Biology of Humans
13. Body Defense Mechanisms
In the previous two chapters we learned about the structure and function of the cardiovascular and lymphatic systems. We were introduced to white blood cells and their roles in body defenses. In this chapter, we study how the body reacts to the invasion of disease-causing organisms and substances that it perceives as threats. We see that there are three lines of defense. We also learn that the body can acquire long-lasting resistance to a microbe by becoming ill or by being immunized. Finally, we consider some potential problems caused by the immune system.
The Body’s Defense System
Your body generally defends you against anything that it does not recognize as being part of or belonging inside you. Common targets of your defense system include organisms that cause disease or infection and body cells that have turned cancerous.
The bacteria, viruses, protozoans, fungi, parasitic worms, and prions (infectious proteins) that cause disease are called pathogens (discussed further in Chapter 13a). Note that this term does not apply to most of the microorganisms we encounter. Many bacteria, for example, are actually beneficial. They flavor our cheese, help rid the planet of corpses through decomposition, and help keep other, potentially harmful bacteria in check within our bodies. Indeed, certain bacteria are essential because they decompose dead material, thereby recycling nutrients to support new life.
Cancerous cells also threaten our well-being. A cancer cell was once a normal body cell, but because of changes in its genes, it can no longer regulate its cell division. If left unchecked, these renegade cells can multiply until they take over the body, upsetting its balance, choking its pathways, and ultimately causing great pain and sometimes death.
· Fever, one of the body's defense mechanisms, helps us fight bacterial infections.
Three Lines of Defense
The body has three strategies for defending against foreign organisms and molecules or cancer cells.
1. Keep the foreign organisms or molecules out of the body in the first place. This is accomplished by the first line of defense—chemical and physical surface barriers.
2. Attack any foreign organism or molecule or cancer cell inside the body. The second line of defense consists of internal cellular and chemical defenses that become active if the surface barriers are penetrated.
3. Destroy a specific type of foreign organism or molecule or cancer cell inside the body. The third line of defense is the immune response, which destroys specific targets (usually disease-causing organisms) and remembers those targets so that a quick response can be mounted if they enter the body again.
Thus, the first and second lines of defense consist of nonspecific mechanisms that are effective against any foreign organisms or substances. We are born with these defense mechanisms, so they are described as innate responses. We acquire the third line of defense, the immune response, which is an adaptive, specific mechanism of defense. We acquire adaptive immunity when we are exposed to chemicals and organisms that are not recognized as belonging in the body. The three lines of defense against pathogens are summarized in Figure 13.1.

FIGURE 13.1. The body's three lines of defense against pathogens
First Line of Innate Defense: Physical and Chemical Barriers
The skin and mucous membranes that form the first line of defense are physical barriers that help keep foreign substances from entering the body (Figure 13.2). In addition, they produce several protective chemicals.
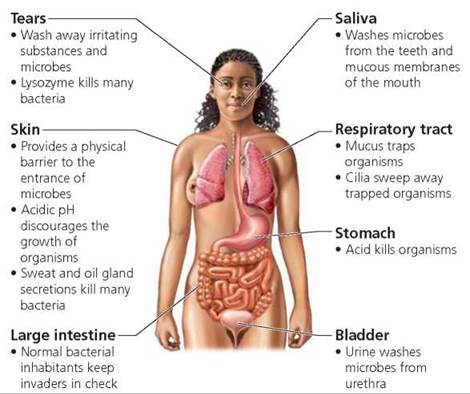
FIGURE 13.2. The body's first line of defense consists of physical and chemical barriers that serve as innate, nonspecific defenses against any threats to our well-being. Collectively, they prevent many invading organisms and substances from entering the body, or confine them to a local region, kill them, remove them, or slow their growth.
Physical barriers. Like a suit of armor, unbroken skin helps shield the body from pathogens by providing a barrier to foreign substances. A layer of dead cells forms the tough outer layer of skin. These cells are filled with the fibrous protein keratin, which waterproofs the skin and makes it resistant to the disruptive toxins (poisons) and enzymes of most would- be invaders. Some of the strength of this barrier results from the tight connections binding the cells together. What is more, the dead cells are continuously shed and replaced, at the rate of about a million cells every 40 minutes. As dead cells flake off, they take with them any microbes that have somehow managed to latch on. Another physical barrier, the mucous membranes lining the digestive and respiratory passages, produces sticky mucus that traps many microbes and prevents them from fully entering the body. The cells of the mucous membranes of the upper respiratory airways have cilia—short, hairlike structures that beat constantly. This beating moves the contaminated mucus to the throat. We eliminate the mucus in the throat by swallowing, coughing, or sneezing.
Chemical barriers The skin also provides chemical protection against invaders. Sweat and oil produced by glands in the skin wash away microbes. Moreover, the acidity of the secretions slows bacterial growth, and the oils contain chemicals that kill some bacteria.
Other chemical barriers include the lining of the stomach, which produces hydrochloric acid and protein-digesting enzymes that destroy many pathogens. Beneficial bacteria in a woman's vagina create an acidic environment that discourages the growth of some pathogens. The acidity of urine slows bacterial growth. (Urine also works as a physical barrier, flushing microbes from the lower urinary tract.) Saliva and tears contain an enzyme called lysozyme that kills some bacteria by disrupting their cell walls.
Stop and think
Harmful bacteria within the digestive system often cause diarrhea. How might this be a protective response of the body?
Second Line of Innate Defense: Defensive Cells and Proteins, Inflammation, and Fever
The second line of defense consists of nonspecific internal defenses against any pathogen that breaks through the physical and chemical barriers and enters the body. This second line of defense includes defensive cells and proteins, inflammation, and fever (see Table 13.1).
TABLE 13.1. The Second Line of Defense—Innate, Nonspecific Internal Defenses
Defense |
Example |
Function |
Defensive cells |
Phagocytic cells such as neutrophils and macrophages |
Engulf invading organisms |
Eosinophils |
Kill parasites |
|
Natural killer cells |
Kill many invading organisms and cancer cells |
|
Defensive proteins |
Interferons |
Slow the spread of viruses in the body |
Complement system |
Stimulates histamine release; promotes phagocytosis; kills bacteria; enhances inflammation |
|
Inflammation |
Widening of blood vessels and increased capillary permeability, leading to redness, heat, swelling, and pain |
Brings in defensive cells and speeds healing |
Fever |
Abnormally high body temperature |
Slows the growth of bacteria; speeds up body defenses |
Defensive cells. Specialized "scavenger" cells called phagocytes (phage, to eat; cyte, cell) engulf pathogens, damaged tissue, or dead cells by the process of phagocytosis (Chapter 3). This class of white blood cells serves not only as the front-line soldiers in the body's internal defense system but also as janitors that clean up debris. When a phagocyte encounters a foreign particle, cytoplasmic extensions flow from the phagocytic cell, bind to the particle, and pull it inside the cell. Once inside the cell, the particle is enclosed within a membrane-bound vesicle and quickly destroyed by digestive enzymes.
The body has several types of phagocytes. One type, neutrophils, arrives at the site of attack before the other types of white blood cells and immediately begins to consume the pathogens, especially bacteria, by phagocytosis. Other white blood cells (monocytes) leave the vessels of the circulatory system and enter the tissue fluids, where they develop into large macrophages (macro, big; phage, to eat). Macrophages have hearty and less discriminating appetites than neutrophils do, and they attack and consume virtually anything that is not recognized as belonging in the body—including viruses, bacteria, and damaged tissue (Figure 13.3).

FIGURE 13.3. A macrophage ingesting a bacterium (the rod-shaped structure). The bacterium will be pulled inside the cell within a membrane-bound vesicle and quickly killed.
A second type of white blood cell, eosinophils, attacks pathogens that are too large to be consumed by phagocytosis, such as parasitic worms. Eosinophils get close to the parasite and discharge enzymes that destroy the organism. Macrophages then remove the debris.
Natural killer cells. A third type of white blood cell, called natural killer (NK) cells, roams the body in search of abnormal cells and quickly orchestrates their death. In a sense, NK cells function as the body's police walking a beat. They are not seeking a specific villain. Instead, they respond to any suspicious character, including a cell whose cell membrane has been altered by the addition of proteins that are unfamiliar to the NK cell. The prime targets of NK cells are cancerous cells and cells infected with viruses. Cancerous cells routinely form but are quickly destroyed by NK cells and prevented from spreading (Figure 13.4).
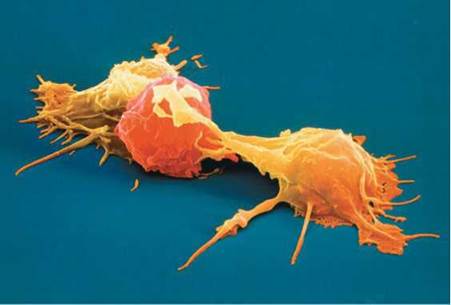
FIGURE 13.4. Natural killer cells (shown in orange) attacking a leukemia cell (shown in red). NK cells patrol the body, bumping and touching other cells as they go. When NK cells contact a cell with an altered cell surface, such as a cancer cell or a virus-infected cell, a series of events is immediately initiated. The NK cell attaches to the target cell and releases proteins that create pores in the target cell, making the membrane leaky and causing the cell to burst.
