Barron's AP Psychology, 7th Edition (2016)
Chapter 5. States of Consciousness
KEY TERMS
Consciousness
Levels of consciousness
Conscious level
Nonconscious level
Preconscious level
Subconscious level
Unconscious level
Sleep
Sleep cycles
Sleep stages
REM sleep
Sleep disorders
Insomnia
Narcolepsy
Sleep apnea
Night terrors
Dreams
Freudian dream interpretation
Activation-synthesis dream theory
Information-processing dream theory
Hypnosis
Posthypnotic amnesia
Posthypnotic suggestion
Role theory of hypnosis
State theory of hypnosis
Dissociation theory of hypnosis
Psychoactive drugs
Agonists
Antagonists
Tolerance
Withdrawal
Stimulants
Depressants
Hallucinogens (also called psychedelics)
Opiates
KEY PEOPLE
William James
Sigmund Freud
Ernest Hilgard
OVERVIEW
While you are reading this text, you can probably become aware of your sense of consciousness. Early psychologists such as William James, author of the first psychology textbook, were very interested in consciousness. However, since no tools existed to examine it scientifically, the study of consciousness faded for a time. Currently, consciousness is becoming a more common research area due to more sophisticated brain imaging tools and an increased emphasis on cognitive psychology.
The historical discussion about consciousness centers on the competing philosophical theories of dualism and monism. Dualists believe humans (and the universe in general) consist of two materials: thought and matter. Matter is everything that has substance. Thought is a nonmaterial aspect that arises from, but is in some way independent of, a brain. Dualists argue that thought gives humans free will. Some philosophers maintain that thought is eternal and continues existing after the brain and body die. Monists disagree and believe everything is the same substance, and thought and matter are aspects of the same substance. Thought is a by-product of brain processes and stops existing when the body dies.
Psychology does not try to address these metaphysical questions directly. However, psychologists are trying to examine what we can know about consciousness and to describe some of the processes or elements of consciousness. Psychologists define consciousness as our level of awareness about ourselves and our environment. We are conscious to the degree we are aware of what is going on inside and outside ourselves.
This psychological definition implies that consciousness is not like an on/off switch. We are not conscious or unconscious. Psychologists refer to different levels and different states of consciousness.
LEVELS OF CONSCIOUSNESS
Ironically, we experience different levels of consciousness in our daily life without being consciously aware of the experience. While you are reading this text, you might be tapping your pen or moving your leg in time to the music you are listening to. One level of consciousness is controlling your pen or leg, while another level is focused on reading these words. Research demonstrates other more subtle and complex effects of different levels of consciousness. The mere-exposure effect (also see Chapter 14) occurs when we prefer stimuli we have seen before over novel stimuli, even if we do not consciously remember seeing the old stimuli. For example, say a researcher shows a group of research participants a list of nonsense terms for a short period of time. Later, the same group is shown another list of terms and asked which terms they prefer or like best. The mere-exposure effect predicts that the group will choose the terms they saw previously, even though the group could not recall the first list of nonsense terms if asked. On some level, the group knows the first list.
A closely related concept is priming. Research participants respond more quickly and/or accurately to questions they have seen before, even if they do not remember seeing them. Another fascinating phenomenon that demonstrates levels of consciousness is blind sight. Some people who report being blind can nonetheless accurately describe the path of a moving object or accurately grasp objects they say they cannot see! One level of their consciousness is not getting any visual information, while another level is able to “see” as demonstrated by their behavior.
The concept of consciousness consisting of different levels or layers is well established. Not all researchers agree about what the specific levels are, but some of the possible types offered by researchers are shown in the following.
