periods of major depression and mania, the two poles of emotions. Symptoms of the manic state include an inflated ego, little need for sleep, excessive talking, and impulsivity. Rapid cycling is usually characterized by short periods of mania followed almost immediately by deep depression, usually of longer duration. Newer drug treatments, including lithium carbonate, have proved successful in bringing symptoms under control for many sufferers.
Biological psychologists have evidence from family studies, including twin studies, that there is a genetic component involved in mood disorders. Too much of the neurotransmitter norepinephrine is available during mania; too little of norepinephrine or serotonin during depression. Prozac, Zoloft, and Paxil increase availability of serotonin by blocking reuptake. PET and fMRI scans reveal lowered brain energy consumption in individuals with depression, especially in the left frontal lobe, associated with positive emotions; and MRI and CAT scans show abnormal shrinkage of frontal lobes in long-term severely depressed patients. Psychoanalysts attribute depression to early loss of or rejection by a parent, resulting in depression when the individual experiences personal losses later in life and turns anger inside. Behaviorists say that depressed people elicit negative reactions from others, resulting in maintenance of depressed behaviors. The social cognitive (cognitive-behavioral) perspective holds that self-defeating beliefs that may arise from learned helplessness influence biochemical events, fueling depression. Learned helplessness is the feeling of futility and passive resignation that results from inability to avoid repeated aversive events. According to psychologist Martin Seligman, a negative explanatory style puts an individual at risk for depression when bad events occur. When bad events happen, people with a negative (pessimistic) explanatory style think the bad events will last forever, affect everything they do, and are all their fault; they give stable, global, internal explanations. Cognitive viewpoints include Aaron Beck’s theory (cognitive triad) that depressed individuals have a negative view of themselves, their circumstances, and their future possibilities, and that they generalize from negative events; and Susan Nolen-Hoeksema’s rumination theory that depressed people who go over and over the negative event in their minds are prone to more intense depression than those who distract themselves.
Schizophrenia
Schizophrenia is a broad umbrella of symptoms and disorders characterized by psychosis or lack of touch with reality evidenced by highly disordered thought processes. Patients with schizophrenia can show abnormal thinking, emotion, movement, socialization, and/or perception. Because one cause of schizophrenia is an excess of dopamine, anti-psychotic drugs are effective in treating some symptoms in about 50% of the sufferers. A positive symptom of schizophrenia isn’t something that is good, but a behavioral excess or peculiarity rather than an absence. Delusions and hallucinations, two frequent signs of schizophrenia, are both positive symptoms. Delusions are erroneous beliefs that are maintained even when compelling evidence to the contrary is presented. Hallucinations are false sensory perceptions, such as the experience of seeing, hearing, or otherwise perceiving something that is not present. Lack of emotion, sometimes called flat affect; social withdrawal; apathy; inattention; and lack of communication are examples of negative symptoms of schizophrenia. Four types of schizophrenia are disorganized, catatonic, paranoid, and undifferentiated.
• Symptoms of disorganized schizophrenia include incoherent speech, inappropriate mood, hallucinations, and delusional thought patterns. People with disorganized schizophrenia may make no sense when talking and act in a very bizarre way that is inappropriate for the situation (e.g., laughing in the back of the church during a funeral). Silly, childlike behavior is typical.
• Paranoid schizophrenia is characterized by delusions of grandeur, persecution, and reference. The delusions typically form an elaborate network resulting from misinterpretation of reality. For example, people with paranoid schizophrenia often think that they are special and have been selected for exceptional attention (delusions of reference). They often misinterpret occurrences as directly relevant to them, such as lightning being a signal from God. They frequently believe that such attention is because of their specialness and that they are world leaders (delusions of grandeur). They then think that others are so threatened that these other people plot against them (delusions of persecution). Suffering delusions of persecution, people are fearful and can be a danger as they attempt to defend themselves against their imagined enemies.
• Catatonic schizophrenia is characterized by disordered movement patterns, sometimes immobile stupor, or frenzied and excited behaviors. People suffering from this disorder might remain in one position, becoming “statues” with what is called waxy flexibility or holding postures that would normally be impossible to maintain by others.
