CONCEPTS IN BIOLOGY
PART VI. PHYSIOLOGICAL PROCESSES
25. Nutrition. Food and Diet
25.6. Eating Disorders
The three most common health problems related to diet and patterns of food consumption are obesity, bulimia, and anorexia nervosa. All three disorders involve behaviors that lead to ill health. The causes of these behaviors are complex and often involve a strong psychological component. Metabolic imbalances may also contribute to the development of these disorders, particularly obesity. Culture has a strong influence on our perceptions of ourselves and influences our behavior. Some studies have shown that there is a tendency for members of a family to develop the same kinds of eating disorders. Therefore, it has been suggested that genetic factors influence the risk of developing eating disorders. On the other hand, members of the same family also are likely to develop patterns of eating related to culture and other factors. Eating disorders are often associated with psychological depression.
Obesity
Obesity is the condition of being overweight to the extent that a person’s health, quality of life, and life span are adversely affected (figure 25.8). Obesity occurs when people consistently take in more food energy than is necessary to meet their daily requirements. About 30% of the U.S. population is considered to be obese, based on their having a body mass index above 30 kg/m2. An obese person has a significantly increased risk for many diseases. In general, the higher the body mass index, the more significant the risk.

FIGURE 25.8. Obesity
Obesity is a serious health problem for about 30% of North Americans.
Determining Body Mass Index (BMI)
Body mass index (BMI) is a measure of body weight compared with height. BMI is calculated by determining a person’s weight (without clothing) in kilograms and their barefoot height in meters. The BMI is the weight in kilograms divided by height in meters squared:
(Appendix 1 of this book gives conversions to the metric system of measurements.) For example, a person with a height of 5 feet 6 inches (1.68 meters) who weighs 165 pounds (75 kilograms) has a body mass index of 26.6 kg/m2:

A person with a body mass index of less than 18.5 kg/m2 is considered to be underweight. A body mass index between 18.5 and 25 kg/m2 is considered a healthy weight; between 25 and 30 kg/m2overweight; and over 30 kg/m2 is considered obese. Figure 25.9 allows you to determine what weight category you are in.
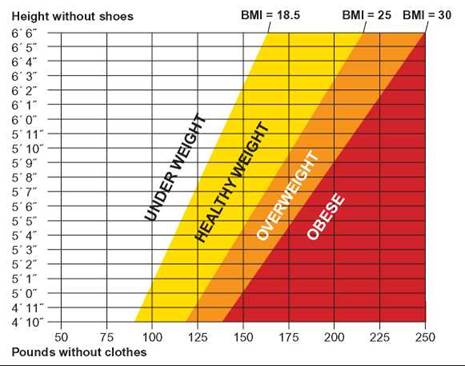
FIGURE 25.9. Body Mass Index
This graph allows you to determine which body mass index category you fall into.
Contributing Causes to Obesity
While all obese people have an imbalance between their food intake and their energy expenditure, the reasons for this imbalance are complex and varied. It appears that for most people, the imbalance is related to culture and lifestyle, although for some there are underlying biological reasons as well.
1. Cultural Influences Our culture encourages food consumption. Social occasions and business meetings frequently involve eating. It is clear that these and other cultural factors have much to do with the incidence of obesity. For example, obesity rates have increased over time, which strongly suggests that most cases of obesity are due to changes in lifestyle, not inherent biological factors. Furthermore, immigrants from countries with low rates of obesity show increased rates of obesity when they integrate into the American culture.
Snack foods are an important cultural influence. Snack foods typically have high amounts of sugars and fats. Consumption of these foods at other than meal times increases the total number of Calories consumed during the day. Furthermore, many of these foods are said to provide “empty Calories”—Calories are provided by sugar or fat but there is little or no other nutritional benefit (protein, vitamins, minerals, or fiber).
Restaurants play a role. Less than half the meals consumed in the United States are prepared in the home. This means that the consumer has reduced choices in the kind of food available, no control over the way foods are prepared, and little control over serving size. Meals prepared in restaurants and fast-food outlets emphasize meat and minimize the fruit, vegetable, and cereal portions, in direct contradiction to the Food Guide Pyramid. The methods of preparation also typically involve cooking with oils and serving with dressings or fat- containing condiments. In addition, portion sizes are generally much larger than recommended. Furthermore, restaurants and other food preparers have increased the size of portions significantly over the past 50 years. For example, in the 1950s, a fast-food serving of French fries was 2.4 ounces. Today, that size is still available, but it is the small size, and medium and large sizes contain two to three times the quantity of the small size.
An inactive lifestyle contributes to the incidence of obesity. Often, exercise is all that is needed to control a weight problem. In addition to increasing metabolism during the exercise itself, exercise tends to raise the basal metabolic rate for a period of time following exercise.
2. Psychological Factors Overeating is associated with a variety of psychological factors. Eating is a pleasurable activity and, as with all pleasurable activities, it is sometimes difficult to determine when to stop. Conversely, overeating also is often associated with depression.