As soon as it touches a cell with an abnormal surface, the NK cell attaches to the abnormal cell and delivers a "kiss of death" in the form of proteins that create many pores in the target cell. The pores make the target cell "leaky," so that it can no longer maintain a constant internal environment and eventually bursts.
Defensive proteins. The second line of defense also includes defensive proteins. We will discuss two types of defensive proteins: interferons, which slow viral reproduction, and the complement system, which assists other defensive mechanisms.
Interferons. A cell that has been infected with a virus can do little to help itself. But cells infected with a virus can help cells that are not yet infected. Before certain virally infected cells die, they secrete small proteins called interferons that act to slow the spread of viruses already in the body. As the name implies, interferons interfere with viral activity.
Interferons mount a two-pronged attack. First, they help rid the body of virus-infected cells by attracting macrophages and NK cells that destroy the infected cells immediately. Second, interferons protect cells that are not yet infected with the virus. When released, an interferon diffuses to neighboring cells and stimulates them to produce proteins that prevent viruses from replicating in those cells. Because viruses cause disease by replicating inside body cells, preventing replication curbs the disease. Interferon helps protect uninfected cells from all strains of viruses, not just the one responsible for the initial infection.
Pharmaceutical preparations of interferon have been shown to be effective against certain cancers and viral infections. Interferons inhibit cell division of cancer cells. For instance, interferon is often successful in combating a rare form of leukemia (hairy cell leukemia) and Kaposi's sarcoma, a form of cancer that often occurs in people with AIDS. Interferon has also been approved for treating the hepatitis C virus, which can cause cirrhosis of the liver and liver cancer; the human papillomavirus (HPV), which causes genital warts and cervical cancer; and the herpes virus, which causes genital herpes.
Complement system. The complement system, or simply complement, is a group of at least 20 proteins whose activities enhance, or complement, the body's other defense mechanisms. Until these proteins are activated by infection, they circulate in the blood in an inactive state. Once activated, these proteins enhance both nonspecific and specific defense mechanisms. The effects of complement include the following:
• Destruction of pathogen. Complement can act directly by punching holes in a target cell's membrane (Figure 13.5) so that the cell is no longer able to maintain a constant internal environment. Just as when NK cells secrete proteins that make a target cell's membrane leaky, water enters the cell, causing it to burst.
• Enhancement of phagocytosis. Complement enhances phagocytosis in two ways. First, complement proteins attract macrophages and neutrophils to the site of infection to remove the foreign cells. Second, one of the complement proteins binds to the surface of the microbe, making it easier for macrophages and neutrophils to "get a grip" on the intruder and devour it.
• Stimulation of inflammation. Complement also causes blood vessels to widen and become more permeable. These changes provide increased blood flow to the area and increased access for white blood cells.
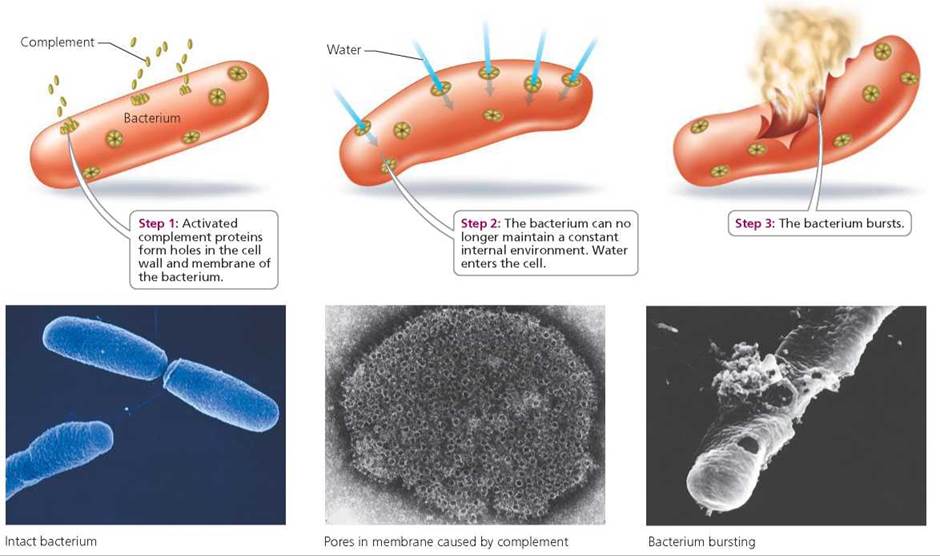
FIGURE 13.5. Complement has a direct destructive effect on pathogens.
Inflammation. When body tissues are injured or damaged, a series of events called the inflammatory response or reaction occurs. This response destroys invaders and helps repair and restore damaged tissue. The four cardinal signs of inflammation that occur at the site of a wound are redness, heat (or warmth), swelling, and pain. These signs announce that certain cells and chemicals have combined efforts to contain infection, clean up the damaged area, and heal the wound. Let's consider the causes of the cardinal signs and how they are related to the benefits of inflammation.
• Redness. Redness occurs because blood vessels dilate (widen) in the damaged area, causing blood flow in this area to increase. The dilation is caused by histamine, a substance that is also released during allergic reactions (discussed later in the chapter). Histamine is released by small, mobile connective tissue cells called mast cells in response to chemicals from damaged cells.
The increased blood flow to the site of injury delivers phagocytes, blood-clotting proteins, and defensive proteins, including complement and antibodies. At the same time, the increased blood flow washes away dead cells and toxins produced by the invading microbes.
• Heat. The increased blood flow also elevates the temperature in the area of injury. The elevated temperature increases the metabolic rate of the body cells in the region and speeds healing. Heat also increases the activities of phagocytic cells and other defensive cells.
• Swelling. The injured area swells because histamine also makes capillaries more permeable, or leakier, than usual. Fluid seeps into the tissues from the bloodstream, bringing with it many beneficial substances. Bloodclotting factors enter the injured area and begin to wall off the region, thereby helping to protect surrounding areas from injury and preventing excessive loss of blood. The seepage also increases the oxygen and nutrient supply to the cells. If the injured area is a joint, swelling can hamper movement—an effect that might seem to be an inconvenience, but it permits the injured joint to rest and recover.
• Pain. There are several causes for the pain in an inflamed area. For example, the excessive fluid that has leaked into the tissue presses on nerves and contributes to the sensation of pain. Some soreness might be caused by bacterial toxins, which can kill body cells. Injured cells also release pain-causing chemicals, such as prostaglandins. Pain usually causes a person to protect the area to avoid additional injury.
Because of the wider blood vessels and increased capillary permeability that bring about the inflammatory response, phagocytes begin to swarm to the injured site, attracted by chemicals released when tissue is damaged. Within minutes, the neutrophils squeeze through capillary walls into the fluid around cells and begin engulfing pathogens, toxins, and dead body cells. Soon macrophages arrive and continue the body's counterattack for the long term. Macrophages are also important in cleaning debris, such as dead body cells, from the damaged area. As the recovery from infection continues, dead cells (including microbes), body tissue cells, and phagocytes may begin to ooze from the wound as pus (Figure 13.6).
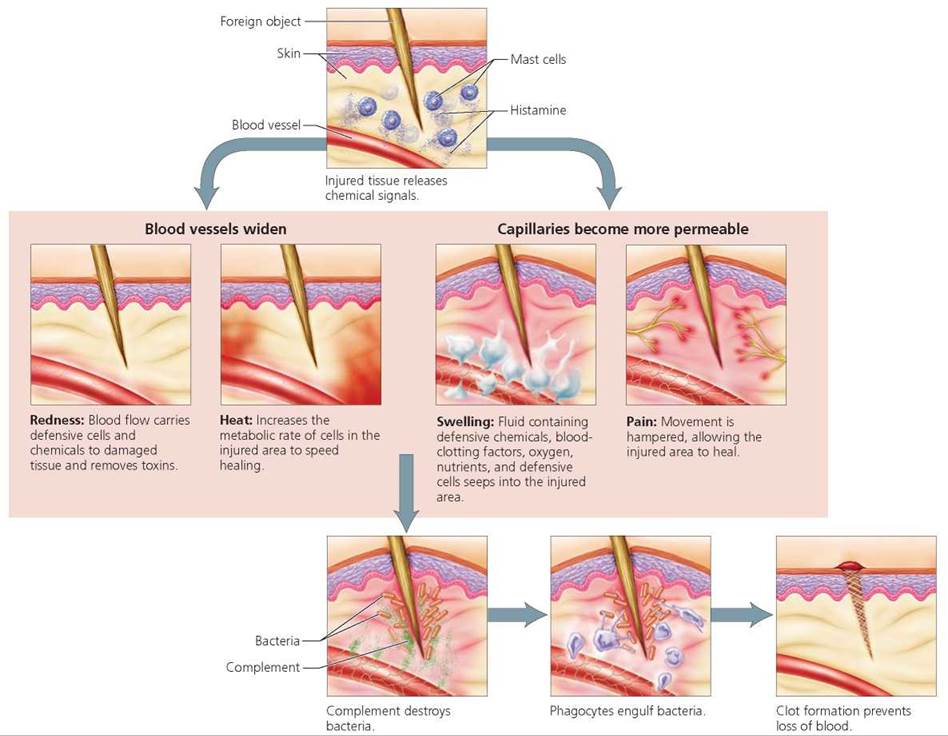
FIGURE 13.6. The inflammatory response is a general response to tissue injury or invasion by foreign microbes. It serves to defend against pathogens and to clear the injured area of pathogens and dead body cells, allowing repair and healing to occur. The four cardinal signs of inflammation are redness, heat, swelling, and pain.