• Undifferentiated or simple schizophrenia is marked by disturbances of thought or behavior and emotion that do not fit neatly into any of the above categories. One area of dysfunction is noted, and yet the person may be perfectly normal in every other aspect of life.
Biological psychologists attribute some positive symptoms of schizophrenia, such as hallucinations and delusions, to excessively high levels of the neurotransmitter dopamine, and some negative symptoms, such as lack of emotion and social withdrawal, to lack of the neurotransmitter glutamate. Brain scans show abnormalities in numerous brain regions of individuals with schizophrenia. These abnormalities may result from teratogens such as viruses or genetic predispositions. The diathesis-stress model holds that people predisposed to schizophrenia are more vulnerable to stressors than other people. Thus, only people who are both predisposed and also stressed are likely to develop schizophrenia. Psychoanalysts attribute schizophrenia to fixation at the oral stage and a weak ego. Behaviorists assume that schizophrenia results from reinforcement of bizarre behavior. Humanists think schizophrenia is caused by lack of congruence between the public self and actual self.
Schizophrenia is NOT split personality! People with schizophrenia experience a split with reality. People with dissociative identity disorder show two or more personalities.
Personality Disorders
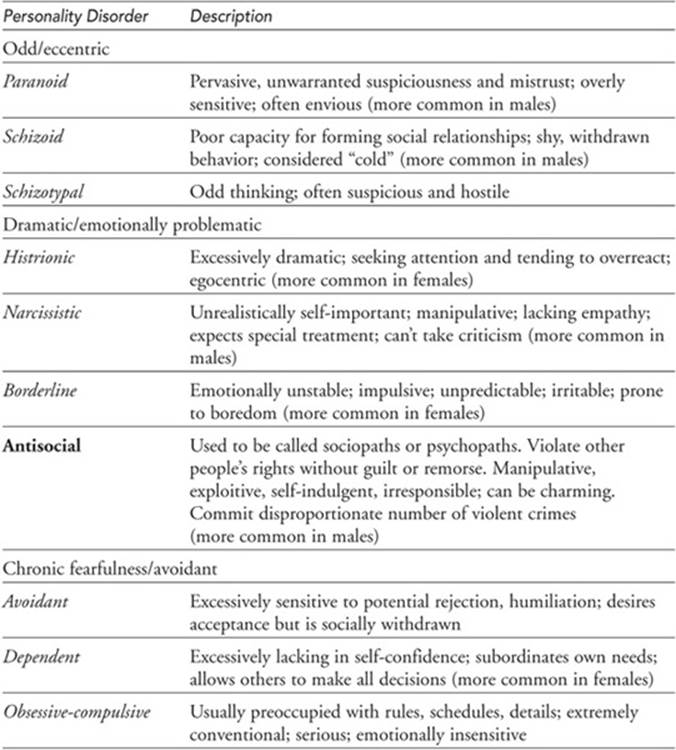
People with personality disorders have longstanding, maladaptive thought and behavior patterns that are troublesome to others, harmful, or illegal. Although these patterns impair people’s social functioning, individuals do not experience anxiety, depression, or delusions. DSM-IV classifies personality disorders on Axis II grouped into three clusters: odd/eccentric (including paranoid, schizoid, schizotypal), dramatic/emotionally problematic (including histrionic, narcissistic, borderline, and antisocial), and chronic fearfulness/avoidant (including avoidant, dependent, and obsessive-compulsive). See Table 16.1.
Table 16.1 Personality Disorders
Developmental Disorders
Disorders of infancy, childhood, and adolescence include attention-deficit hyperactivity disorder, infantile autism, anorexia nervosa, and bulimia nervosa.
• Children with attention-deficit hyperactivity disorder (ADHD) are unable to focus their attention, are easily distracted, and often act impulsively, quickly changing activities, which results in failure to complete tasks. Their inattention and inappropriate behaviors often lead to personal, social, and academic problems. ADHD is diagnosed 10 times more frequently in boys than in girls.