|
Conscious level |
The information about yourself and your environment you are currently aware of. Your conscious level right now is probably focusing on these words and their meanings. |
|
Nonconscious level |
Body processes controlled by your mind that we are not usually (or ever) aware of. Right now, your nonconscious is controlling your heartbeat, respiration, digestion, and so on. |
|
Preconscious level |
Information about yourself or your environment that you are not currently thinking about (not in your conscious level) but you could be. If I asked you to remember your favorite toy as a child, you could bring that preconscious memory into your conscious level. |
|
Subconscious level |
Information that we are not consciously aware of but we know must exist due to behavior. The behaviors demonstrated in examples of priming and mere-exposure effect suggest some information is accessible to this level of consciousness but not to our conscious level. |
|
Unconscious level |
Psychoanalytic psychologists believe some events and feelings are unacceptable to our conscious mind and are repressed into the unconscious mind. Many psychologists object to this concept as difficult or impossible to prove. See the section on psychoanalytic theory in Chapter 10 for more information about the unconscious. |
SLEEP
As a student, sleep is most likely a subject near and dear to your heart. Many studies show that a large percentage of high school and college students are sleep deprived, meaning they do not get as much sleep as their body wants. To a psychologist, referring to being asleep as being unconscious is incorrect. Sleep is one of the states of consciousness.
According to the psychological definition of consciousness, sleep is a state of consciousness because, while we are asleep, we are less aware of ourselves and our environment than we are when we are in our normal awake state. Other states of consciousness—drug-induced states, hypnosis, and so on—are states of consciousness for similar reasons.
Sleep Cycle
You may be familiar with the term circadian rhythm. During a 24-hour day, our metabolic and thought processes follow a certain pattern. Some of us are more active in the morning than others, some of us get hungry or go to the bathroom at certain times of day, and so on. Part of our circadian rhythm is our sleep cycle. Our sleep cycle is our typical pattern of sleep. Researchers using EEG machines can record how active our brains are during sleep and describe the different stages of sleep we progress through each night. Refer to Figure 5.1 for a graphic representation of the stages of a typical sleep cycle.
As you can see in Figure 5.1, sleep is far from being a time of unconsciousness. We cycle through different stages of sleep during the night. Our brain waves and level of awareness change as we cycle through the stages. The period when we are falling asleep is called sleep onset. This is the stage between wakefulness and sleep. Our brain produces alpha waves when we are drowsy but awake. We might experience mild hallucinations (such as falling or rising) before actually falling asleep and entering stage 1. While we are awake and in stages 1 and 2, our brains produce theta waves, which are relatively high-frequency, low-amplitude waves. However, the theta waves get progressively slower and higher in amplitude as we go from wakefulness and through stages 1 and 2. In stage 2, the EEG starts to show sleep spindles, which are short bursts of rapid brain waves. From there, we move into stages 3 and 4, which are sometimes called delta sleep (also called slow-wave sleep) because of the delta waves that exist during these stages. The slower the wave (slow waves are low-frequency waves), the deeper the sleep and less aware we are of our environment. A person in delta sleep is very difficult to wake up. If you are awakened out of delta sleep, you may be very disoriented and groggy. Delta sleep seems to be very important in replenishing the body’s chemical supplies, releasing growth hormones in children, and fortifying our immune system. A person deprived of delta sleep will be more susceptible to illness and will feel physically tired. Increasing exercise will increase the amount of time we spend in stages 3 and 4.
After a period of time in delta sleep, our brain waves start to speed up and we go back through stages 3 and 2. However, as we reach stage 1, our brain produces a period of intense activity, our eyes dart back and forth, and many of our muscles may twitch repeatedly. This is REM—rapid eye movement. This sleep stage is sometimes called paradoxical sleep since our brain waves appear as active and intense as they do when we are awake. The exact purposes of REM are not clear, but some effects are known. Dreams usually occur in REM sleep. (Dreams can occur in any stage of sleep, but it is far more likely that any detailed dream occurs in REM.) REM sleep deprivation interferes with memory. Individuals deprived of REM sleep will experience REM rebound—experiencing more and longer periods of REM—the next time they are allowed to sleep normally. The more stress we experience during the day, the longer our periods of REM sleep will be.
Notice in Figure 5.1 that not only do we cycle through these approximately 90-minute stages about 4–7 times during the night, the cycle itself varies during the night. As we get closer to morning (or whenever we naturally awaken), we spend more time in stages 1 and 2 and in REM sleep and less in stages 3 and 4. Also, age affects the pattern. Babies not only spend more total time sleeping than we do (up to 18 hours), they also spend more time in REM sleep. As we age, our total need for sleep declines as does the amount of time we spend in REM sleep. Although research has not answered all the questions about sleep, details about our sleep cycle provide clues as to why we spend so much of our life in this altered state of consciousness.