Fever A fever is an abnormally high body temperature (Figure 13.7). Fevers are caused by pyrogens (pyro, fire; gen, producer), chemicals that raise the "thermostat" in the brain (the hypothalamus) to a higher set point. Bacteria release toxins that sometimes act as pyrogens. It is interesting to note, however, that the body produces its own pyrogens as part of its defensive strategy. Regardless of the source, pyrogens have the same effect on the hypothalamus, raising the set point so that physiological responses, such as shivering, are initiated to raise body temperature (as discussed in Chapter 4). Thus, we have the chills while the fever is rising. When the set point is lowered, the fever breaks and physiological responses such as perspiring reduce the body temperature until it reaches the new set point.

FIGURE 13.7. Although a fever might make us feel uncomfortable, it can help the body fight disease.
A mild or moderate fever helps the body fight bacterial infections by slowing the growth of bacteria and stimulating body defense responses. Bacterial growth is slowed because a mild fever causes the liver and spleen to remove iron from the blood, and many bacteria require iron to reproduce. Fever also increases the metabolic rate of body cells; the higher rate speeds up defensive responses and repair processes. On the other hand, a very high fever (over 105°F, or 40.6°C) is dangerous. It can inactivate enzymes needed for biochemical reactions within body cells.
Third Line of Defense: Adaptive Immune Response
When the body's first and second lines of defense fail to stop a pathogen, the body's specific defenses respond and target the particular pathogen, cancer cell, or foreign molecule that has entered the body. The third line of defense, the immune system, provides the specific responses and memory. The organs of the lymphatic system (see Chapter 12) are important components of the immune system because they produce the various cells responsible for immunity. The immune system is not an organ system in an anatomical sense. Instead, the immune system is defined by its function: recognizing and destroying specific pathogens or foreign molecules. The body's specific defenses working together are called an adaptive immune response.
There are several important characteristics of an adaptive immune response. First, an adaptive immune response is directed at a particular pathogen. For example, the immune system of a child infected with measles recognizes the measles virus as a foreign substance (not belonging in the body) and then acts to immobilize, neutralize, or destroy it. An effective immune system will enable the child to recover from the illness. Second, the immune system has memory. If the same child is again exposed to the same pathogen years later, the immune system remembers the pathogen and attacks it so quickly and vigorously that the child will not become ill with measles a second time.
Distinguishing Self from Nonself
To defend against a foreign organism or molecule, the body must be able distinguish it from a body cell and recognize it as foreign. This ability depends on the fact that each cell in your body has special molecules embedded in the plasma membrane that label the cell as self. These molecules serve as flags declaring the cell as a "friend." The molecules are called MHC markers, named for the major histocompatibility complex genes that code for them. The self labels on your cells are different from those of any other person (except an identical twin) as well as from those of other organisms, including pathogens. The immune system uses these labels to distinguish between what is part of your body and what is not (Figure 13.8). It doesn't attack cells that are recognized as self.
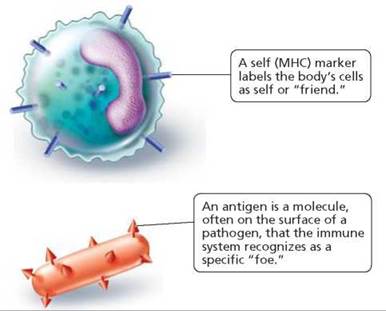
FIGURE 13.8. All nucleated cells in the body have molecular MHC markers on their surface that label them as self. Foreign substances, including potential disease-causing organisms, have molecules on their surfaces that are not recognized as belonging in the body. Foreign molecules that are capable of triggering an adaptive immune response are called antigens.
A nonself substance or organism that triggers an immune response is called an antigen. Because an antigen is not recognized as belonging in the body, the immune system directs an attack against it. Typically, antigens are large molecules, such as proteins, polysaccharides, or nucleic acids. Often, antigens are found on the surface of an invader—embedded in the plasma membrane of an unwelcome bacterial cell, for instance, or part of the protein coat of a virus. However, pieces of invaders and chemicals secreted by invaders, such as bacterial toxins, can also serve as antigens. Each antigen is recognized by its shape.
Certain white blood cells, called lymphocytes, are responsible for both the specificity and the memory of the adaptive immune response. There are two principal types of lymphocytes: B lymphocytes, or more simply B cells, and T lymphocytes, or T cells. Both types form in the bone marrow, but they mature in different organs of the body. It is thought that B cells mature in the bone marrow. The T cells, on the other hand, mature in the thymus gland, which overlies the heart.
As the T lymphocytes mature, they develop the ability to distinguish between cells that belong in the body and those that do not. The T cells must be able to recognize the specific MHC self markers of that person and not respond vigorously to cells bearing that MHC self marker. If T cells do respond to cells with those self markers, the T cells are destroyed. Once they are mature, T lymphocytes circulate through the body, bumping into other cells and checking to be sure those cells have the correct self (MHC) marker. Cells with proper MHC markers are passed by.
In addition, both T and B lymphocytes, as they mature, are programmed to recognize one particular type of antigen. This recognition is the basis of the specificity of the adaptive immune response. Each lymphocyte develops its own particular receptors—molecules having a unique shape—on its surface. Thousands of identical receptor molecules pepper the surface of each lymphocyte, and they are unlike the receptor molecules on other lymphocytes. When an antigen fits into a lymphocyte's receptors, much like a key into a lock, the body's defenses target that particular antigen. Due to the tremendous diversity of receptor molecules, each type occurring on a different lymphocyte, a few of the billions of lymphocytes in your body are able to respond to each of the thousands of different antigens that you will be exposed to in your lifetime.
When an antigen is detected, B cells and T cells bearing receptors able to respond to that particular invader are stimulated to divide repeatedly, forming two lines of cells. One line of descendant cells is made up of effector cells, which carry out the attack on the enemy. Effector cells generally live for only a few days. Thus, after the invader has been eliminated from the body, the number of effector cells declines. The other line of descendant cells is composed of memory cells, long-lived cells that "remember" that particular invader and mount a rapid, intense response to it if it should ever appear again. The quick response of memory cells is the mechanism that prevents you from getting ill from the same pathogen twice.
Antibody-Mediated Responses and Cell-Mediated Responses
An analogy can be made between the body's immune defenses and a nation's military defense system. The military has scouts who look for invaders. If an invader is found, the scout alerts the commander of the military forces and provides an exact description of the villain. The scout must also provide the appropriate password so that the commander knows he or she is not a spy planting misinformation. The body also has scouts, called macrophages, that are part of the nonspecific defenses. Macrophages roam the tissues, looking for any invader. The cells that act as the immune system's commander are a subset of T cells called helper T cells. When macrophages properly alert helper T cells they respond by calling out the body's specific defensive forces, and the adaptive immune responses begin.
A nation's military may have two (or more) branches. For example, it may consist of an army and a navy. Specialized to respond in slightly different ways to enemy invasion, each branch is armed with certain types of weapons. Either branch can be activated to combat a particular threat, say little green people with purple hair. The navy may be called into action if the enemy is encountered at sea, whereas the army will come to the defense if the enemy is on land.
The body, similarly, has two types of specific defenses. These specific defenses recognize the same antigens and destroy the same invaders, but they do so in different ways.
• Antibody-mediated immune responses defend primarily against antigens found traveling freely in intercellular and other body fluids—for example, toxins or extracellular pathogens such as bacteria or free viruses. The warriors of this branch of immune defense are the effector B cells (also called plasma cells), and their weapons are Y-shaped proteins called antibodies, which neutralize and remove potential threats from the body. Antibodies are programmed to recognize and bind to the antigen posing the threat; they help eliminate the antigen from the body. We discuss how this works in greater detail later in the chapter.
• Cell-mediated immune responses protect against cellular pathogens or abnormal cells, including body cells that have become infected with viruses or other pathogens and cancer cells. The lymphocytes responsible for cell-mediated immune responses are a type of T cell called cytotoxic T cell (discussed at greater length later in the chapter). Once activated, cytotoxic T cells quickly destroy the cellular pathogen, infected body cells, or cancerous cells by causing them to burst.
Now that the various defenders have been introduced, let's see how they work together to produce your body's highly effective immune response. Table 13.2 summarizes the functions of the cells participating in the adaptive immune response, and Table 13.3 summarizes the steps in the adaptive immune response.