• Autism can be an extremely serious childhood disorder. Diagnosis is based on three primary symptoms that become evident early in life: lack of responsiveness to other people, impairment in verbal and nonverbal communications, and very limited activities and interests. Children with autism engage in repetitive behaviors. Autism has become more common.
• Eating disorders have also become more common, especially in adolescent females in North America and Western Europe. Anorexia nervosa is an eating disorder characterized by a weight of less than 85% of normal, abnormally restrictive food consumption, and an unrealistic body image. No matter how emaciated they become, people with anorexia still think they are fat and may continue to lose weight, which can result in death. Bulimia nervosa is an eating disorder characterized by a pattern of eating binges involving intake of thousands of calories, followed by purging by either vomiting or using laxatives. Following the purge, people with bulimia typically feel guilty, self-critical, and depressed. Purging can cause sore throat, swollen glands, loss of tooth enamel, nutritional deficiencies, dehydration, and intestinal damage.
![]() Review Questions
Review Questions
Directions: For each question, choose the letter of the choice that best completes the statement or answers the question.
1. Hani was unable to tell the difference between right and wrong. Which of the following definitions of abnormal behavior is described in this example?
(A) maladaptive
(B) insanity
(C) commitment
(D) statistical
(E) personal
2. The behavioral approach attributes the cause of abnormal behavior to
(A) internal conflict from early childhood trauma
(B) the result of neurochemical imbalances
(C) poor self-concept
(D) reinforcement of maladaptive behaviors learned through experience
(E) irrational and illogical perceptions of reality
3. Which of the following best characterizes a person experiencing obsessive-compulsive disorder?
(A) Anna, who hyperventilates whenever she is trapped in an elevator
(B) Ben, who returns home seven times to see if he has turned off the stove
(C) Katia, who complains constantly about feeling sick and goes to many different doctors
(D) Kabir, who keeps remembering the plane crash that killed the other members of his family
(E) Miguel, who wanders about town in a daze, not sure who he is or how he got there
4. A soldier who experiences sudden blindness after seeing his buddies killed in battle is best diagnosed with
(A) a phobic disorder
(B) hypochondriasis
(C) bipolar disorder
(D) dissociative fugue
(E) conversion disorder
5. A common feature among people diagnosed with dissociative identity disorder is
(A) early childhood sexual or physical abuse
(B) repeated physical complaints
(C) relatives suffering from bipolar disorder
(D) excess of dopamine
(E) hallucinations and delusions
6. Which of the following is NOT characteristic of the manic state of bipolar disorder?
(A) inflated ego
(B) excessive talking
(C) shopping sprees
(D) fearlessness
(E) too much sleep
7. Paranoid personality disorder is characterized by
(A) unwarranted suspiciousness and mistrust of other people
(B) lack of interest in social relationships
(C) unusual preoccupation with rules and schedules
(D) instability revolving around problems of mood and thought processes
(E) pleasure-seeking, shallow feelings, lack of conscience
8. When Herb physically abuses his dates, he considers himself good with the ladies, has little remorse for his actions, and has had repeated trouble with authority figures. His likely diagnosis is
(A) autism
(B) narcissistic personality disorder
(C) antisocial personality disorder
(D) borderline personality disorder
(E) schizophrenia
9. A delusion is a
(A) phobia of being in social situations
(B) misperception of auditory and visual stimuli
(C) faulty and disordered thought pattern
(D) first indication of dissociative disorders
(E) characteristic of people suffering from dependent personality disorder
10. DSM-IV is most helpful for
(A) identifying the causes of psychological disorders
(B) recommending treatment for psychological disorders
(C) classifying psychological disorders
(D) distinguishing between sanity and insanity
(E) suggesting where consumers can get help for mental health issues
11. All of the following are classified as anxiety disorders EXCEPT
(A) phobias
(B) post-traumatic stress
(C) panic
(D) obsessive-compulsive disorder
(E) hypochondriasis
12. Which of the following is a negative symptom of schizophrenia?
(A) delusional thinking
(B) incoherent speech
(C) hyperexcitability
(D) hearing voices
(E) flat affect
13. Which of the following disorders is most closely associated with excessive levels of dopamine?
(A) histrionic personality
(B) dependent personality
(C) paranoid schizophrenia
(D) bipolar disorder
(E) major depression
14. Estrella always goes shopping with Maria. Because she has no confidence in her own decisions, she lets Maria decide what she should buy, and pays for clothes for Maria with money she was saving for a haircut. Estrella shows signs of which of the following personality disorders?