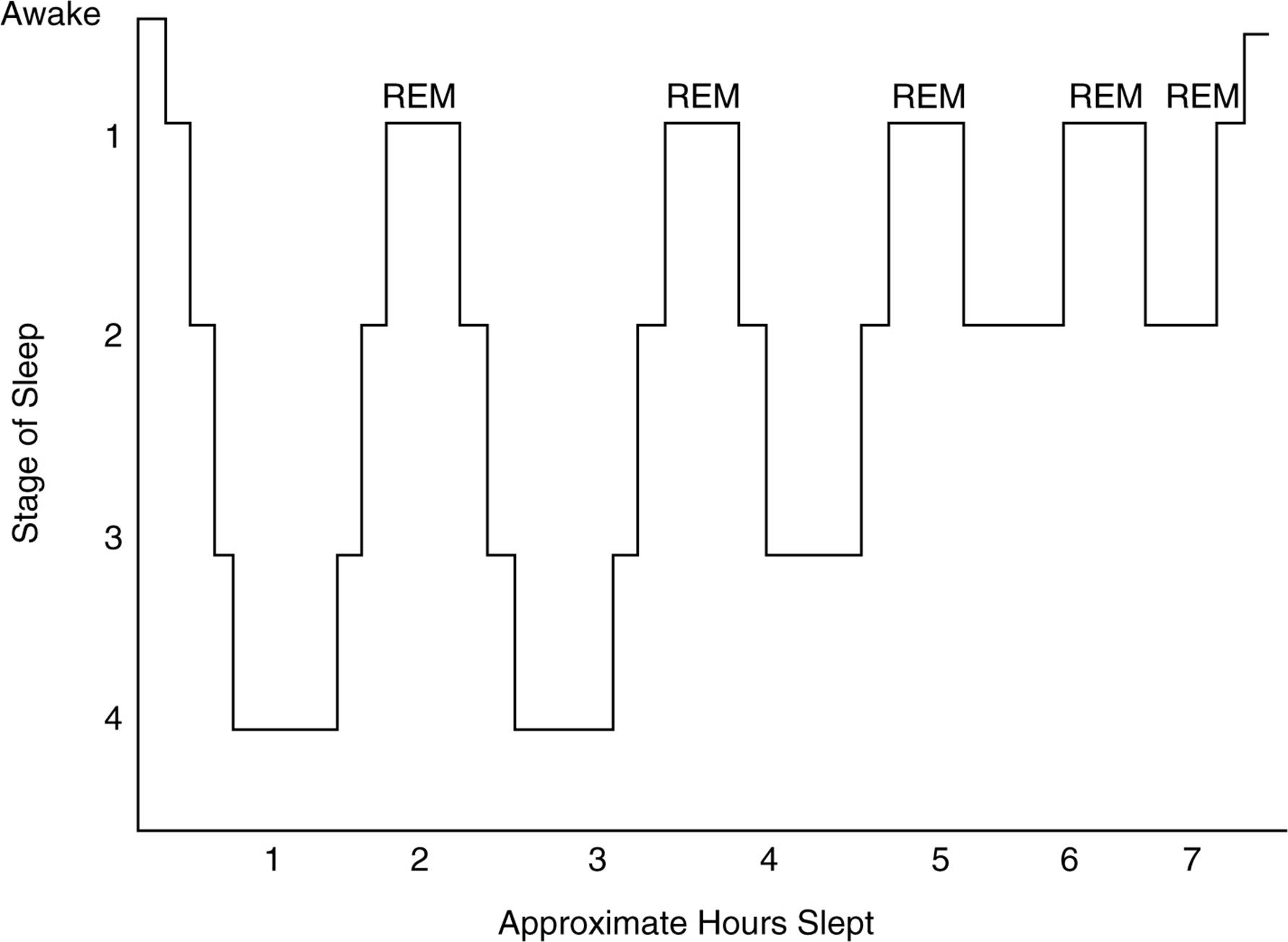
Figure 5.1. Stages of sleep.