TABLE 13.2. Cells Involved in the Adaptive Immune Response
Cell |
Functions |
Macrophage |
An antigen-presenting cell • Engulfs and digests pathogen or invader • Places a piece of digested antigen on its plasma membrane • Presents the antigen to a helper T cell • Activates the helper T cell |
T Cells |
|
Helper T cell |
The “on” switch for both lines of immune response • After activation by macrophage, it divides, forming effector helper T cells and memory helper T cells • Helper T cells activate B cells and T cells |
Cytotoxic T cell (effector T cell) |
Responsible for cell-mediated immune responses • When activated by helper T cells, it divides to form effector cytotoxic T cells and memory cytotoxic T cells • Destroys cellular targets, such as infected body cells, bacteria, and cancer cells |
Suppressor T cell |
The “off” switch for both lines of immune responses • Suppresses the activity of the B cells and T cells after the foreign cell or molecule has been successfully destroyed |
B Cells |
Involved in antibody-mediated responses • When activated by helper T cells, it divides to form plasma cells and memory cells |
Plasma cell |
Effector in antibody-mediated response • Secretes antibodies specific to extracellular antigens, such as toxins, bacteria, and free viruses |
Memory Cells |
Responsible for memory of immune system • Generated by B cells or any type of T cell during an immune response • Enable quick and efficient response on subsequent exposures of the antigen • May live for years |
TABLE 13.3. Steps in the Adaptive Immune Response
Step 1: Threat |
Foreign cell or molecule enters the body |
Step 2: Detection |
• Macrophage detects foreign cell or molecule and engulfs it |
Step 3: Alert |
• Macrophage puts antigen from the pathogen on its surface and finds the helper T cell with correct receptors for that antigen |
• Macrophage presents antigen to the helper T cell |
|
• Macrophage alerts the helper T cell that there is an invader that “looks like” the antigen |
|
• Macrophage activates the helper T cell |
|
Step 4: Alarm |
Helper T cell activates both lines of defense to fight that specific antigen |
Step 5: Building specific defenses (clonal selection) |
• Antibody-mediated defense—B cells are activated and divide to form plasma cells that secrete antibodies specific to the antigen • Cell-mediated defense—T cells divide to form cytotoxic T cells that attack cells with the specific antigen |
Step 6: Defense |
• Antibody-mediated defense—antibodies specific to the antigen eliminate the antigen • Cell-mediated defense—cytotoxic T cells cause cells with the antigen to burst |
Step 7: Continued surveillance |
Memory cells formed when helper T cells, cytotoxic T cells, and B cells were activated remain to provide swift response if the antigen is detected again |
Step 8: Withdrawal of forces |
Once the antigen has been destroyed, suppressor T cells shut down the immune response to that antigen |
Steps of the Adaptive Immune Response
Although the cell-mediated immune response and the antibody- mediated immune response use different mechanisms to defend against pathogens or foreign molecules (nonself), the general steps in these responses are the same (Figure 13.9).
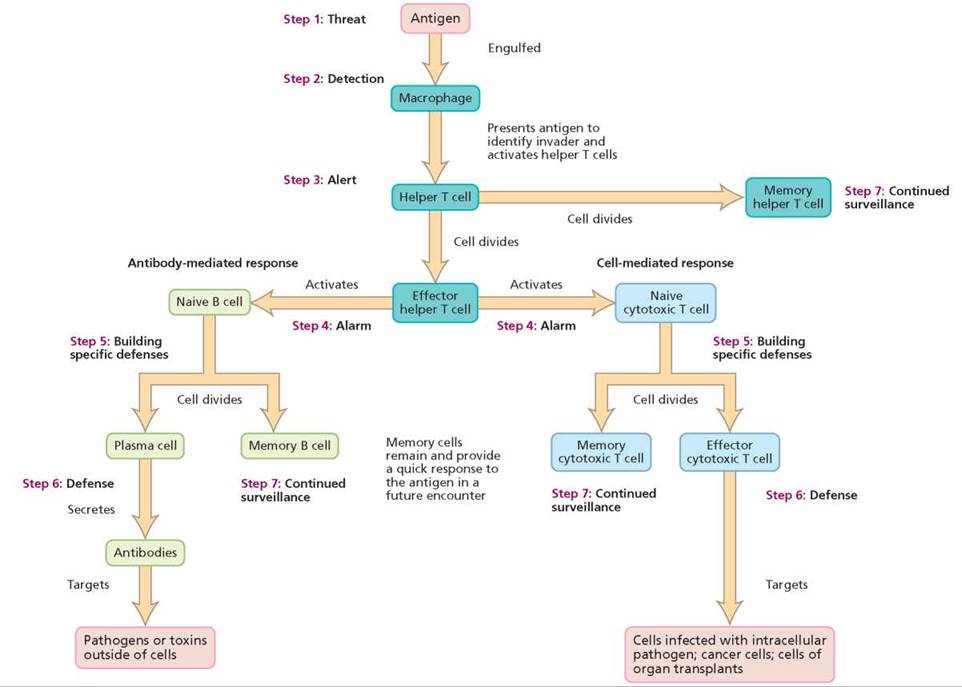
FIGURE 13.9. An overview of the adaptive immune response
Why are helper T cells critical to the adaptive immune response?
Helper T cells activate both naive cytotoxic T cells and naive B cells. Thus, helper T cells turn on both the cell-mediated and the antibody-mediated adaptive immune responses.
Threat. The adaptive immune response begins when a molecule or organism (an antigen) lacking the self (MHC) marker manages to evade the first two lines of defense and enters the body (Figure 13.10).
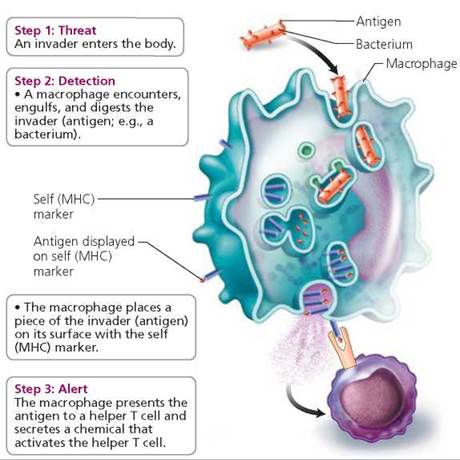
FIGURE 13.10. A macrophage is an important antigen-presenting cell. It presents the antigen, which is attached to a self (MHC) marker, to a helper T cell, and activates the helper T cell.
Detection. Recall that macrophages are phagocytic cells that roam the body, engulfing any foreign material or organisms they may encounter. Within the macrophage, the engulfed material is digested into smaller pieces.
Alert. The macrophage then alerts the immune system's commander, a helper T cell, that an antigen is present. The macrophage accomplishes this task by transporting some of the digested pieces to its own surface, where they bind to the MHC self markers on the macrophage membrane. The self marker acts as a secret password that identifies the macrophage as a "friend." On the other hand, the antigen bound to the self markers function as a kind of wanted poster, telling the lymphocytes that there is an invader and revealing how the invader can be identified. The displayed antigens trigger the immune response. Thus, the macrophage is an important type of antigen-presenting cell (APC). (B cells and dendritic cells— cells with long extensions found in lymph nodes—are two other kinds of antigen-presenting cells.)
The macrophage presents the antigen to a helper T cell, the kind of T cell that serves as the main switch for the entire adaptive immune response. However, the macrophage must alert the right kind of helper T cell—a helper T cell bearing receptors that recognize the specific antigen being presented. These specific helper T cells constitute only a tiny fraction of the entire T cell population. Finding the right helper T cell is like looking for a needle in a haystack. The macrophage wanders through the body until it literally bumps into an appropriate helper T cell. The encounter most likely occurs in one of the lymph nodes, because these bean-shaped structures, discussed in Chapter 12, contain huge numbers of lymphocytes of all kinds. When the antigen-presenting macrophage meets the appropriate helper T cell and binds to it, the macrophage secretes a chemical that activates the helper T cell.
Alarm. Within hours, an activated helper T cell begins to secrete its own chemical messages. The helper T cell's message calls into active duty the appropriate B cells and T cells—those with the ability to bind to the particular antigen that triggered the response.
Building Specific Defenses. When the appropriate "naive"1 B cells or T cells are activated, they begin to divide repeatedly. The result is a clone (a population of genetically identical cells) that is specialized to protect against the particular target antigen.
The process by which this highly specialized clone is produced, called clonal selection, underlies the entire adaptive immune response (Figure 13.11). We have seen that each lymphocyte is equipped to recognize an antigen of a specific shape. Any antigen that enters the body will be recognized by only a few lymphocytes at most. By binding to the receptors on a lymphocyte's surface, an antigen selects a lymphocyte that was preprogrammed during its maturation with receptors able to recognize that particular antigen. That particular lymphocyte is then stimulated to divide and produces a clone of millions of identical cells able to recognize that same antigen.
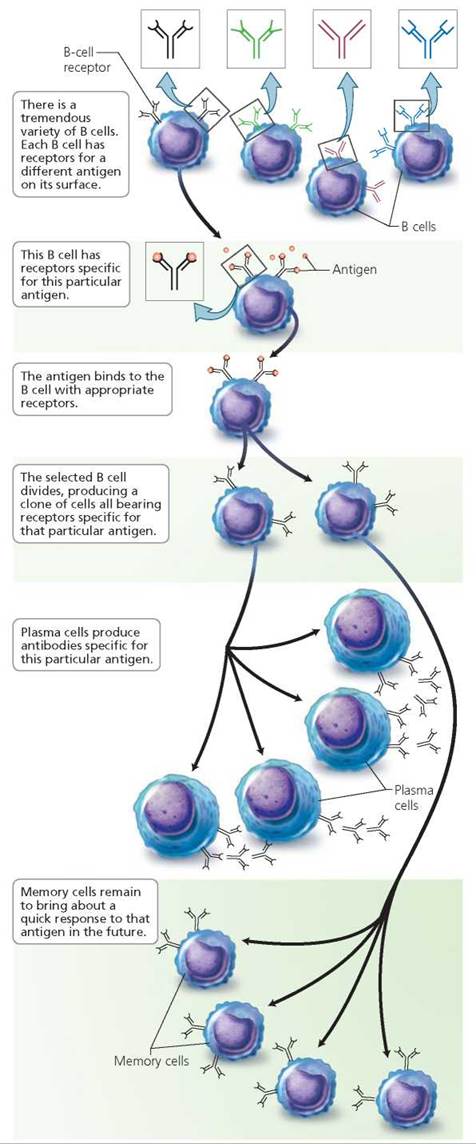
FIGURE 13.11. Clonal selection is the process by which an adaptive immune response to a specific antigen becomes amplified. This figure shows clonal selection of B cells, but a similar process occurs with T cells.