3. Genetic and Metabolic Differences Recent discoveries of genes in mice suggest that there are genetic components that contribute to obesity. In one study, mice without a crucial gene gained an extraordinary amount of weight. There may be similar genes in humans. It is also clear that some people have much lower metabolic rates than most of the population and, therefore, need much less food than is typical. Still other obese individuals have a chemical imbalance of the nervous system that prevents them from feeling “full” until they have eaten an excessive amount of food. This imbalance prevents the brain from turning off the desire to eat. Research into the nature and action of this brain chemical indicates that, if obese people lacking this chemical receive it in pill form, they can feel “full” even when their food intake is decreased by 25% (Outlooks 25.2).
OUTLOOKS 25.2
The Genetic Basis of Obesity
Advances have been made in identifying the genetic and biochemical factors that regulate body weight. While not yet fully understood, a person's ability to regulate food intake and control body weight is at least partly controlled by the actions of several genes.
The molecules produced by these genes are messengers that control the flow of information between the stomach and nerve cells in a portion of the brain called the hypothalamus. This flow of information controls the appetite—whether one is hungry or not depends on how these cells are stimulated.
Several molecules are involved in this control:
1. Leptin is a hormone produced by white fat tissue; it is the product of the ob gene (formerly called the "obesity" gene). Leptin acts on nerve cells in the brain to regulate food intake. The absence of leptin causes severe obesity; the presence of leptin suppresses the appetite center of the brain. As a person's weight increases, the additional fat cells increase the production of leptin. In animals, the increase in leptin signals the brain to send signals that cause the animal to eat less and the body to do more. In humans, however, this does not appear to be the case, because many obese people have high levels of leptin and no suppression of appetite.
2. Neuropeptide Y (NPY) is a small protein that increases appetite. Leptin's appetite-suppressing effects may be due to the fact that leptin can inhibit NPY.
3. Alpha-melanocyte-stimulating hormone (a-MSH), which also increases production of the brown pigmentation of the skin, suppresses the appetite by acting on the hypothalamus. Leptin is believed to stimulate the production of a-MSH, which suppresses the appetite.
4. Melanin-concentrating hormone (MCH) is another neuropeptide. High levels of MCH in the brain increase food consumption and low levels decrease food consumption. Some believe that the smell of food may stimulate the production of MCH and enhance appetite. The gene for MCH is significantly more active in the brains of the obese.
5. Ghrelin is a growth hormone peptide secreted by the stomach. It has the opposite effect of leptin—it appears to be a powerful appetite stimulant.
Dealing with Obesity
Weight control is a matter of balancing the Calories ingested with the Calories expended by normal daily activities and exercise. The Food Guide Pyramid is clearly designed to provide information that will aid people in maintaining an appropriate weight.
Medical advice is important in dealing with obesity. Although it is likely that most cases of obesity do not involve underlying medical causes, it is wise to rule out that possibility before beginning a program to deal with obesity. Health practitioners are changing their view of obesity from one of blaming the obese person for lack of self-control to one of treating the condition as a chronic disease that requires a varied approach to control. For most people, dietary counseling and increased exercise are all that is needed, but some need psychological counseling, drug therapy, or surgery. Regardless, controlling obesity can be very difficult because it requires basic changes in a person’s eating habits, lifestyle, and value system.
Diet plans provide many different approaches to managing one’s diet to maintain an appropriate weight. Not all of these plans are the same, and not all are suitable to a particular situation. Some of these are based on solid nutritional and biological research while others are not. If a diet plan is to be valuable in promoting good health, it must satisfy a person’s needs in several ways. It must provide Calories and the nutrients important to good health. It should also contain readily available foods from all the basic food groups, and it should provide enough variety to prevent the person from becoming bored. In the final analysis, it should change how he or she eats.
Fad diets promise large, rapid weight loss but, in fact, may result only in temporary water loss. They may encourage eating and drinking foods that are diuretics, which increase the amount of urine produced and thus increase water loss. Or they may encourage exercise or other activities that cause people to lose water through sweating. Or they may simply encourage people to eat less for a period of time, which results in a temporary weight loss because there is less food in the gut.
Exercise should be a part of any program dealing with obesity. The health risks associated with being overweight or obese can be lessened by increasing one’s fitness. Fitness is a measure of how efficiently a person can function both physically and mentally. A person with a BMI of 30 kg/m2 may be more fit than someone with a BMI of 23 kg/m2 if he or she is involved in a regular program of physical and mental exercise. As fitness increases, so does metabolism, strength, mental acuity, and coordination. The use of body mass index to assess healthy weights is based on the assumption that excess weight is the result of fat tissue. In most cases this is true. However, since muscle is more dense than fat, very muscular people may have a high BMI and fall into the overweight or obese category when, in fact, they may not be.
An exercise program can involve organized exercise in sports or fitness programs. It can also include simple lifestyle changes, such as walking up stairs rather than taking an elevator, parking at the back of the parking lot so you walk farther, riding a bike for short errands, and walking down the hall to someone’s office rather than using the phone or e-mail.