Sleep Disorders
Many of us will experience a night, or perhaps a series of nights, of sleeplessness. These isolated periods of disruption in our sleep pattern give us an idea of the inconvenience and discomfort true sleep disorders can cause in people’s lives. Sleep researchers identify and diagnose several sleep disorders.
Insomnia is far and away the most common sleep disorder, affecting up to 10 percent of the population. An insomniac has persistent problems getting to sleep or staying asleep at night. Most people will experience occasional bouts of insomnia, but diagnosed insomniacs have problems getting to sleep more often than not. Insomnia is usually treated with suggestions for changes in 'text-align: justify;line-height:normal'>Narcolepsy occurs far more rarely than insomnia, occurring in less than 0.001 percent of the population. Narcoleptics suffer from periods of intense sleepiness and may fall asleep at unpredictable and inappropriate times. Narcoleptics may suddenly fall into REM sleep regardless of what they are doing at the time. One of my students suffered from narcolepsy from the time he was a preadolescent up until his graduation from high school. After he was finally diagnosed, he estimated that before his treatment he was drowsy almost his entire day except for two to three hours in the late afternoon. Narcolepsy can be successfully treated with medication and changing sleep patterns (usually involving naps at certain times of the day).
Sleep apnea may occur almost as commonly as insomnia and in some ways might be more serious. Apnea causes a person to stop breathing for short periods of time during the night. The body causes the person to wake up slightly and gasp for air, and then sleep continues. This process robs the person of deep sleep and causes tiredness and possible interference with attention and memory. Severe apnea can be fatal. Since these individuals do not remember waking up during the night, apnea frequently goes undiagnosed. Overweight men are at a higher risk for apnea. Apnea can be treated with a respiration machine that provides air for the person as he or she sleeps.
My mother tells me that I experienced night terrors as a child. I would sit up in bed in the middle of the night and scream and move around my room. Night terrors usually affect children, and most do not remember the episode when they wake up. The exact causes are not known, but night terrors are probably related in some way to somnambulism (sleep walking). They occur more commonly in children, and both phenomena occur during the first few hours of the night in stage 4 sleep. Most people stop having night terrors and episodes of somnambulism as they get older.
DREAMS
Dreams are the series of storylike images we experience as we sleep. Some people remember dreams frequently, sometimes more than one per night, while others are not aware of whether we dream or not. Some of us even report lucid dreams in which we are aware that we are dreaming and can control the storyline of the dream. Dreams are a difficult research area for psychologists because they rely almost entirely on self-reports. As mentioned previously, researchers know that if people are awakened during or shortly after an REM episode, they often report they were dreaming. Researchers theorize about the purposes and meanings of dreams. However, validating these theories is difficult with the limited access researchers currently have to dreams.
Sigmund Freud considered dreams an important tool in his therapy. Freudian psychoanalysis emphasizes dream interpretation as a method to uncover the repressed information in the unconscious mind. Freud said that dreams were wish fulfilling, meaning that in our dreams we act out our unconscious desires. This type of dream analysis emphasizes two levels of dream content. Manifest content is the literal content of our dreams. If you dream about showing up at school naked, the manifest content is your nudity, the room you see yourself in at school, the people present, and so on. More important to Freud was the latent content, which is the unconscious meaning of the manifest content. Freud thought that even during sleep, our ego protected us from the material in the unconscious mind (thus the term protected sleep) by presenting these repressed desires in the form of symbols. So showing up naked at school would represent a symbol in this type of analysis, perhaps of vulnerability or anxiety. This type of dream analysis is common. Check any bookstore, and you will find multiple dream interpretation books based on this theory. However, popularity does not imply validity. Researchers point out that this theory is difficult to validate or invalidate. How do we know which are the correct symbols to examine and what they mean? The validity of the theory cannot be tested. Consequently, this analysis is mostly used in psychoanalytic therapy and in pop psychology rather than in research.