The following analogy may be helpful for understanding clonal selection. Consider a small bakery with only sample cookies on display. A customer chooses a particular cookie and places an order for many cookies of that type. The cookies are then prepared especially for that person. The sample cookies do not take a lot of space, so a wide selection can be on display for other customers to select. The baker does not waste energy making cookies that have not been specifically requested. Your body prepares samples of many kinds of lymphocytes; a given lymphocyte responds to only one antigen. When an antigen selects the appropriate lymphocyte, the body produces many additional copies of the lymphocyte chosen by that particular antigen.
Stop and think
A primary target of HIV, the human immunodeficiency virus that leads to AIDS, is the helper T cell. Why does the virus's preference for the helper T cell impair the immune system more than if another type of lymphocyte were targeted?
We have already mentioned that two types of cells are produced in step 5: memory cells and effector cells. Before turning to the role of memory cells, let's look more closely at exactly how the effector cells protect us.
Defense—The Antibody-Mediated Response. In the antibody- mediated immune response, activated B cells divide. The effector cells they produce through clonal selection, which are called plasma cells, secrete antibodies into the bloodstream to defend against antigens free in the blood or bound to a cell surface (Figure 13.12). Antibodies are Y-shaped proteins that recognize a specific antigen by its shape. Each antibody is specific for one particular antigen. The specificity results from the shape of the proteins that form the tips of the Y (Figure 13.13). Because of their shapes, the antibody and antigen fit together like a lock and a key. Each antibody can bind to two identical antigens, one at the tip of each arm on the Y.
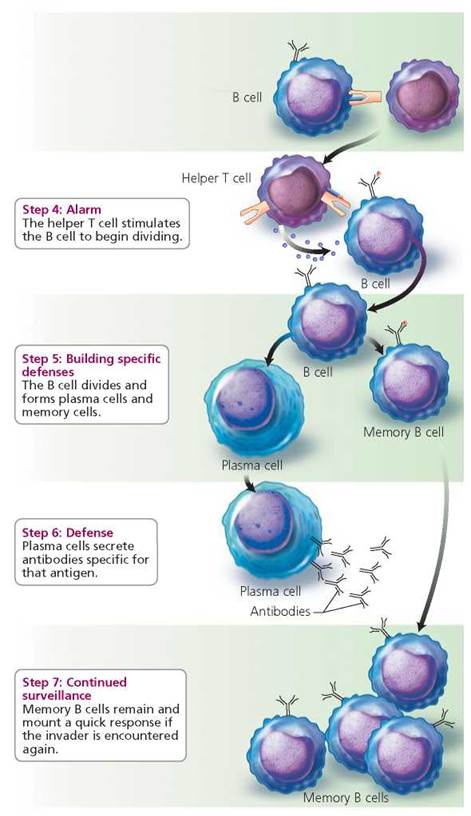
FIGURE 13.12. Antibody-mediated immune response
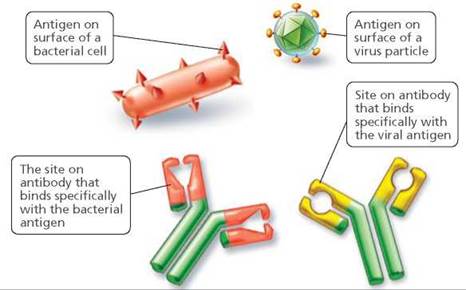
FIGURE 13.13. An antibody is a Y-shaped protein designed to recognize an antigen having a specific shape. The recognition of a specific antigen occurs due to the shape of the tips of the Y in the antibody molecule.
Antibodies can bind only to antigens that are free in body fluids or attached to the surface of a cell. Their main targets are toxins and extracellular microbes, including bacteria, fungi, and protozoans. Antibodies help defend against these pathogens in several ways that can be remembered with the acronym PLAN.
• Precipitation: The antigen-antibody binding causes antigens to clump together and precipitate (settle out of solution), enhancing phagocytosis by making the antigens easier for phagocytic cells to capture and engulf.
• Lysis (bursting): Certain antibodies activate the complement system, which then pokes holes through the membrane of the target cell and causes it to burst.
• Attraction of phagocytes: Antibodies also attract phagocytic cells to the area. Phagocytes then engulf and destroy the foreign material.
• Neutralization: Antibodies bind to toxins and viruses, neutralizing them and preventing them from causing harm.
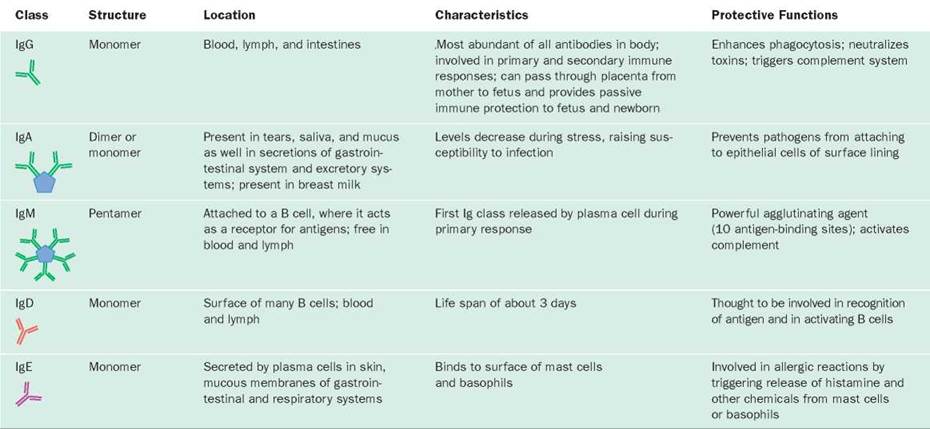
There are five classes of antibodies, each with a special role to play in protecting against invaders. Antibodies are also called immunoglobulins (Ig), and each class is designated with a letter: IgG, IgA, IgM, IgD, and IgE. As you can see in Table 13.4, the antibodies of some classes exist as single Y-shaped molecules (monomers), in one class they exist as two attached molecules (dimers), and in one class they exist as five attached molecules (pentamers) radiating outward like the spokes of a wheel.
TABLE 13.4. Classes of Antibodies
Defense—The Cell-Mediated Response. The cytotoxic T cells are the effector T cells responsible for the cell-mediated immune response that destroys antigen-bearing cells. Each cytotoxic T cell is programmed to recognize a particular antigen bound to MHC markers on the surface of a cellular pathogen, an infected or cancerous body cell, or on cells of a tissue or organ transplant. A cytotoxic T cell becomes activated to destroy a target cell when two events occur simultaneously, as shown in Figure 13.14. First, the cytotoxic T cell must encounter an antigen-presenting cell, such as a macrophage. Second, a helper T cell must release a chemical to activate the cytotoxic T cell. When activated, the cytotoxic T cell divides, producing memory cells and effector cytotoxic T cells.
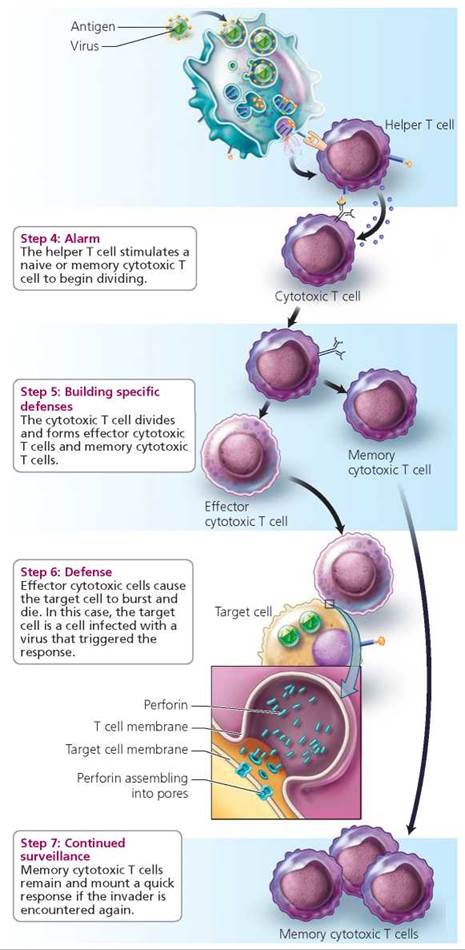
FIGURE 13.14. Cell-mediatedimmuneresponse
An effector cytotoxic T cell releases chemicals called perforins, which cause holes to form in the target cell membrane. The holes are large enough to allow some of the cell's contents to leave the cell so that the cell disintegrates. The cytotoxic T cell then detaches from the target cell and seeks another cell having the same type of antigen.
Stop and think
Rejection of an organ transplant occurs when the recipient's immune system attacks and destroys the cells of the transplanted organ. Why would this attack occur? Which branch of the immune system would be most involved?