Many people who initiate exercise plans as a way of reducing weight are frustrated because they initially gain weight rather than lose it. This is because a given volume of muscle weighs more than fat. Typically, they are “out of shape” and have low muscle mass. If they gain a pound of muscle at the same time they lose a pound of fat, they do not lose weight. However, if the fitness program continues, they will eventually stop increasing muscle mass and will lose weight. Even so, weight as muscle is more healthy than weight as fat.
Bulimia
Bulimia (“hunger of an ox”) is a disease condition in which the person engages in a cycle of eating binges followed by fasting or purging the body of the food by inducing vomiting or using laxatives (figure 25.10). The following are behaviors typically shown by bulimics:
• Excessive preoccupation with body image
• Excessive preoccupation with exercise
• Going to the bathroom after meals (to vomit)
• Hiding the fact that they are eating
• The use of laxatives or diuretics
• Irregular eating habits

FIGURE 25.10. Bulimia
Persons with bulimia go on eating binges followed by fasting or activities to get rid of food such as inducing vomiting, using laxatives, or using diuretics.
Many bulimics also use diuretics, which cause the body to lose water, resulting in the loss of weight. A bulimic person may induce vomiting physically or by using nonprescription drugs. Case studies have shown that some bulimics take 40 to 60 laxatives a day to rid themselves of food. For some, the laxatives become addictive.
Bulimics are usually of normal body weight or are overweight. Although women are more likely than men to become bulimic, there has been an increasing number of men with this disorder. The cause is thought to be psychological, stemming from depression or other psychological problems.
The binge-purge cycle and the associated use of diuretics and laxatives result in a variety of symptoms that can be deadly. It is often called the silent killer because it is difficult to detect. The following is a list of the major health problems observed in many bulimics:
• Excessive water loss
• Diminished blood volume
• Extreme mineral deficiencies
• Kidney malfunction
• Increased heart rate
• Loss of rhythmic heartbeat
• Lethargy
• Diarrhea
• Severe stomach cramps
• Damage to teeth and gums
• Loss of body proteins
• Migraine headaches
• Fainting spells
Anorexia Nervosa
Anorexia nervosa (figure 25.11) is a nutritional deficiency disease characterized by severe, prolonged weight loss as a result of a voluntary severe restriction in food intake. It is most common among adolescent and preadolescent women. An anorexic person’s fear of becoming overweight is so intense that, even though weight loss occurs, it does not lessen the fear of obesity, and the person continues to diet, even refusing to maintain the optimum body weight for his or her age, sex, and height. Persons who have this disorder have a distorted perception of their bodies. They see themselves as fat when, in fact, they are starving to death. Society’s preoccupation with body image, particularly among young people, may contribute to the incidence of this disease. Outlooks 25.3 describes an additional example of a problem with distorted body image. The following are some of the symptoms of anorexia nervosa:
Thin, dry, brittle hair
Degradation of fingernails Constipation
Amenorrhea (lack of menstrual periods)
Decreased heart rate
Loss of body proteins
Weaker than normal heartbeat
Calcium deficiency
Osteoporosis
Hypothermia (low body temperature)
Hypotension (low blood pressure)
Increased skin pigmentation
Reduction in the size of the uterus
Inflammatory bowel disease
Slowed reflexes Fainting
Weakened muscles
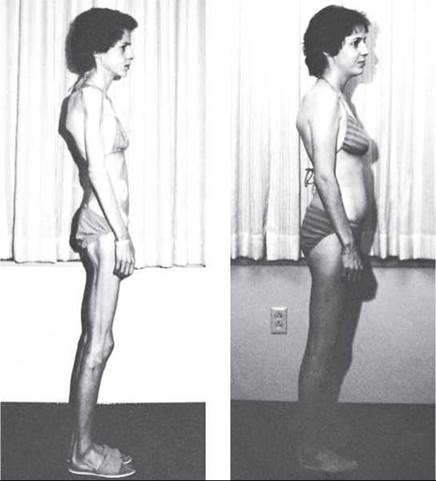
FIGURE 25.11. Anorexia Nervosa
Anorexia nervosa is a psychological eating disorder afflicting many Americans. These photographs were taken of an individual before and after treatment. Restoring a person with this disorder requires both medical and psychological efforts.
OUTLOOKS 25.3
Muscle Dysmorphia
A cousin to anorexia, muscle dysmorphia is an obsession with being muscular. Commonly called "big-orexia," it has been an under-diagnosed condition because, for men, being big is acceptable. Their muscles may be sculptured and bulging, yet no amount of persuasion can convince them their body is big enough. Those with this condition feel they are the objects of hate, resentment, fear, and loathing, and therefore must continue to "bulk up." To accomplish this, they exercise to the extreme and take anabolic steroids. Long-term use of these steroids, whether injectable or tablet form, can result in damage to the liver, heart, and muscles; raised cholesterol levels; mood swings; acne; enlarged breasts; and "'roid-rage." The common misconception about these steroids is that, when properly taken, they are safe. They are not.
25.6. CONCEPT REVIEW
10. What is BMI? How is it calculated?
11. What are the three primary eating disorders?
12. What is the role of leptin in controlling appetite?