The activation-synthesis theory of dreaming looks at dreams first as biological phenomena. Brain imaging proves that our brain is very active during REM sleep. This theory proposes that perhaps dreams are nothing more than the brain’s interpretations of what is happening physiologically during REM sleep. Researchers know that our minds are very good at explaining events, even when the events have a purely physiological cause. Split-brain patients (see Chapter 3) sometimes make up elaborate explanations for behaviors caused by their operation. Dreams may be a story made up by a literary part of our mind caused by the intense brain activity during REM sleep. According to this theory, dreams, while interesting, have no more meaning than any other physiological reflex in our body.
The information-processing theory of dreaming falls somewhere in between the Freudian and activation-synthesis theories. This theory points out that stress during the day will increase the number and intensity of dreams during the night. Also, most people report their dream content relates somehow to daily concerns. Proponents of information processing theorize that perhaps the brain is dealing with daily stress and information during REM dreams. The function of REM may be to integrate the information processed during the day into our memories. Babies may need more REM sleep than adults because they process so much new information every day.
HYPNOSIS
The high school where I teach usually hires a stage hypnotist to entertain at the postprom party. The day after students see the hypnotist’s show, I can expect dozens of questions about the process of hypnosis and whether it is a valid psychological phenomenon or some sort of trick. Many of the questions concern some of the curious powers hypnotism seems to have. One of these is posthypnotic amnesia, when people report forgetting events that occurred while they were hypnotized. The hypnotist may also implant a posthypnotic suggestion, a suggestion that a hypnotized person behave in a certain way after he or she is brought out of hypnosis. Like many other topics regarding consciousness, many questions about hypnosis are not completely answered. However, at least three theories attempt to explain what goes on during hypnosis.
Role theory states that hypnosis is not an alternate state of consciousness at all. This theory points out that some people are more easily hypnotized than others, a characteristic called hypnotic suggestibility. People with high hypnotic suggestibility share some other characteristics as well. They tend to have richer fantasy lives, follow directions well, and be able to focus intensely on a single task for a long period of time. These factors may indicate that hypnotism is a social phenomenon. Perhaps during hypnosis, people are acting out the role of a hypnotized person and following the suggestions of the hypnotist because that is what is expected of the role.
Other researchers use state theory to explain hypnosis. They point out that hypnosis meets some parts of the definition for an altered state of consciousness. Hypnotists seem to be able to suggest that we become more or less aware of our environments. In addition, some people report dramatic health benefits from hypnosis, such as pain control and reduction in specific physical ailments.
Researcher Ernest Hilgard explained hypnosis in a different way in his dissociation theory. According to Hilgard, hypnosis causes us to divide our consciousness voluntarily. One part or level of our consciousness responds to the suggestions of the hypnotist, while another part or level retains awareness of reality. In an experiment investigating hypnotism and pain control, Hilgard asked hypnotized participants to put their arm in an ice water bath. Most of us would feel this intense cold as painful after a few seconds, but the hypnotized participants reported no pain. However, when Hilgard asked them to lift their index finger if any part of them felt the pain, most participants lifted their finger. This experiment demonstrated the presence of a hidden observer, a part or level of our consciousness that monitors what is happening while another level obeys the hypnotist’s suggestions.
DRUGS
Psychoactive drugs are chemicals that change the chemistry of the brain (and the rest of the body) and induce an altered state of consciousness. Some of the behavioral and cognitive changes caused by these drugs are due to physiological processes, but some are due to expectations about the drug. Research shows that people will often exhibit some of the expected effects of the drug if they think they ingested it, even if they did not (this is similar to the placebo effect).
All psychoactive drugs change our consciousness through similar physiological processes in the brain. Normally, the brain is protected from harmful chemicals in the bloodstream by thicker walls surrounding the brain’s blood vessels. This is called the blood-brain barrier. However, the molecules that make up psychoactive drugs are small enough to pass through the blood-brain barrier. These molecules either mimic or block naturally occurring neurotransmitters in the brain. The drugs that mimic neurotransmitters are called agonists. These drugs fit in the receptor sites on a neuron that normally receive the neurotransmitter and function as that neurotransmitter normally would. The drugs that block neurotransmitters are called antagonists. These molecules also fit into receptor sites on a neuron. However, instead of acting like the neurotransmitter, they simply prevent the natural neurotransmitters from using that receptor site. Other drugs prevent natural neurotransmitters from being reabsorbed back into a neuron, creating an abundance of that neurotransmitter in the synapse. No matter what mechanism they use, drugs gradually alter the natural levels of neurotransmitters in the brain. The brain will produce less of a specific neurotransmitter if it is being artificially supplied by a psychoactive drug.