Continued Surveillance. The first time an antigen enters the body, only a few lymphocytes can recognize it. Those lymphocytes must be located and stimulated to divide in order to produce an army of lymphocytes ready to eliminate that particular antigen. As a result, the primary response, the one that occurs during the body's first encounter with a particular antigen, is relatively slow. A lapse of several days occurs before the antibody concentration begins to rise, and the concentration does not peak until 1 to 2 weeks after the initial exposure to the antigen (Figure 13.15).
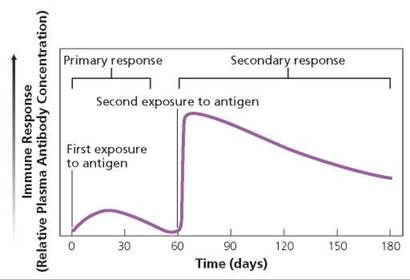
FIGURE 13.15. The primary and secondary immune responses. In the primary response, which occurs after the first exposure to an antigen, there is a delay of several days before the concentration of circulating antibodies begins to increase. It takes 1 to 2 weeks for the antibody concentration to peak because the few lymphocytes programmed to recognize that particular antigen must be located and activated. (The T cells show a similar pattern of response.) The secondary response following a subsequent exposure to an antigen is swifter and stronger than the primary response. The difference is due to the long-lived memory cells produced during the primary response; these are a larger pool of lymphocytes programmed to respond to that particular antigen.
Following subsequent exposure to the antigen, the secondary response is strong and swift. Recall that when naive B cells and T cells were stimulated to divide, not only did they produce effector cells that actively defended against the invader, but they also produced memory cells. These memory B cells, memory cytotoxic T cells, and memory helper T cells live for years or even decades. As a result, the number of lymphocytes programmed to respond to that particular antigen is much greater than it was before the first exposure. When the antigen is encountered again, each of those memory cells divides and produces new effector cells and memory cells specific for that antigen. Therefore, the number of effector cells rises quickly during the secondary response, and within 2 or 3 days reaches a higher peak than it did during the primary response.
Withdrawal of Forces. As the immune system begins to conquer the invading organism and the level of antigens declines, another type of T cell, the suppressor T cell, releases chemicals that dampen the activity of both B cells and T cells. Suppressor T cells turn off the immune response when the antigen no longer poses a threat. This may be a mechanism that prevents the immune system from overreacting and harming healthy body cells.
Active and Passive Immunity
There are two types of immunity: In active immunity the body actively defends itself by producing memory B cells and T cells following exposure to an antigen. Active immunity happens naturally whenever a person gets an infection. Fortunately, active immunity can also develop through vaccination (also known as immunization), a procedure that introduces a harmless form of an antigen into the body to stimulate immune responses against that antigen. Today, some vaccines, such as the vaccine for hepatitis B, are prepared using bacteria that are genetically modified to produce a protein from the pathogen. Since only the protein (antigen) is injected, rather than the actual virus, the vaccine can't cause disease. In some kinds of vaccination—whooping cough and typhoid fever, for instance— the microbe is killed before the vaccine is prepared. Other vaccines must be made from live organisms in order to be effective. In these cases, the microbes are first weakened so that they can no longer cause disease. The microbes are weakened by transferring them repeatedly in tissue culture, which allows unpredictable mutations to occur. Still other vaccines, including the one against smallpox, are prepared from microbes that cause related but milder diseases.
Because it leads to the production of memory cells, active immunity—occurring naturally or via vaccination—is relatively long-lived. The first dose of a vaccine causes the primary immune response, and antibodies and some memory cells are generated. In certain cases, especially when inactivated antigens are used in the vaccine, the immune system may "forget" its encounter with the antigen after a time. A booster is administered periodically to make sure the immune system does not forget. The booster results in a secondary immune response and enough memory cells to provide for a quick response should a potent form of that pathogen ever be encountered.
Vaccinations have saved millions of lives. In fact, they have been so effective in preventing diseases such as whooping cough and tetanus that many people mistakenly think those diseases have been eliminated. However, most of the diseases that vaccines prevent still exist, so vaccinations are still important. Children should be immunized (given vaccines) on a recommended schedule.
Passive immunity is protection that results when a person receives antibodies produced by another person or animal. For instance, some antibodies produced by a pregnant woman can cross the placenta and give the growing fetus some immunity. These maternal antibodies remain in the infant's body for as long 3 months after birth, at which point the infant is old enough to produce its own antibodies. Antibodies in breast milk also provide passive immunity to nursing infants, especially against pathogens that might enter through the intestinal lining. The mother's antibodies are a temporary yet critical blanket of protection, because most of the pathogens that would otherwise threaten the health of a newborn have already been encountered by the mother's immune system.
People can acquire passive immunity medically by being injected with antibodies produced in another person or animal. In this case, passive immunity is a good news-bad news situation. The good news is that the effects are immediate. Gamma globulin, for example, is a preparation of antibodies used to protect people who have been exposed to diseases such as hepatitis B or who are already infected with the microbes that cause tetanus, measles, or diphtheria. Gamma globulin is often given to travelers before they visit a country where viral hepatitis is common. The bad news is that the protection is short-lived. The borrowed antibodies circulate for 3 to 5 weeks before being destroyed in the recipient's body. Because the recipient's immune system was not stimulated to produce memory cells, protection disappears with the antibodies.
Stop and think
The viruses that cause influenza (the flu) mutate rapidly, so the antigens in the protein coat continually change. Why does this characteristic make it difficult to develop a flu vaccine that will be effective for several consecutive years?
What would you do?
There is now a vaccine against the human papillomavirus, a sexually transmitted virus that is also the most important cause of cervical cancer. Health officials recommend the vaccine for girls 11 or 12 years of age, but it can be given to girls as young as 9 years and to women as old as 26 years. Some social conservatives fear that use of this vaccine will encourage vaccinated teenagers to be sexually active. If you were (or are) a parent, would you have your daughter vaccinated? Why or why not?
Monoclonal Antibodies
Suppose you wanted to determine whether a particular antigen was present in a solution, tissue, or even somewhere in the body. An antibody specific for that antigen would be just the tool you would need. Because of its specificity, any such antibody would go directly to the target antigen. If a label (such as a radioactive tag or a molecule that fluoresces) were attached to the antibody, the antibody could reveal the location of the antigen. You can see that for a test of this kind, it is desirable to have a supply of identical antibodies that react with a specific antigen. Groups of identical antibodies that bind to one specific antigen are called monoclonal antibodies.
Monoclonal antibodies have many uses. Home pregnancy tests contain monoclonal antibodies produced to react with a hormone (human chorionic gonadotropin; see Chapter 18) secreted by membranes associated with the developing embryo. Monoclonal antibodies have also proved useful in screening for certain diseases, including Legionnaire's disease, hepatitis, certain sexually transmitted diseases, and certain cancers, including those of the lung and prostate. Some monoclonal antibodies are also used in cancer treatment. The radioactive material or chemical treatment to combat the cancer is attached to a monoclonal antibody that targets the tumor cells but has little effect on healthy cells.
Problems of the Immune System
The immune system protects us against myriad threats from agents not recognized as belonging in the body. However, sometimes the defenses are misguided. In autoimmune disease, the body's own cells are attacked. Allergies result when the immune system protects us against substances that are not harmful. Tissue rejection following organ transplant is also caused by the immune system (see the Health Issue essay, Rejection of Organ Transplants).
Autoimmune Disorders
Autoimmune disorders occur when the immune system fails to distinguish between self and nonself and attacks the tissues or organs of the body. If the immune system can be called the body's military defense, then autoimmune disease is the equivalent of friendly fire.
As we have seen, during their development, lymphocytes are programmed to attack a specific foreign antigen while still tolerating self antigens. Lymphocytes that do not learn to make this distinction are usually destroyed. Unfortunately, some lymphocytes that are primed to attack self antigens escape destruction. These cells are like time bombs ready to attack the body's own cells at the first provocation. For example, if these renegade lymphocytes are activated by a virus or bacterium, they may direct their attack against healthy body cells as well as the invading organism.
Autoimmune disorders are often classified as organ-specific or non-organ-specific. As the name implies, organ-specific autoimmune disorders are directed against a single organ. Organ-specific autoimmune disorders are usually caused by T cells that have gone awry. The thyroid gland, for example, is attacked in Hashimoto's thyroiditis. In contrast, non-organ-specific autoimmune disorders are generally caused by antibodies produced by B cells gone awry and tend to have effects throughout the body. In systemic lupus erythematosus, for instance, connective tissue is attacked. Since connective tissue can be found throughout the body, almost any organ can be affected. Lupus can cause skin lesions or rashes, especially a butterfly-shaped rash centered on the nose and spreading to both cheeks. It may affect the heart (pericarditis), joints (arthritis), kidneys (nephritis), or nervous system (seizures).
A number of autoimmune disorders occur because portions of disease-causing organisms resemble proteins found on normal body cells. If the immune system mistakes the body's antigens for the foreign antigens, it may attack them. For instance, the body's attack on certain streptococcal bacteria that cause a sore throat may result in the production of antibodies that target not only the streptococcal bacteria but also similar molecules that are found in the valves of the heart and joints. The result is an autoimmune disorder known as rheumatic fever.
Treatment of autoimmune disorders is usually two pronged. First, any deficiencies caused by the disorder are corrected. Second, drugs are administered to depress the immune system.