(A) histrionic
(B) dependent
(C) antisocial
(D) obsessive-compulsive
(E) narcissistic
![]() Answers and Explanations
Answers and Explanations
1. B—Insanity is a legal definition of abnormal behavior. It means that a person, at the time he or she committed a crime, could not distinguish between right and wrong.
2. D—The behavioral approach sees abnormal behavior as a result of faulty reinforcement of maladaptive behavior.
3. B—Ben shows checking behavior, a common problem associated with obsessive–compulsive disorder. His obsessive thought is that he may have left the stove on, and the ritualistic behavior or compulsion is the need to return home and “check” to make sure that it has been turned off.
4. E—A conversion disorder is characterized by excessive anxiety that has been transformed into a physical symptom without an organic or biological cause. The blindness probably does not disturb the soldier as much as it would if it were physiological, because it protects him from having to “see” any friends die in battle.
5. A—Childhood sexual or physical abuse is a common feature found in those diagnosed with dissociative identity disorder. Psychoanalytically trained professionals believe that, as a result of the trauma, the child “dissociates” as a defense mechanism and that the amnesia experienced by one or more of the personalities is massive repression.
6. E—Mania in the patient with bipolar disorder is characterized by little need for sleep. Sleep deprivation may actually trigger this phase of the disorder, and frequently during the manic cycle the patient gets 2 hours of sleep or less.
7. A—People diagnosed with paranoid personality disorder tend to be unduly suspicious and to mistrust others. They are overly sensitive and prone to jealousy.
8. C—Herb is clearly antisocial, and the lack of remorse or a guilty conscience for hurting others is a chief indicator of this personality disorder. It is difficult to treat people with this disorder.
9. C—A delusion is a disordered thought pattern characteristic of psychotic disorders like schizophrenia. Someone with paranoid schizophrenia might have delusions of grandeur, persecution, or reference.
10. C—DSM-IV is a handbook that lists common symptoms of psychological disorders, which helps professionals in the classifying and diagnosing of patients. It does not list either causes or treatments.
11. E—Hypochondriasis is classified as a somatoform disorder characterized by physical symptoms for which there is no demonstrable physical cause and by unrealistic interpretation of physical signs as evidence of serious diseases.
12. E—Flat affect is a negative symptom, a lack of any particular mood state. Each of the other answers shows a positive symptom of schizophrenia, one that is present.
13. C—Excessive dopamine is associated with positive symptoms of schizophrenia, such as hallucinations and delusions.
14. B—Estrella seems excessively lacking in self-confidence. She subordinates her own needs by buying clothes for Maria, and allows Maria to make decisions for her. These are characteristics of dependent personality disorder.
![]() Rapid Review
Rapid Review
Defining abnormal behavior—statistically rare, violates cultural norms, personally interferes with day-to-day living, and legally may cause a person to be unable to know right from wrong (insanity).
Causes of abnormal behavior by psychological perspective:
• Psychoanalytic: unresolved internal conflict in the unconscious mind.
• Behavioral: maladaptive behaviors learned from inappropriate rewards and punishment.
• Humanistic: conditions of worth imposed by society, which cause lowered self-concept.
• Cognitive: irrational and faulty thinking.
• Biological: neurochemical or hormonal imbalances; abnormal brain structures or genetics.
Brief descriptions of common psychological problems:
• Anxiety—a feeling of impending doom or disaster from a specific or unknown source that is characterized by mood symptoms of tension agitation, and apprehension; bodily symptoms of sweating, muscular tension, and increased heart rate and blood pressure; as well as cognitive symptoms of worry, rumination, and distractibility. Anxiety disorders include:
Generalized anxiety disorder—characterized by persistent, pervasive feelings of doom for at least six months not associated with a particular object or situation.