This change causes tolerance, a physiological change that produces a need for more of the same drug in order to achieve the same effect. Tolerance will eventually cause withdrawal symptoms in users. Withdrawal symptoms vary from drug to drug. They range from the headache I might get if I do not consume any caffeine during the day to the dehydrating and potentially fatal night sweats (sweating profusely during sleep) a heroin addict experiences during withdrawal. Dependence on psychoactive drugs can be either psychological or physical or can be both. Persons psychologically dependent on a drug feel an intense desire for the drug because they are convinced they need it in order to perform or feel a certain way. Persons physically dependent on a substance have a tolerance for the drug, experience withdrawal symptoms without it, and need the drug to avoid the withdrawal symptoms. Different researchers categorize psychoactive drugs in different ways, but four common categories are stimulants, depressants, hallucinogens, and opiates.
Caffeine, cocaine, amphetamines, and nicotine are common stimulants. Stimulants speed up body processes, including autonomic nervous system functions such as heart and respiration rate. This dramatic increase is accompanied by a sense of euphoria. The more-powerful stimulants, such as cocaine, produce an extreme euphoric rush that may make a user feel extremely self-confident and invincible. All stimulants produce tolerance, withdrawal effects, and other side effects (such as disturbed sleep, reduced appetite, increased anxiety, and heart problems) to a greater or lesser degree that corresponds with the power of the drug.
Depressants slow down the same body systems that stimulants speed up. Alcohol, barbiturates, and anxiolytics (also called tranquilizers or antianxiety drugs) like Valium are common depressants. Obviously, alcohol is by far the most commonly used depressant and psychoactive drug. A euphoria accompanies the depressing effects of depressants, as does tolerance and withdrawal symptoms. In addition, alcohol slows down our reactions and judgment by slowing down brain processes. The inhibition of different brain regions causes behavioral changes. For example, when enough alcohol is ingested to affect the cerebellum, our motor coordination is dramatically affected, eventually making it difficult or impossible for the user to even stand. Because it is so widespread, more research has been done on alcohol than on any other psychoactive drug.
Alcohol is categorized as a depressant because of its effect on our nervous system, even though some people report feeling more energized after ingesting a small amount of alcohol. This energizing effect is due to expectations about alcohol and because alcohol lowers inhibitions. Similarly, nicotine is a stimulant because it speeds up our nervous system, but some smokers smoke to relax.
Hallucinogens (also sometimes called psychedelics) do not necessarily speed up or slow down the body. These drugs cause changes in perceptions of reality, including sensory hallucinations, loss of identity, and vivid fantasies. Common hallucinogens include LSD, peyote, psilocybin mushrooms, and marijuana. One notable feature of hallucinogens is their persistence. Some amount of these drugs may remain in the body for weeks. If an individual ingests the hallucinogen again during this time period, the new dose of the chemical is added to the lingering amount, creating more profound and potentially dangerous effects. This effect is sometimes called reverse tolerance because the second dose may be less than the first but cause the same or greater effects. Effects of hallucinogens are less predictable than those of stimulants or depressants.
Opiates such as morphine, heroin, methadone, and codeine are all similar in chemical structure to opium, a drug derived from the poppy plant. The opiates all act as agonists for endorphins and thus are powerful painkillers and mood elevators. Opiates cause drowsiness and a euphoria associated with elevated endorphin levels. The opiates are some of the most physically addictive drugs because they rapidly change brain chemistry and create tolerance and withdrawal symptoms.
PRACTICE QUESTIONS
Directions: Each of the questions or incomplete statements below is followed by five suggested answers or completions. Select the one that is best in each case.
1.Agonists are psychoactive drugs that
(A)produce tolerance to the drug without the associated withdrawal symptoms.