Health Issue
Rejection of Organ Transplants
Each year, tens of thousands of people receive a gift of life in the form of a transplanted kidney, heart, lungs, liver, or pancreas. Although these transplants seem almost commonplace today, they have been performed for only about 30 years. Before organ transplants could be successful, physicians had to learn how to prevent the effector T cells of the immune system from attacking and killing the transplanted tissue because it lacked appropriate self markers. When transplanted tissue is killed by the host's immune system, we say that the transplant has been rejected.
The success of a transplant depends on the similarity between the host tissues and the transplanted tissues. The most successful transplants are those in which tissue is taken from one part of a person's body and transplanted to another part. In cases of severe burns, for example, healthy skin from elsewhere on the body can replace badly burned areas of skin.
Another way to increase the likelihood that a transplant will be accepted is to use cells from the person's body to grow the transplant in a laboratory. Today, it is possible to grow some organs, urinary bladders for instance, in the laboratory. Cells are taken from the defective organ and grown in tissue culture. When there are enough cells, they are placed on a 3-D model of the organ. Then the cell-covered mold is incubated until the new organ is formed. We discuss laboratory-grown organs in more detail in Chapter 19a.
Because identical twins are nearly genetically identical, their cells have the same self markers, and organs can be transplanted from one twin to another with little fear of tissue rejection. But few of us have an identical twin. The next best source for tissue for a transplant, and the most common, is a person whose cell surface markers closely match those of the host. Usually the transplanted tissue comes from a person who has recently died. The donor is usually brain-dead, but his or her heart is kept beating by life-support equipment. Some organs—primarily kidneys—can be harvested from someone who has died and whose heart has stopped beating. In some cases, living people can donate organs; one of two healthy kidneys can be donated to a needy recipient, as can sections of liver.
The odds in favor of a successful transplant are always improving, and so the waiting list of patients in need of an organ from a suitable donor has outpaced the supply. Some researchers believe that in the future, organs from nonhuman animals may fill the gap between the supply of organs and the demand. So far, however, attempts to transplant animal organs into people have failed. The biggest obstacle is hyperacute rejection. Within minutes to hours after transplant, the animal organ dies because its blood supply is choked off by the human immune system.
Other dangers may remain, even if the rejection problem is solved. Animals carry infectious agents that are harmless to their hosts but that might “jump species” and then gain the ability to spread from the transplant recipient to another person. If that were possible, we would have to ask whether it is ethical to expose a third party to risk.
Questions to Consider
• If you are a tissue match for someone who needs a kidney or a bone marrow transplant, how would you decide whether to be a donor?
• Do you think that family members who are a tissue match should be obligated to donate a kidney or bone marrow?
• Do you think that people should be able to buy a kidney or bone marrow from a suitable donor?
Allergies
An allergy is an overreaction by the immune system to an antigen, in this case called an allergen. The immune response in an allergy is considered an overreaction because the allergen itself usually is not harmful to the body. The most common allergy is hay fever—which, by the way, is not caused by hay and does not cause a fever. Hay fever is more correctly known as allergic rhinitis (rhino, nose; -itis, inflammation of). The symptoms of hay fever—sneezing and nasal congestion— occur when an allergen is inhaled, triggering an immune response in the respiratory system. Mucous membranes of the eyes may also respond, causing red, watery eyes. Common causes of hay fever include pollen, mold spores, animal dander, and the feces of dust mites—microscopic creatures that are found throughout your home (Figure 13.16). The same allergens, however, can trigger asthma. During an asthma attack, the small airways in the lung (bronchioles) constrict, making breathing difficult. In food allergies, the immune response occurs in the digestive system and may cause nausea, vomiting, abdominal cramps, and diarrhea. Food allergies can also cause hives, a skin condition in which patches of skin temporarily become red and swollen.

FIGURE 13.16. Common causes of allergies are pollen grains and the feces of dust mites, such as the mite shown here.
An immediate allergic response begins when a person is exposed to an allergen and a primary immune response is launched (Figure 13.17). Soon, plasma cells churn out the antibody IgE, which binds to either basophils or mast cells. In subsequent exposures to that allergen, the allergen binds to IgE antibodies on the surface of basophils or mast cells and causes granules within the cells to release their contents: histamine.
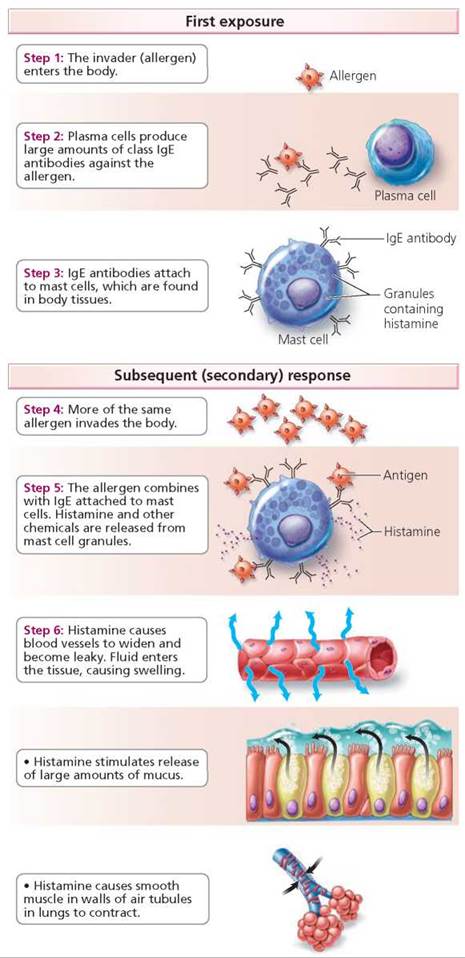
FIGURE 13.17. Steps in an allergic reaction
Histamine then causes the swelling, redness, and other symptoms of an allergic response. The blood vessels widen, slowing blood flow and causing redness. At the same time, the blood vessels become leaky, allowing fluid to flow from the vessels into spaces between tissue cells, swelling the tissues. Histamine also causes the release of large amounts of mucus, so the nose begins to run. In addition, histamine can cause smooth muscles of internal organs to contract. Thus, if the allergen is in the respiratory system, histamine can trigger an asthma attack by causing the air tubules to contract. If the allergen moves from the area where it entered the body, these effects can be widespread. The result can be anaphylactic shock.
Anaphylactic shock is an extreme allergic reaction that occurs within minutes after exposure to the substance a person is allergic to. It can cause pooling of blood in capillaries, which leads to dizziness, nausea, and sometimes unconsciousness as well as extreme difficulty in breathing. Anaphylactic shock can be fatal, but most people survive. Allergies that are common triggers of anaphylactic shock include certain foods; medicines, including antibiotics such as penicillin; and insect stings, especially stings from bees, wasps, yellow jackets, and hornets.
People with allergies often know which substances cause their problems. When the culprits are not known, doctors can identify them using a crude but effective technique in which small amounts of suspected allergens are injected into the skin. If the person is allergic to one of the suspected allergens, a red welt will form at the site of injection.
If you know you have an allergy, the simplest way to avoid the miseries of an allergic reaction is to avoid exposure to the substances that cause problems. During pollen season, spend as much time as possible indoors, using an air conditioner to filter pollen out of the incoming air. Unfortunately, spores from molds growing in air conditioners and humidifiers are also common triggers of allergies. Some common allergy-causing foods, for instance, strawberries or shellfish, may be easy to avoid. Others, such as peanut oil, can show up in some unlikely dishes, including stew, chili, baked goods, or meat patties.
Certain drugs may reduce allergy symptoms. As their name implies, antihistamines block the effects of histamine. Antihistamines are most effective if they are taken before the allergic reaction begins. Unfortunately, allergies tend to become less susceptible to antihistamines over time, and most antihistamines cause drowsiness, which can impair performance on the job or in school and can make driving a car extremely hazardous.
Some allergies can be treated by gradually desensitizing the person to the offending allergens. Allergy shots containing gradually increasing amounts of a known allergen are injected into the person's bloodstream. During this treatment, the allergen causes the production of another class of antibodies—IgG. Afterward, when the allergen enters the body, IgG antibodies bind to it and prevent it from binding to IgE antibodies on mast cells and triggering an allergic reaction.
Looking ahead
In this chapter, we learned about the mechanisms that protect us against harmful organisms and substances. In the next chapter, we consider some infectious organisms that cause disease.
_________________________________________________________
1 A "naive" cell is one that has been programmed to respond to a particular antigen but has not been previously activated to respond.
Highlighting the Concepts
The Body's Defense System (p. 239)
• The targets of the body's defense system include anything that is not recognized as belonging in the body, such as disease- causing organisms and cancerous cells. These foreign agents are called pathogens.
Three Lines of Defense (pp. 240-245)
• The first line of defense is innate—nonspecific physical barriers, such as skin and mucous membranes, and chemical barriers, such as sweat, oil, tears, and saliva, all of which prevent entry of pathogens.
• The second line of innate defense includes defensive cells and proteins, inflammation, and fever. Defensive cells include phagocytes, eosinophils, and natural killer cells. Two types of defensive proteins are antiviral interferons and complement, which cause cells to burst.
• The inflammatory response occurs as a result of tissue injury or invasion by foreign microbes. It begins when mast cells in the injured area release histamine, which increases blood flow by dilating blood vessels to the region and by increasing the permeability of capillaries there. Increased blood flow causes redness and warmth in the region. Fluid leaking from the capillaries causes swelling.