Panic disorder—unpredictable attacks of acute anxiety accompanied by high levels of physiological arousal that last from a few seconds to a few hours.
Phobia—irrational fear of specific objects or situations, such as animals or enclosed spaces.
Obsessive-compulsive disorder—recurrent, unwanted thoughts or ideas or compelling urges to engage in repetitive, ritual-like behavior.
Post-traumatic stress disorder (PTSD)—feelings of social withdrawal accompanied by atypically low levels of emotion caused by prolonged exposure to a stressor, such as a catastrophe; an individual may experience flashbacks and nightmares.
• Somatoform disorders are mental disorders involving a bodily or physical problem for which there is no physiological basis. Symptoms deal with the body and have no realistic physical cause for them. Somatoform disorders include:
Somatization disorder—recurrent complaints about usually vague and unverifiable medical conditions such as dizziness, heart palpitations, and nausea that do not apparently result from any physical cause.
Conversion disorder—actual loss of bodily function, such as blindness, paralysis, or numbness, due to excessive anxiety with no physiological cause.
Hypochondriasis—persistent and excessive worry about developing a serious illness.
• Dissociation—experience of two or more streams of consciousness cut off from each other. Dissociative disorders involve loss of memory or identity. The Freudian explanation is repression of hurtful situations too painful for the individual to deal with. Dissociative disorders involve the massive repression of traumatic events or unpleasant memories into the unconscious mind. Dissociative disorders include:
Dissociative amnesia—characterized by inability to remember repressed events or personal information.
Dissociative fugue—“traveling amnesiac disorder” characterized by moving away and assuming a new identity, with amnesia for the previous identity.
Dissociative identity disorder (formerly known as multiple personality disorder)—rare disorder in which two or more distinct personalities exist within the same person.
• Mood disorders—affective disorders characterized by significant shifts or disturbances in mood that affect normal perception, thought, and behavior. Mood disorders include:
Major (clinical) depression (also called unipolar mood disorder)—involves persistent and severe feelings of sadness and worthlessness accompanied by changes in appetite, sleeping, and behavior.
Bipolar disorder—characterized by extreme mood swings from unusual excitement to serious depression.
• Schizophrenia—a serious mental disorder (psychosis) characterized by thought disturbances, hallucinations, anxiety, emotional withdrawal, and delusions.
Psychosis—disorder characterized by an apparent break with reality.
Delusion—false belief of being plotted against (persecution), or being extraordinarily important (grandeur), or being controlled by others.
Hallucination—false sensory perception such as hearing voices or seeing images that are not present.
Four major types of schizophrenia: disorganized, catatonic, paranoid, and undifferentiated.
Disorganized schizophrenia (hebephrenia)—characterized by thought disturbances and silly behavior or absence of emotions.
Catatonic schizophrenia—characterized by bizarre movements or lack of movement, such as immobile stupor and waxy flexibility
• Personality disorders are classified on DSM-IV Axis II and grouped into three clusters: odd/eccentric (including paranoid, schizoid, schizotypal), dramatic/emotionally problematic (including histrionic, narcissistic, borderline, and antisocial), and chronic fearfulness/avoidant (including avoidant, dependent, and obsessive-compulsive). Personality disorders are characterized by persistent patterns of mal-adaptive and inflexible traits in personality.
• Developmental disorders involve disturbances in learning, language, and motor or social skills showing up in infancy, childhood, or adolescence. Developmental disorders include:
Attention-deficit hyperactivity disorder (ADHD)—characterized by the inability to focus attention, distractibility, and impulsivity.
Autism—characterized by impaired social interaction, poor communication, and limited activities and interests.
Anorexia nervosa—eating disorder characterized by abnormally restrictive eating, gross underweight, and unrealistic body image of being too fat.
Bulimia nervosa—eating disorder characterized by “binging and purging.”