(B)mimic and produce the same effect as certain neurotransmitters.
(C)mimic neurotransmitters and block their receptor sites.
(D)enhance the effects of certain opiates like heroin.
(E)make recovery from physical addiction more difficult.
2.In comparison with older people, babies
(A)sleep more fitfully; they tend to wake up more often.
(B)sleep more deeply; they spend more time in stage 3 and 4 sleep.
(C)spend more time in the REM stage than other sleep stages.
(D)spend more time in stage 1, which causes them to awaken easily.
(E)sleep more than young adults but less than people over 50.
3.Which of the following is the best analogy for how psychologists view consciousness?
(A)the on/off switch on a computer
(B)a circuit breaker that controls power to a house
(C)a fuse that allows electricity to pass through until a short circuit occurs
(D)a dimmer switch for a light fixture
(E)the ignition switch on a car
4.During a normal night’s sleep, how many times do we pass through the different stages of sleep?
(A)2
(B)2–3
(C)4–7
(D)8–11
(E)11–15
5.Which of the following is evidence supporting the role theory of hypnosis?
(A)People with rich fantasy lives are more hypnotizable.
(B)People will not behave under hypnosis in ways they would not without hypnosis.
(C)Hilgard’s experiment demonstrated the presence of a hidden observer.
(D)Our heart and respiration rates may differ while under hypnosis.
(E)Some therapists successfully use hypnosis in therapy.
6.Activation-synthesis theory tries to explain
(A)how consciousness emerges out of neural firings.
(B)how psychoactive drugs create euphoric effects.
(C)the origin and function of dreams.
(D)how our mind awakens us after we pass through all the sleep stages.
(E)how our consciousness synthesizes all the sensory information it receives.
7.Hilgard’s experiment that demonstrated the presence of a hidden observer is evidence for which theory?
(A)role theory of hypnosis
(B)levels theory of consciousness
(C)recuperative theory of sleep
(D)dissociation theory of hypnosis
(E)state theory of hypnosis
8.Which of the following two sleep disorders occur most commonly?
(A)insomnia and narcolepsy
(B)apnea and narcolepsy
(C)night terrors and apnea
(D)somnambulism and insomnia
(E)apnea and insomnia
9.Marijuana falls under what category of psychoactive drug?
(A)depressant
(B)mood elevator
(C)hallucinogen
(D)stimulant
(E)mood depressant
10.Night terrors and somnambulism usually occur during which stage of sleep?
(A)stage 1, close to wakefulness
(B)REM sleep
(C)REM sleep, but only later in the night when nightmares usually occur
(D)stage 4
(E)sleep onset
11.Which neurotransmitter is affected by opiates?
(A)serotonin
(B)endorphins
(C)dopamine
(D)GABA
(E)acetylcholine
12.In the context of this unit, the term tolerance refers to
(A)treatment of psychoactive drug addicts by peers and other members of society.
(B)the amount of sleep a person needs to function normally.
(C)the need for an elevated dose of a drug in order to get the same effect.
(D)the labeling of individuals automatically produced by the level of our consciousness.
(E)the harmful side effects of psychoactive drugs.
13.The information-processing theory says that dreams
(A)are meaningless by-products of how our brains process information during REM sleep.
(B)are symbolic representations of the information we encode during the day.
(C)are processed by one level of consciousness but other levels remain unaware of the dreams.
(D)occur during REM sleep as the brain deals with daily stress and events.
(E)occur only after stressful events, explaining why some people never dream.
14.Which level of consciousness controls involuntary body processes?
(A)preconscious level
(B)subconscious level
(C)unconscious level
(D)autonomic level
(E)nonconscious level
15.Professor Bohkle shows a group of participants a set of geometric shapes for a short period of time. Later, Professor Bohkle shows the same group a larger set of shapes that includes the first set of geometric shapes randomly distributed among the other new images. When asked which shapes they prefer, the participants choose shapes from the first group more often than the new images, even though they cannot remember which images they had seen previously. This experiment demonstrates which concept?
(A)priming
(B)mere-exposure effect
(C)shaping
(D)fundamental-attribution error
(E)primacy