• Fever, an abnormally high body temperature, helps the body fight invading microbes by enhancing several body defense mechanisms and slowing the growth of many pathogens.
• The third line of defense, the adaptive immune response, targets specific pathogens. The immune system has memory.
Distinguishing Self from Nonself (p. 245)
• All body cells are labeled with proteins called major histocompatibility complex (MHC) proteins, which serve as self markers. Cells that lack self markers (MHC) are considered nonself and are attacked. A nonself substance or organism triggers an immune response and is called an antigen.
• Lymphocytes are white blood cells that are responsible for immune responses. Both B lymphocytes (B cells) and T lymphocytes (T cells) develop in the bone marrow. The B cells are thought to mature in the bone marrow, but the T cells mature in the thymus gland. During maturation, B cells and T cells develop receptors on their surfaces that allow each of those cells to recognize an antigen of a different shape.
• When an antigen is detected, B cells and T cells with receptors that respond to that antigen divide repeatedly, forming effector cells that destroy the antigen and forming memory cells that remain in the body over years or even decades to provide a quick response on subsequent exposure to that antigen.
Antibody-Mediated Responses and Cell-Mediated Responses(pp. 245-246)
• The antibody-mediated immune response and the cell-mediated immune response simultaneously defend against the same antigen.
Steps of the Adaptive Immune Response (pp. 247-251)
• Macrophages are phagocytic cells that engulf any foreign material or organism they encounter. After engulfing the material, the macrophage places a part of the destroyed substance on its own surface to serve as an antigen that alerts lymphocytes to the presence of an invader and reveals what the invader looks like. Macrophages also have molecular (MHC) markers on their membranes that identify them as belonging in the body, that is, as self.
• A macrophage then presents the antigen to a helper T cell, which serves as the main switch to the entire immune response. When this encounter occurs, the macrophage secretes a chemical that activates the helper T cell. The helper T cell, in turn, secretes a chemical that activates the appropriate B cells and T cells (those specific for the antigen that the macrophage engulfed).
• B cells are responsible for antibody-mediated immune responses, which defend against antigens that are free in body fluids, including bacteria, free virus particles, and toxins. When called into action by a helper T cell, a B cell divides repeatedly, forming two lines of descendant cells: effector cells that transform into plasma cells and memory B cells. Plasma cells secrete Y-shaped proteins called antibodies into the bloodstream. Antibodies bind to the particular antigen and inactivate it or help remove it from the body.
• Cytotoxic T cells are responsible for cell-mediated immune responses, which are effective against cellular threats, including infected body cells and cancer cells. When a T cell is activated, it divides, forming two lines of descendant cells: effector cells, called cytotoxic T cells, and memory T cells. Cytotoxic T cells secrete perforins that poke holes in the foreign or infected cell, causing it to burst and die.
• After the first encounter with a particular antigen, the primary response is initiated, which may take several weeks to become effective against the antigen. However, because of memory cells, a subsequent exposure to the same antigen triggers a quicker response, called a secondary response.
• Suppressor T cells dampen the activity of B cells and T cells when antigen levels begin to fall.
Active and Passive Immunity (pp. 251-252)
• In active immunity, the body actively participates in forming memory cells to defend against a particular antigen. Active immunity may occur when an antigen infects the body, or it may occur through vaccination, a procedure that introduces a harmless form of an antigen into the body.
• Passive immunity results when a person receives antibodies that were produced by another person or animal. Passive immunity is short-lived.
Monoclonal Antibodies (p. 252)
• Monoclonal antibodies are identical antibodies that bind to a specific antigen. They are useful in research and in the diagnosis and treatment of diseases.
Problems of the Immune System (pp. 252-255)
• Autoimmune disorders occur when the immune system mistakenly attacks the body's own cells.
• An allergy is a strong immune response against an antigen (called an allergen). An allergy occurs when the allergen binds to IgE antibodies on the surface of mast cells or basophils, causing them to release histamine. Histamine, in turn, causes the redness, swelling, itching, and other symptoms of an allergic response.
Reviewing the Concepts
1. Explain the difference between innate nonspecific and adaptive specific defense mechanisms. p. 240
2. List seven types of nonspecific defense mechanisms. Explain how each type helps protect us against disease. pp. 240-243
3. How does a natural killer cell kill its target cell? pp. 241-242
4. What are interferons? What type of cell produces them? How do they help protect the body? p. 242
5. What is the complement system? Explain how it acts directly and indirectly to protect the body against disease. p. 242
6. Signs of inflammation include redness, warmth, swelling, and pain. What causes each of these symptoms? How does inflammation help defend against infection? pp. 242-243
7. What does an antigen-presenting cell do? How do other cells recognize the antigen-presenting cell as a "friend"? p. 247
8. What cells are responsible for antibody-mediated immune responses? What are the targets of antibody-mediated immune responses? p. 249
9. Describe an antibody. How do antibodies inactivate or eliminate antigens from the body? p. 249
10. What is responsible for cell-mediated immune responses? What are the targets of cell-mediated immune responses? pp. 249-250
11. How does a natural killer cell differ from a cytotoxic T cell? pp. 241, 249-250
12. Why does a secondary response occur more quickly than the primary response? pp. 250-251
13. Differentiate between active and passive immunity. pp. 251-252
14. What are monoclonal antibodies? What are some medical uses for them? p. 252
15. What is an autoimmune disorder? pp. 252-253
16. What is an allergy? What causes the symptoms? pp. 253-255
17. Indicate the correct statement:
a. An antibody is specific to one particular antigen.
b. Antibodies are held within the cell that produces them.
c. Antibodies are produced by macrophages.
d. Antibodies can be effective against viruses that are inside the host cell.
18. An antigen is a
a. cell that produces antibodies.
b. receptor on the surface of a lymphocyte that recognizes invaders.
c. memory cell that causes a quick response to an invader when it is encountered a second time.
d. large molecule on the surface of an invader that triggers an immune response.
19. Indicate the choice with the incorrect pairing of cell type and function.
a. Helper T cell—serves as "main switch" that activates both the cell-mediated immune responses and the antibody- mediated immune responses
b. Cytotoxic T cell—presents antigen to the helper T cell
c. Macrophage—roams the body looking for invaders, which are engulfed and digested when they are found
d. Suppressor T cell—shuts off the immune response when the invader has been removed
20. When the doctors say they are looking for a suitable donor for a kidney transplant, they are looking for someone
a. whose tissues have self markers similar to those of the recipient.
b. who lacks antibodies to the recipient's tissues.
c. who has suppressor T cells that will suppress the immune response against the donor kidney.
d. who lacks macrophages.
21. The piece of the antigen displayed on the surface of a macrophage
a. stimulates the suppressor T cells to begin dividing.
b. attracts other invaders to the cell, causing them to accumulate and making it easier to kill the invaders.
c. informs the other cells in the immune system of the exact nature of the antigen they should be looking for (what the antigen "looks like").
d. has no function in the immune response.
22. A cell that kills any unrecognized cell in the body and is part of the nonspecific body defenses is a(n) _____.
23. _____ is a chemical released by mast cells and basophils that produces most of the symptoms of an allergy.
24. Antibodies are produced by _____.
25. _____ are important antigen-presenting cells.
Applying the Concepts
1. After being exposed to the hepatitis B virus, Barbara goes to the doctor and asks to be vaccinated against it. Instead, the doctor gives her an injection of gamma globulin (a preparation of antibodies). Why wasn't she given the vaccine?
2. More than 100 viruses can cause the common cold. How does this fact explain why you can catch a cold from Raymond immediately after recovering from a cold you caught from Jessica?
3. HIV is a virus that kills helper T cells. This virus is not the direct cause of death in people who are infected with it. Instead, people die of diseases caused by organisms that are common in the environment. Explain why HIV-infected persons are susceptible to these diseases.
4. Ira found a deer tick attached to the back of his leg. He knows that deer ticks can transmit the bacterium that causes Lyme disease and that untreated Lyme disease can cause arthritis and fatigue. He immediately went to the doctor to get tested, which would involve drawing blood to look for antibodies to the bacterium. The doctor refused to test Ira for Lyme disease. Why?
5. Rashon has leukemia, a cancer in which the number of white blood cells increases dramatically. The doctors decide that a bone marrow transfer might help by replacing defective bone stem cells with healthy ones. His girlfriend offered to be a donor, but the doctors chose his brother instead. Why? Why was Rashon given drugs to suppress his immune system after the transplant?
Becoming Information Literate
1. Vaccination has reduced or eliminated many diseases that were killers, including diphtheria, typhoid, polio, and smallpox. The Centers for Disease Control and Prevention (CDC) has a recommended schedule for childhood immunization. Yet some parents don't have their children vaccinated.
If you were or are a parent, would you have your child vaccinated according to the recommended schedule? Write a few paragraphs that include the benefits and potential risks of vaccination. Explain how and why you made your decision.
Use at least three reliable sources (books, journals, or websites) to gather information that would help you decide. List each source you considered, and explain why you chose the three sources you used.
2. AIDS is an immune deficiency disease that is occurring in epidemic proportions in Africa. Write a few paragraphs describing the African AIDS crisis and strategies for relieving the crisis.
Use at least three reliable sources (books, journals, or websites) to gather information. List each source you considered, and explain why you chose the three sources you used.